Current Issue
Display Method: |
2026, 38(3): 289-290.
doi: 10.21147/j.issn.1000-9604.2026.03.01
 Abstract
Abstract FullText HTML
FullText HTML PDF 843KB
PDF 843KB
Abstract:
2026, 38(3): 295-297.
doi: 10.21147/j.issn.1000-9604.2026.03.03
Abstract:
2026, 38(3): 298-300.
doi: 10.21147/j.issn.1000-9604.2026.03.04
Abstract:
2026, 38(3): 301-303.
doi: 10.21147/j.issn.1000-9604.2026.03.05
Abstract:
2026, 38(3): 304-306.
doi: 10.21147/j.issn.1000-9604.2026.03.06
Abstract:
2026, 38(3): 307-310.
doi: 10.21147/j.issn.1000-9604.2026.03.07
Abstract:
2026, 38(3): 315-328.
doi: 10.21147/j.issn.1000-9604.2026.03.09
Abstract:
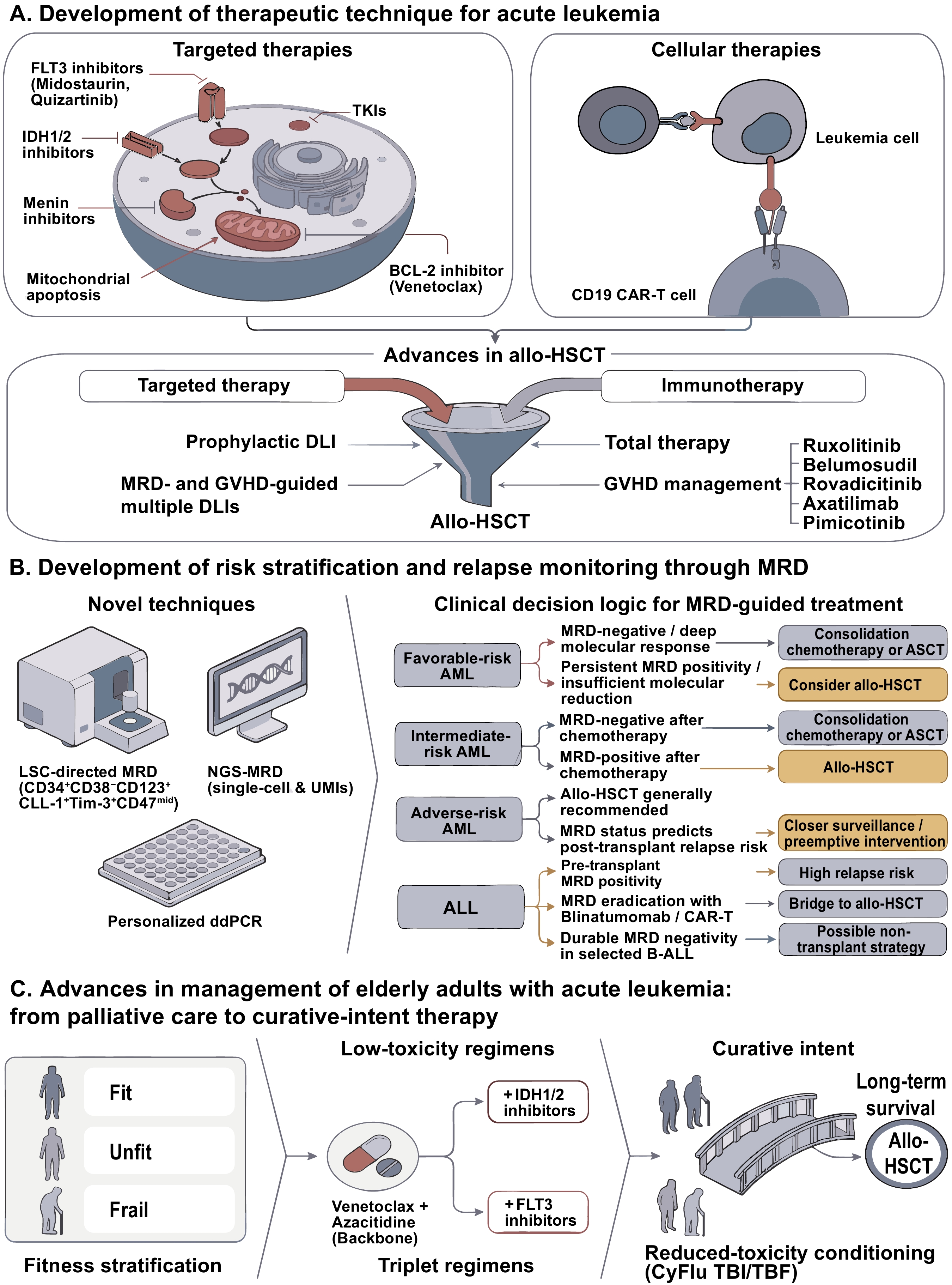
Acute leukemia remains a life-threatening hematologic malignancy with historically poor outcomes in relapsed/refractory and elderly patients. Over the past decade, measurable residual disease (MRD) has evolved from a prognostic indicator to a core determinant of risk stratification and clinical decision-making, driving a paradigm shift toward precision medicine. Technological innovations—including leukemia stem cell (LSC)-directed MRD detection, single-cell sequencing, and personalized digital polymerase chain reaction (PCR)—have markedly improved the sensitivity and specificity of MRD monitoring, enabling the early identification of patients at ultrahigh risk of relapse. Concurrently, targeted therapy has moved from salvage to frontline standard care; the use of FLT3, IDH1/2, and BCR-ABL1 inhibitors combined with chemotherapy or immunotherapy has significantly prolonged remission, improved MRD negativity rates, and redefined prognostic stratification. Novel cellular therapies, particularly CD19/CD22-targeted chimeric antigen receptor T (CAR-T) and bispecific T-cell engagers, have revolutionized the treatment of relapsed/refractory B-cell acute lymphoblastic leukemia, and allogeneic hematopoietic stem cell transplantation (allo-HSCT), optimized by the “Beijing Protocol” for haploidentical donors, remains the cornerstone of curative intent. Low-toxicity regimens, such as venetoclax plus hypomethylating agents, have transformed care for elderly or unfit patients, shifting goals from palliation to long-term survival. Despite these advances, challenges, including antigen escape, CAR-T-cell persistence, graft-versus-host disease, and treatment accessibility, persist. This commentary summarizes landmark progress in MRD-guided precision stratification, targeted therapy, cellular immunotherapy, and allo-HSCT; discusses unresolved clinical bottlenecks; and proposes future directions centered on dynamic MRD monitoring, personalized targeted-immunotherapy combinations, and risk-adapted transplantation strategies to further improve cure rates and long-term survival across all acute leukemia subtypes.
Acute leukemia remains a life-threatening hematologic malignancy with historically poor outcomes in relapsed/refractory and elderly patients. Over the past decade, measurable residual disease (MRD) has evolved from a prognostic indicator to a core determinant of risk stratification and clinical decision-making, driving a paradigm shift toward precision medicine. Technological innovations—including leukemia stem cell (LSC)-directed MRD detection, single-cell sequencing, and personalized digital polymerase chain reaction (PCR)—have markedly improved the sensitivity and specificity of MRD monitoring, enabling the early identification of patients at ultrahigh risk of relapse. Concurrently, targeted therapy has moved from salvage to frontline standard care; the use of FLT3, IDH1/2, and BCR-ABL1 inhibitors combined with chemotherapy or immunotherapy has significantly prolonged remission, improved MRD negativity rates, and redefined prognostic stratification. Novel cellular therapies, particularly CD19/CD22-targeted chimeric antigen receptor T (CAR-T) and bispecific T-cell engagers, have revolutionized the treatment of relapsed/refractory B-cell acute lymphoblastic leukemia, and allogeneic hematopoietic stem cell transplantation (allo-HSCT), optimized by the “Beijing Protocol” for haploidentical donors, remains the cornerstone of curative intent. Low-toxicity regimens, such as venetoclax plus hypomethylating agents, have transformed care for elderly or unfit patients, shifting goals from palliation to long-term survival. Despite these advances, challenges, including antigen escape, CAR-T-cell persistence, graft-versus-host disease, and treatment accessibility, persist. This commentary summarizes landmark progress in MRD-guided precision stratification, targeted therapy, cellular immunotherapy, and allo-HSCT; discusses unresolved clinical bottlenecks; and proposes future directions centered on dynamic MRD monitoring, personalized targeted-immunotherapy combinations, and risk-adapted transplantation strategies to further improve cure rates and long-term survival across all acute leukemia subtypes.
2026, 38(3): 329-335.
doi: 10.21147/j.issn.1000-9604.2026.03.10
Abstract:
2026, 38(3): 336-339.
doi: 10.21147/j.issn.1000-9604.2026.03.11
Abstract:
2026, 38(3): 340-342.
doi: 10.21147/j.issn.1000-9604.2026.03.12
Abstract:
2026, 38(3): 343-346.
doi: 10.21147/j.issn.1000-9604.2026.03.13
Abstract:
2026, 38(3): 347-364.
doi: 10.21147/j.issn.1000-9604.2026.03.14
Abstract:
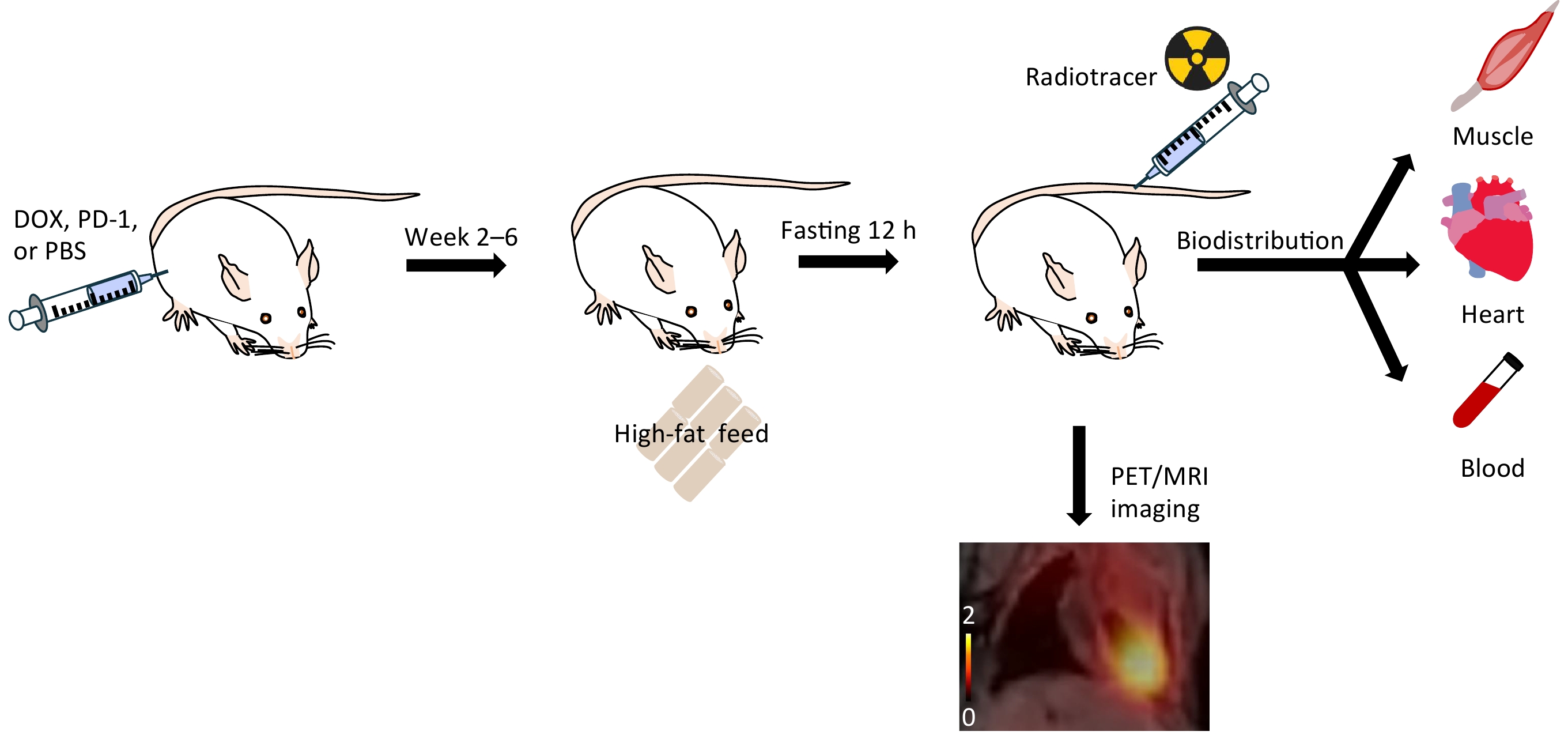
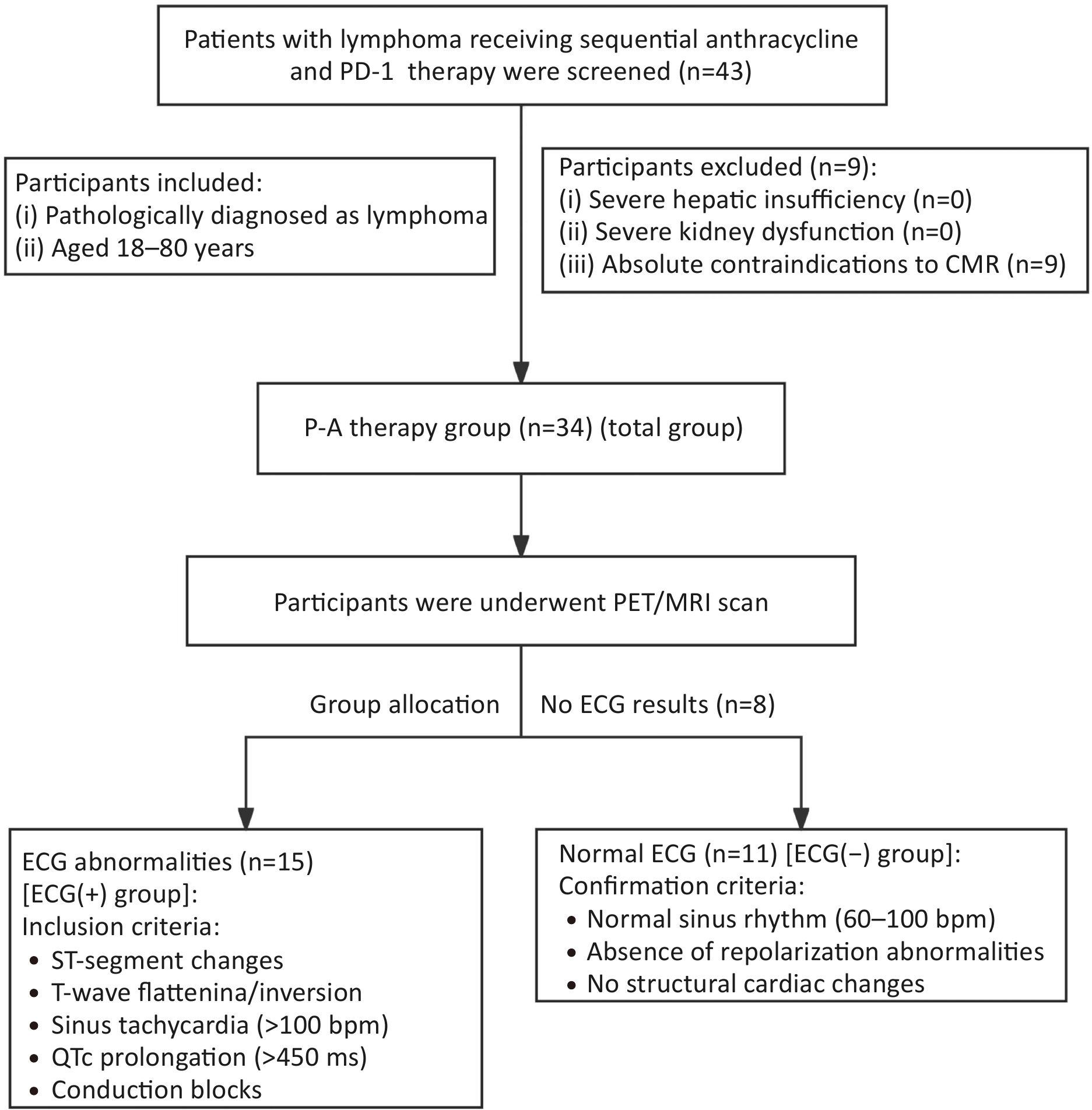
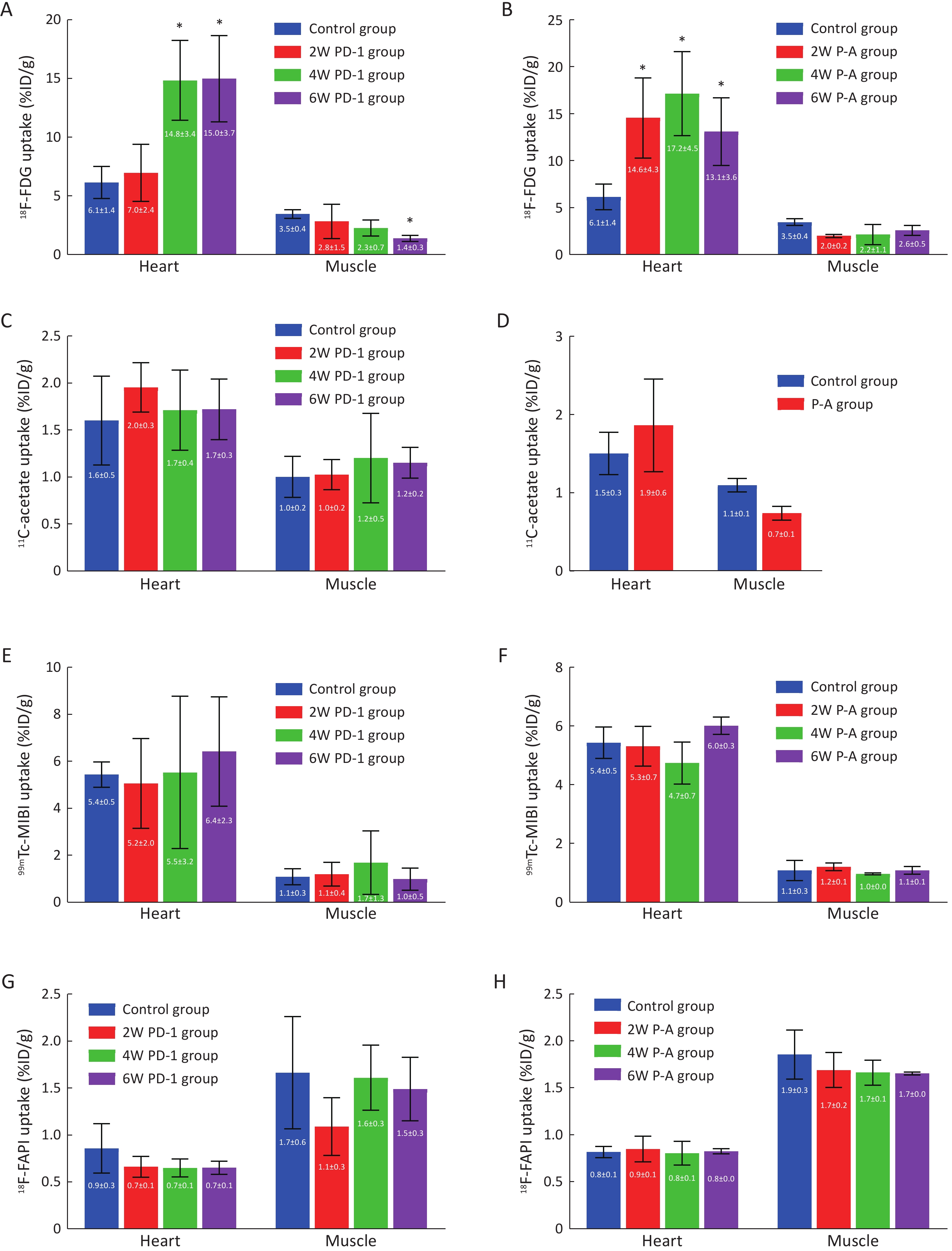
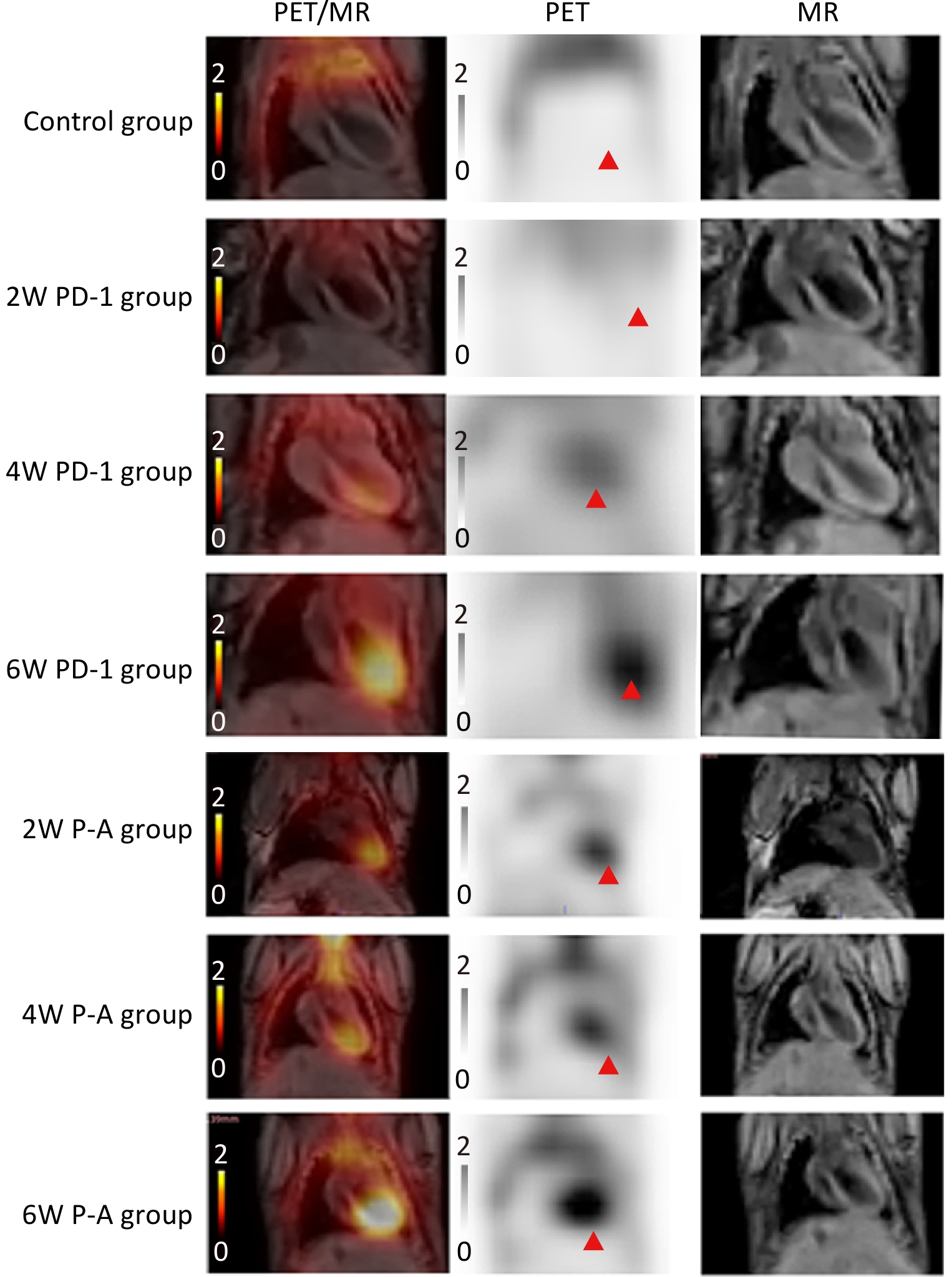
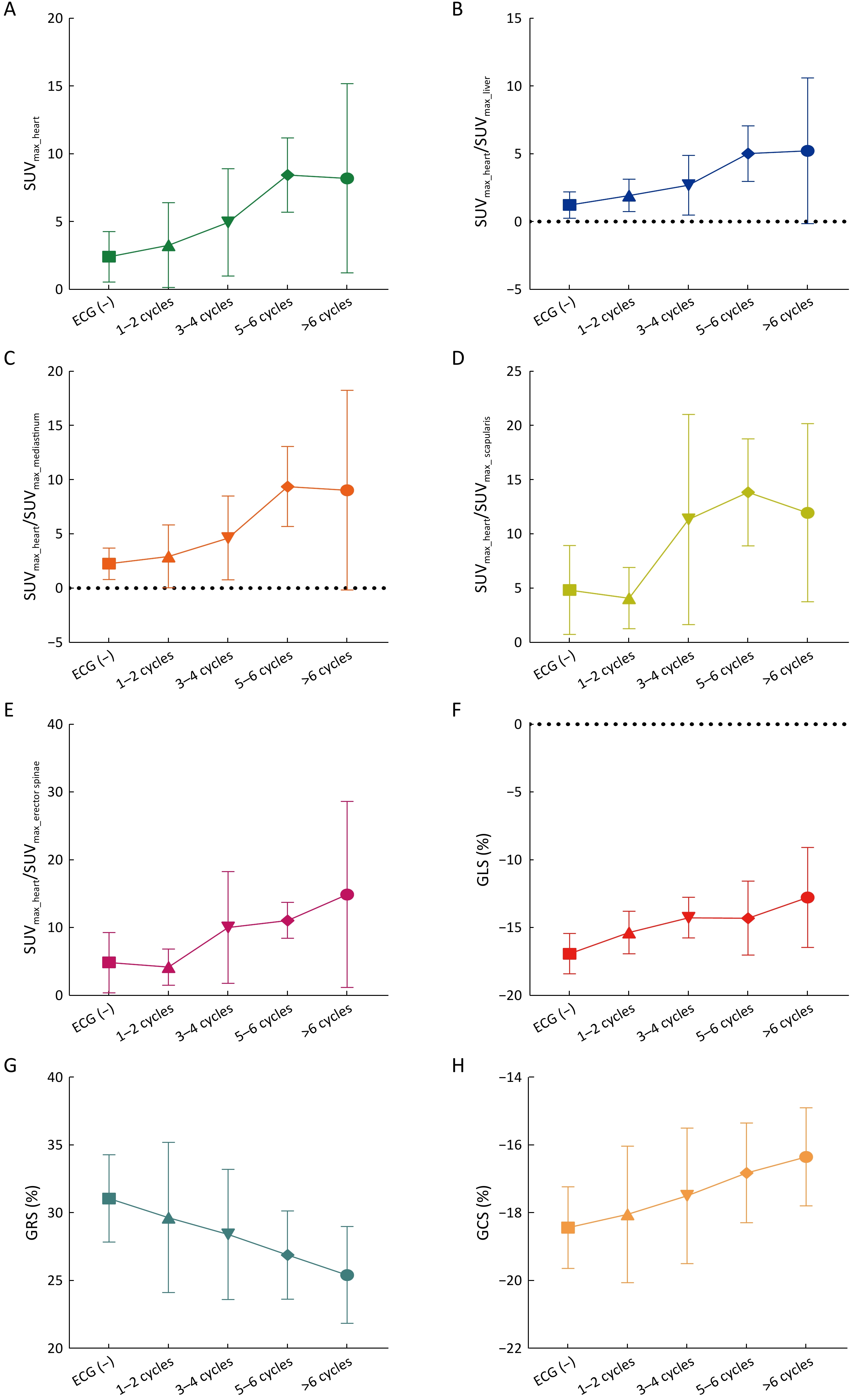
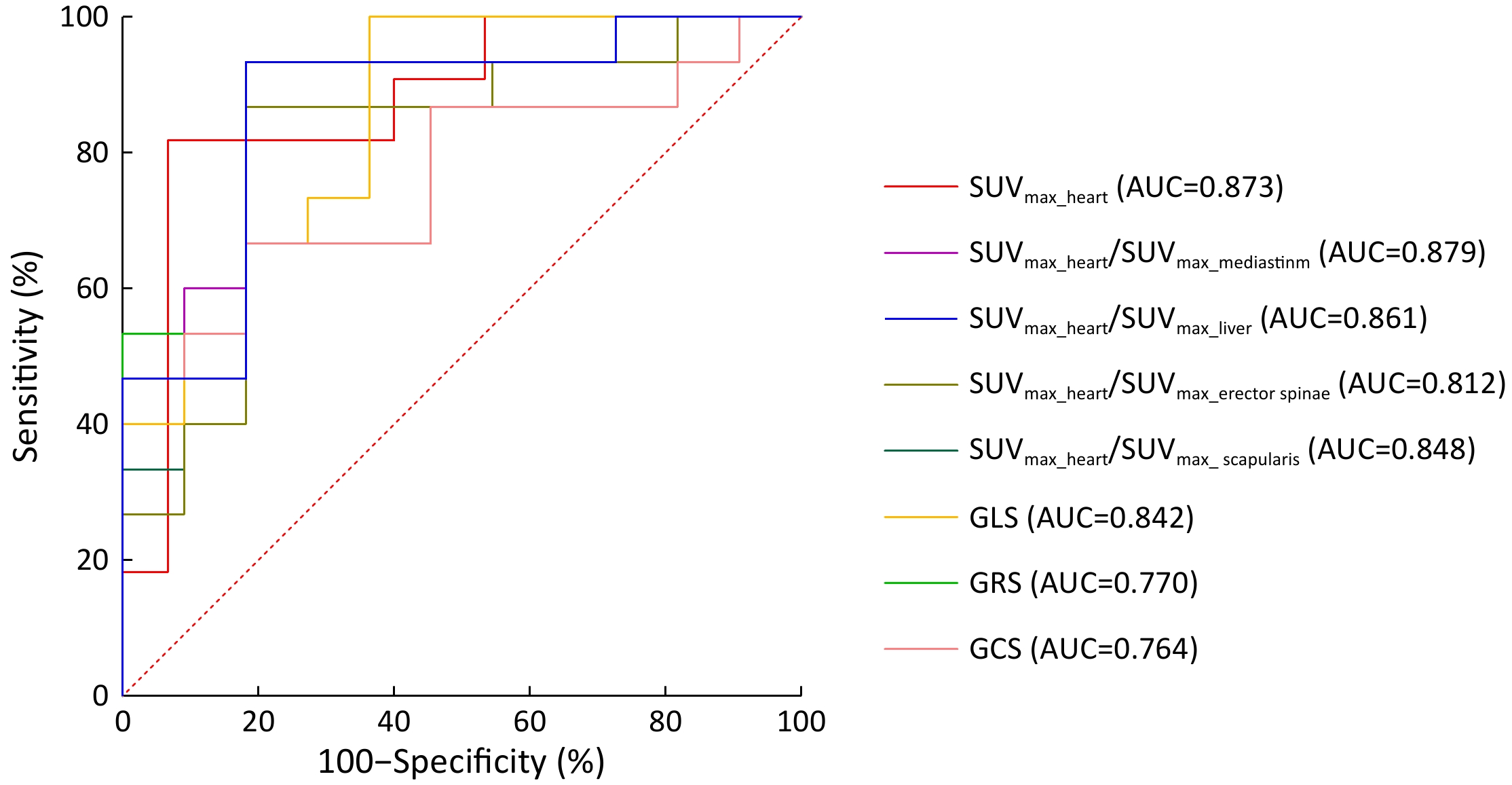
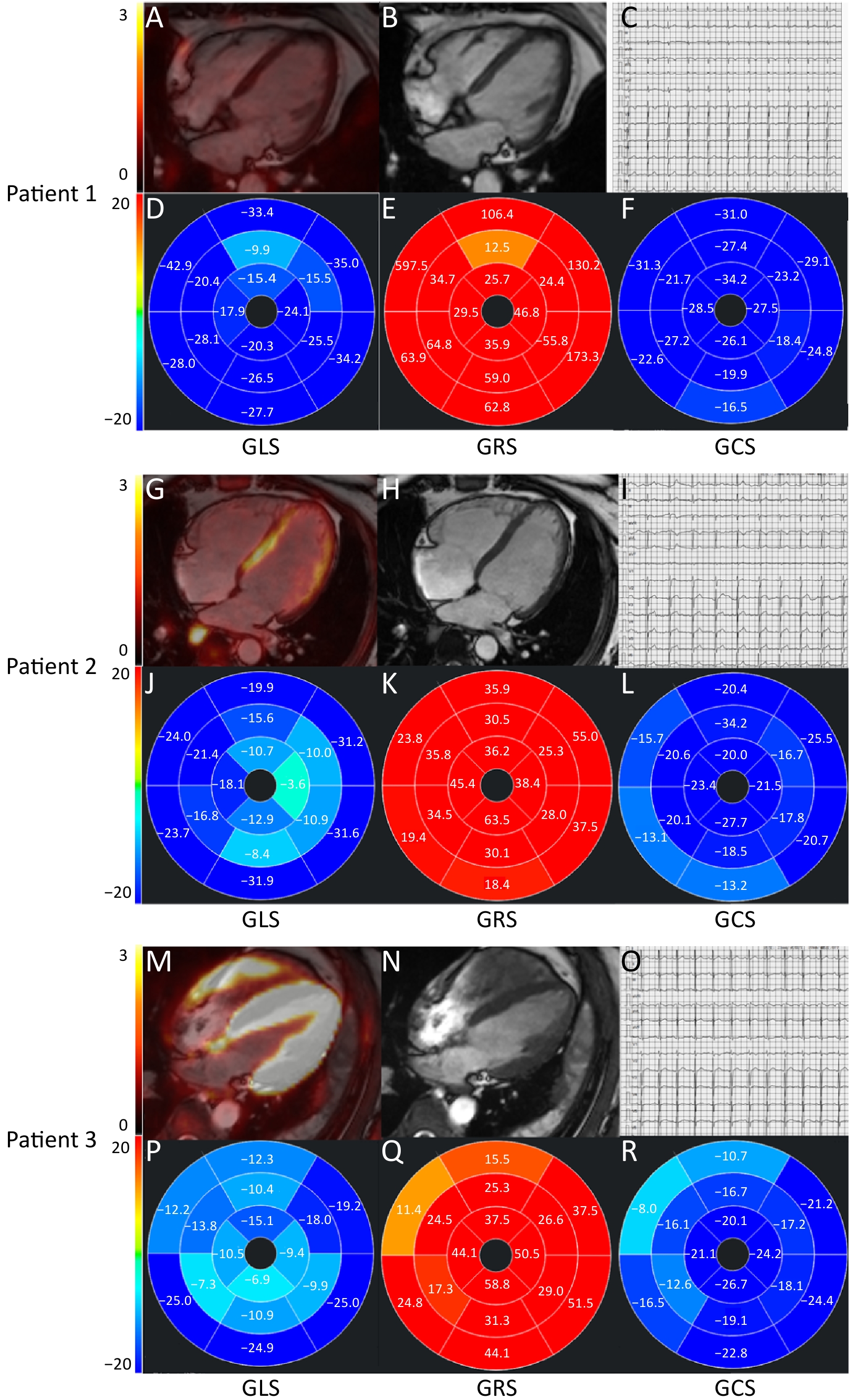
ObjectiveEarly detection of synergistic cardiotoxicity induced by sequential anthracycline and programmed cell death protein 1 (PD-1) inhibitor therapy remains challenging because conventional assessments identify late-stage functional impairment. This study aimed to determine the sensitive imaging probe for early therapy-associated cardiotoxicity and validate findings using integrated positron emission tomography/magnetic resonance imaging (PET/MRI). MethodsCardiotoxicity was assessed in mouse models treated with PD-1 inhibitor or sequential doxorubicin (DOX) and PD-1 inhibitor therapy. Serial biodistribution analyses of 18F-fluorodeoxyglucose (18F-FDG), 18F-fibroblast activation protein inhibitor (18F-FAPI), 99mTc-methoxyisobutylisonitrile (99mTc-MIBI), and 11C-acetate were performed. Histopathological evaluation assessed inflammation, mitochondrial injury, and fibrosis. Findings were validated in a prospective lymphoma cohort receiving sequential anthracycline and PD-1 inhibitor therapy using integrated 18F-FDG PET/MRI. Myocardial maximum standardized uptake value (SUVmax), strain parameters, tissue mapping indices, and electrocardiographic (ECG) changes were analyzed. ResultsSequential DOX and PD-1 inhibitor therapy induced an early increase in myocardial 18F-FDG uptake in mice before preceding systolic dysfunction. Histopathological examination confirmed inflammatory cell infiltration and mitochondrial swelling without extracellular matrix remodeling. In contrast, uptake of 18F-FAPI, 99mTc-MIBI, and 11C-acetate remained unchanged. In patients with lymphoma, myocardial SUVmax was significantly higher in patients with ECG abnormalities [ECG(+)] than in those without ECG abnormalities [ECG(−)], whereas global longitudinal strain, global radial strain, and global circumferential strain were significantly reduced (all P<0.05). After the third PD-1 cycle, myocardial SUVmax remained elevated in ECG(+) patients, whereas strain parameters declined after 5−6 cycles, suggesting that metabolic alterations precede functional impairment. SUVmax_heart demonstrated the highest diagnostic accuracy for cardiotoxicity [cutoff=3.0; area under the curve (AUC)=0.873; sensitivity=93.3%; specificity=80.0%]. ConclusionsCardiac 18F-FDG PET/MRI enables early detection of synergistic cardiotoxicity induced by DOX and PD-1 inhibitors before structural or functional deterioration occurs. SUVmax_heart may serve as an imaging biomarker for risk stratification and timely cardioprotective intervention.

2026, 38(3): 365-378.
doi: 10.21147/j.issn.1000-9604.2026.03.15
Abstract:
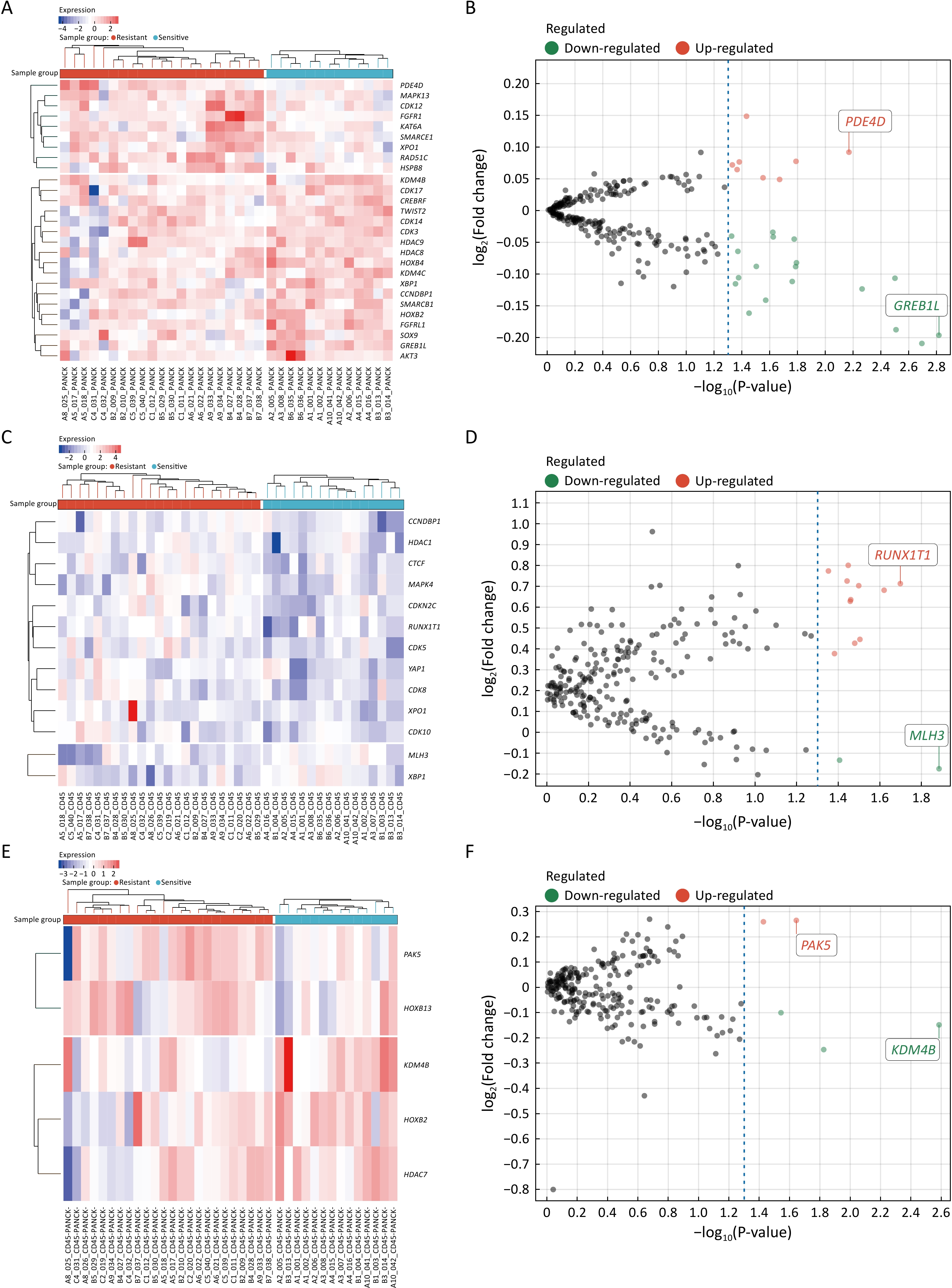
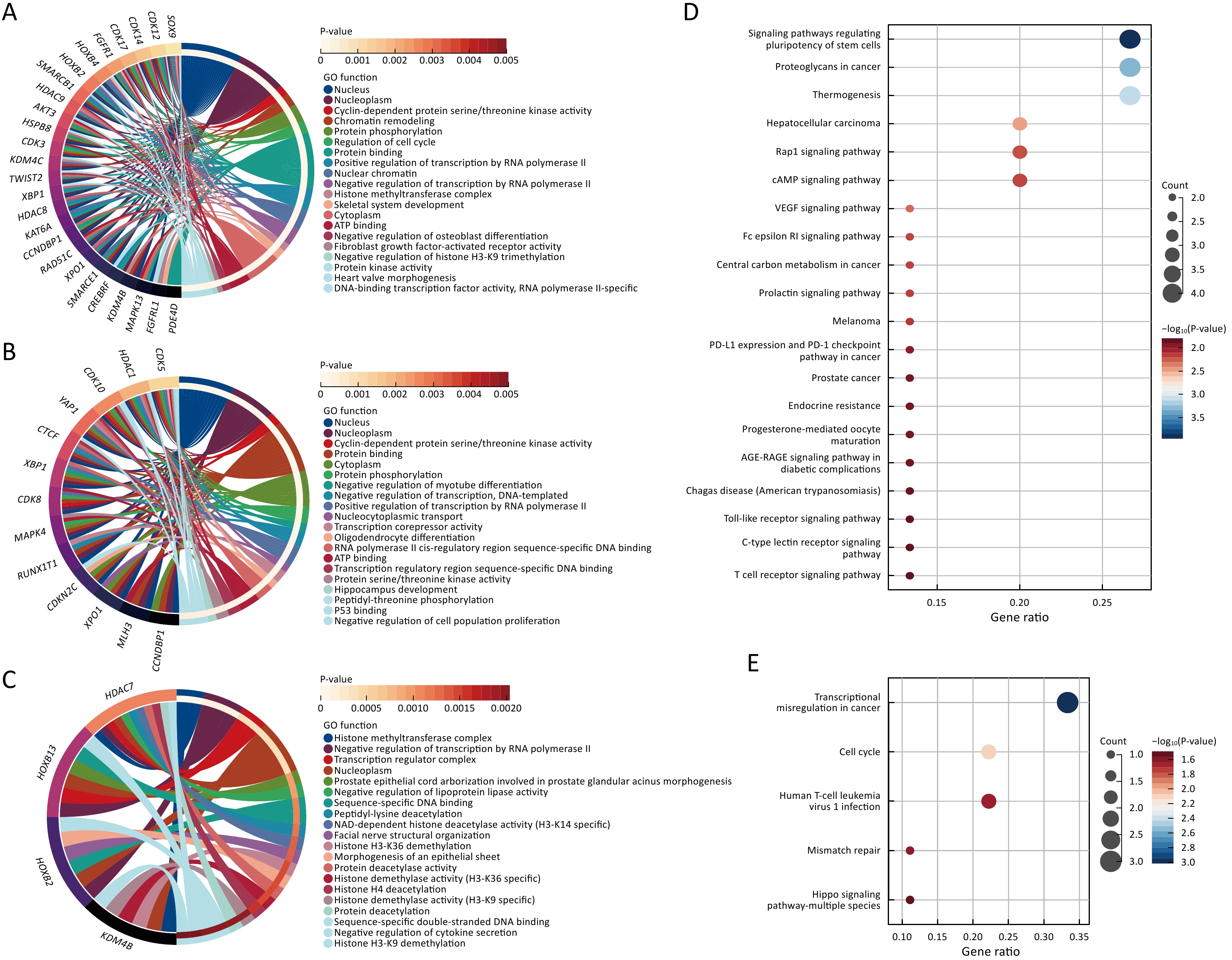
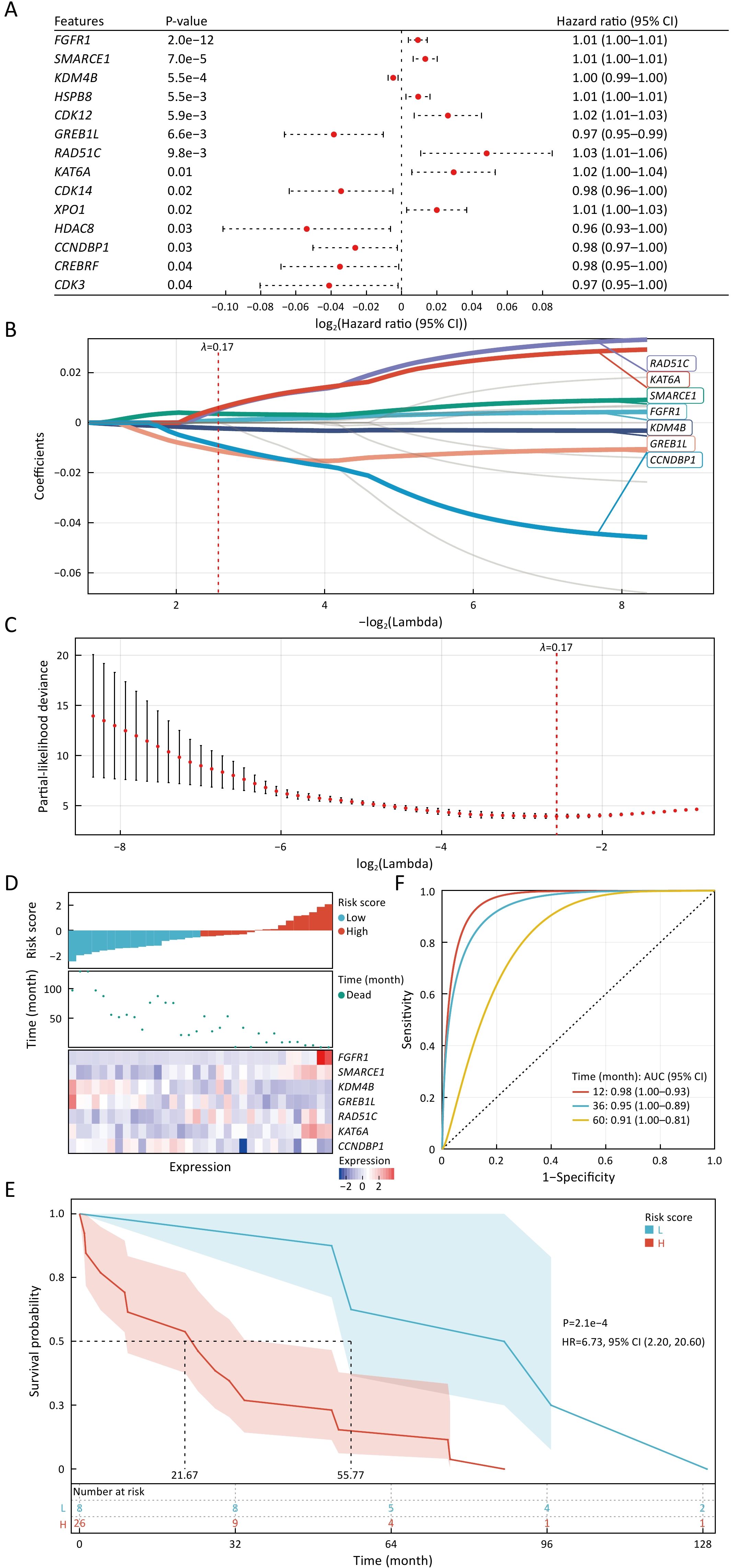
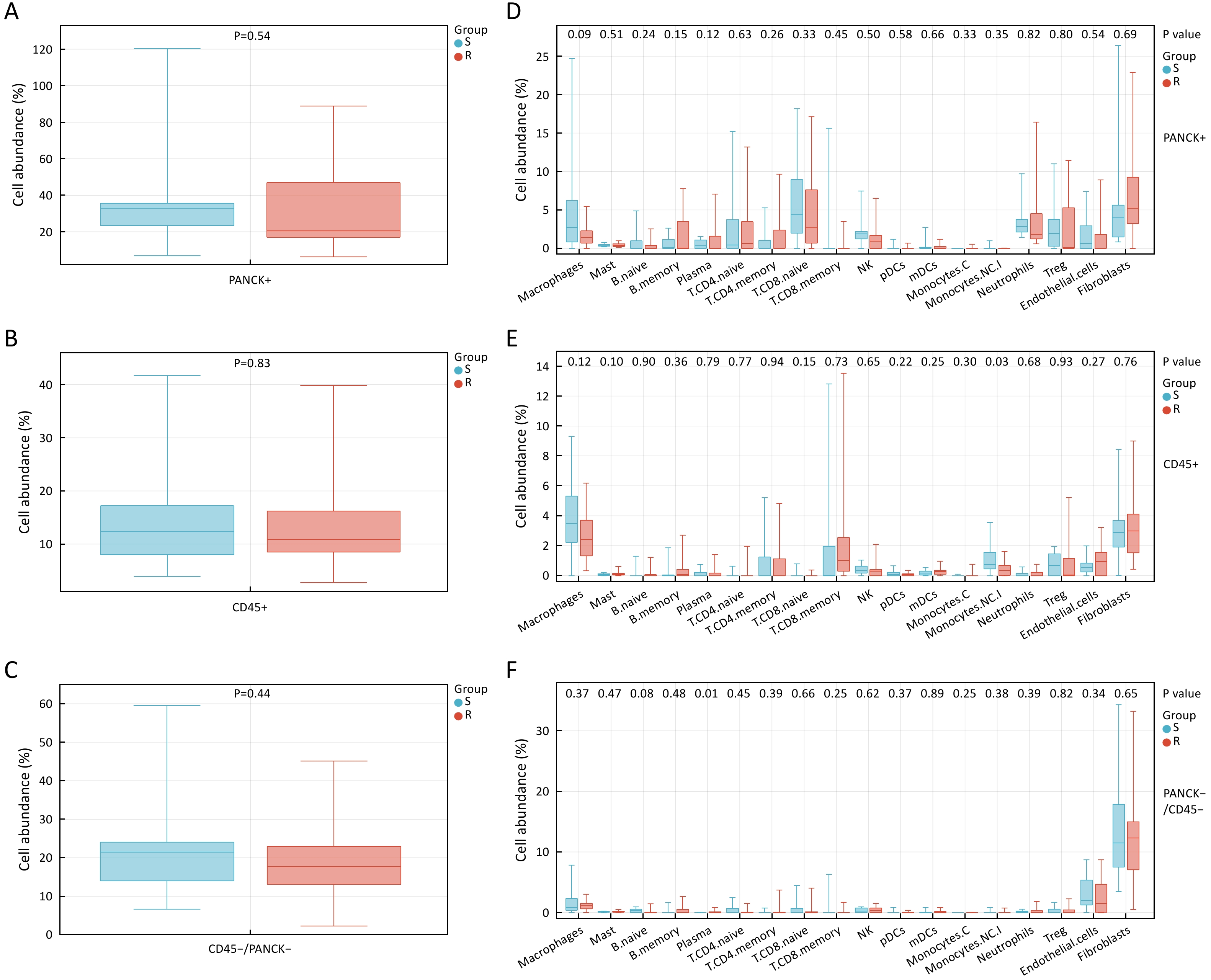
ObjectiveEndocrine resistance occurs in nearly all patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2−) early breast cancer (EBC), which can develop local and distant recurrence. The situation highlights the need to explore biomarkers for the efficacy of endocrine therapy (ET). MethodsWe performed digital spatial profiling on postoperative tumor samples from 20 HR+/HER2− EBC patients receiving adjuvant tamoxifen therapy, based on a designated panel comprising 235 ET-related genes. Paired patients were stratified into resistant and sensitive groups based on ET response. A total of 111 regions in three tissue compartments defined by morphology markers [tumor (PANCK+), leucocytes (CD45+), and nonimmune stroma (CD45−/PANCK−)] were investigated for immune and transcriptomic biomarkers. ResultsA total of 27, 13, and 5 differentially expressed genes (DEGs) were identified in PANCK+, CD45+, and CD45−/PANCK− regions. In the PANCK+ regions, mRNA expression of fourteen DEGs was significantly associated with disease-free survival (DFS), among which seven DEGs were further selected to construct a model for DFS. In the model, patients with low-risk scores had a median DFS of 55.77 months, significantly longer than 21.67 months among those with high-risk scores [P=2.1e−4, hazard ratio (HR)=6.73, 95% confidence interval (95% CI) =2.20−20.60)]. The area under curve for 1-year, 3-year, and 5-year DFS was 0.98, 0.95, and 0.91, indicating its superior efficacy. ET-sensitive patients had significantly higher non-classical monocyte infiltration in the CD45+ regions (P=0.03), whereas ET-resistant patients had significantly higher plasma cell infiltration in the CD45−/PANCK− regions (P=0.01). ConclusionsOur study has first demonstrated the spatial transcriptomic landscapes of patients with different responses to ET, which may help stratify patients who are responsive to ET and motivate the exploration of the molecular mechanisms of endocrine resistance.
2026, 38(3): 379-392.
doi: 10.21147/j.issn.1000-9604.2026.03.16
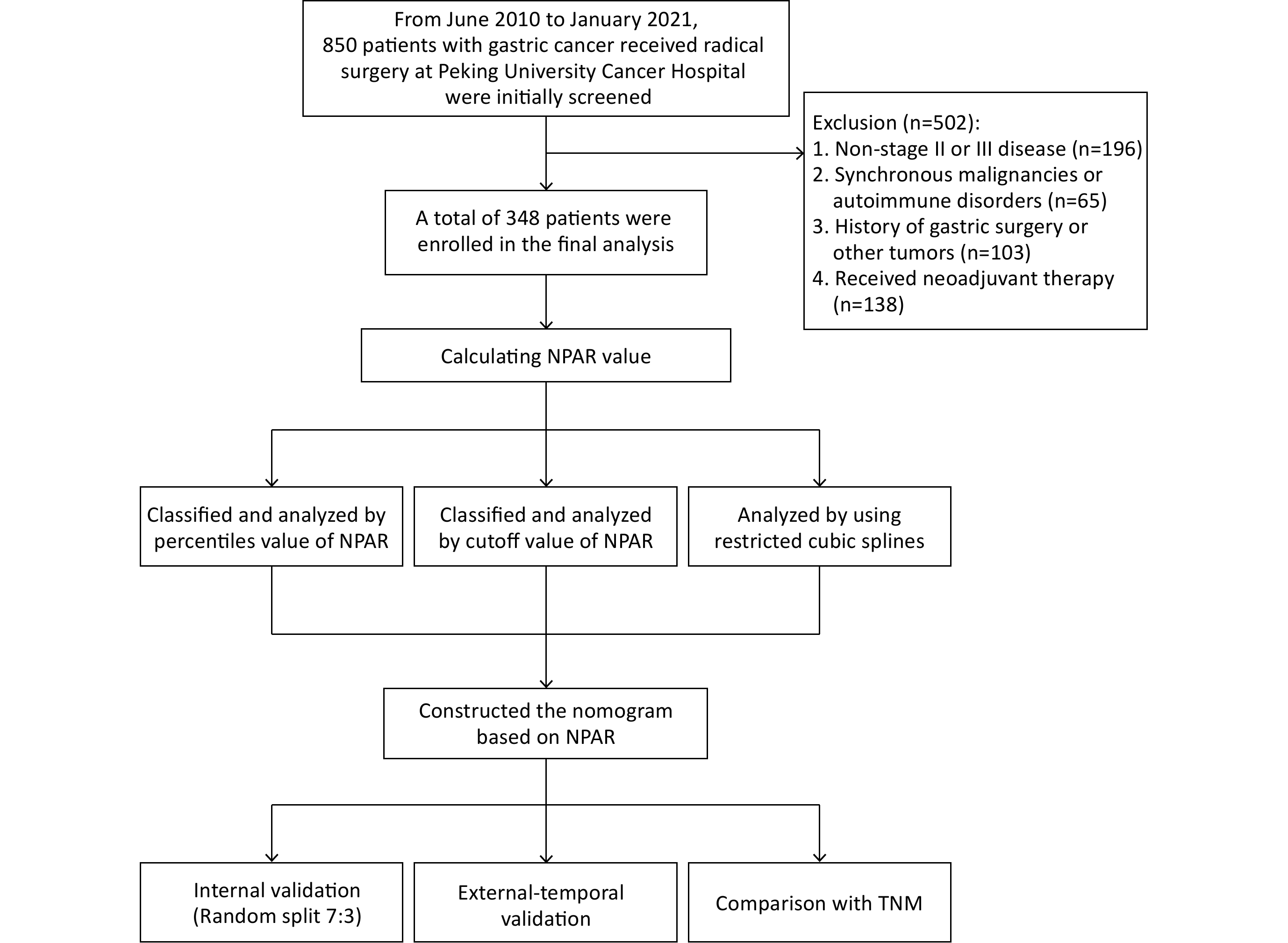
Abstract:
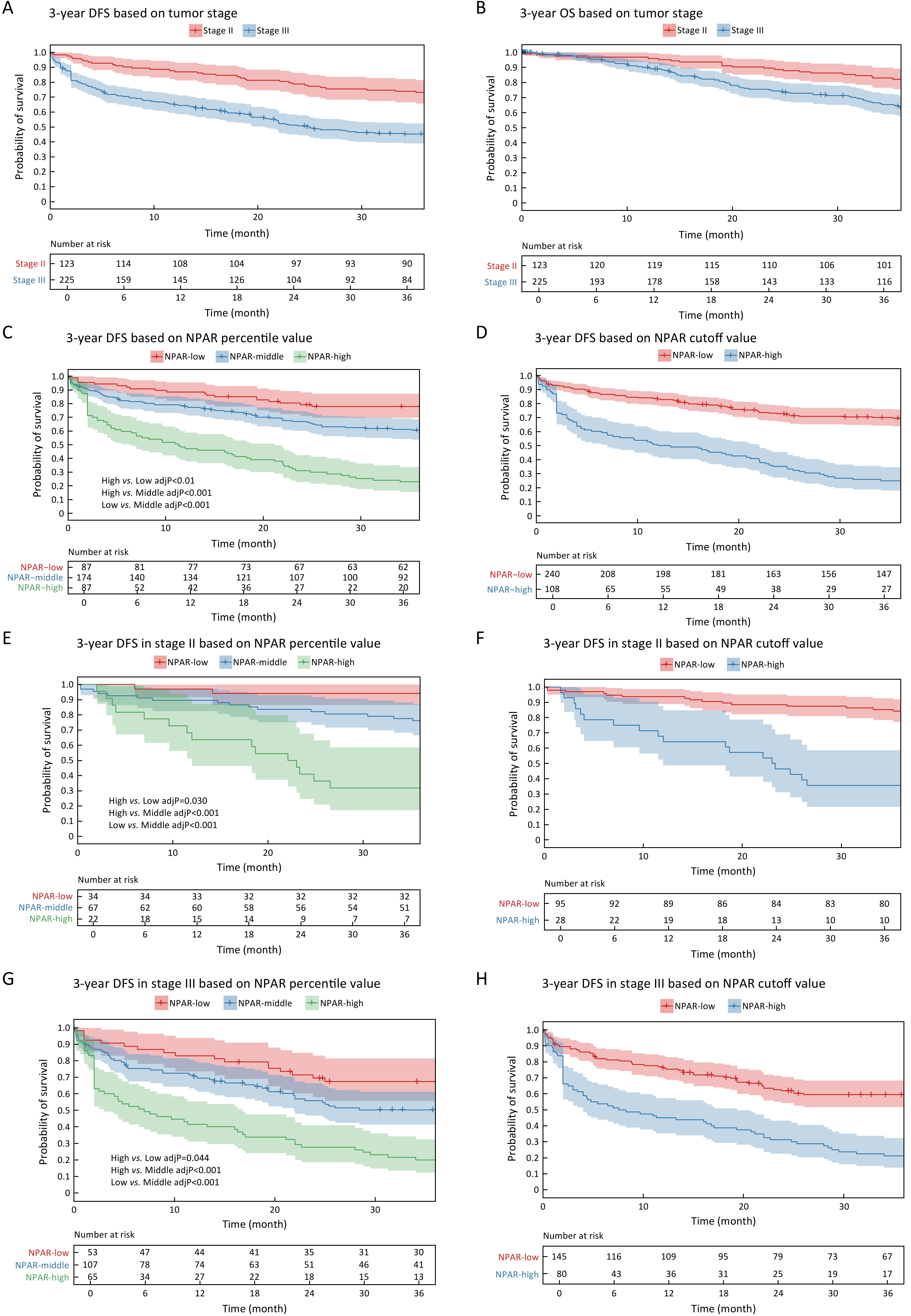
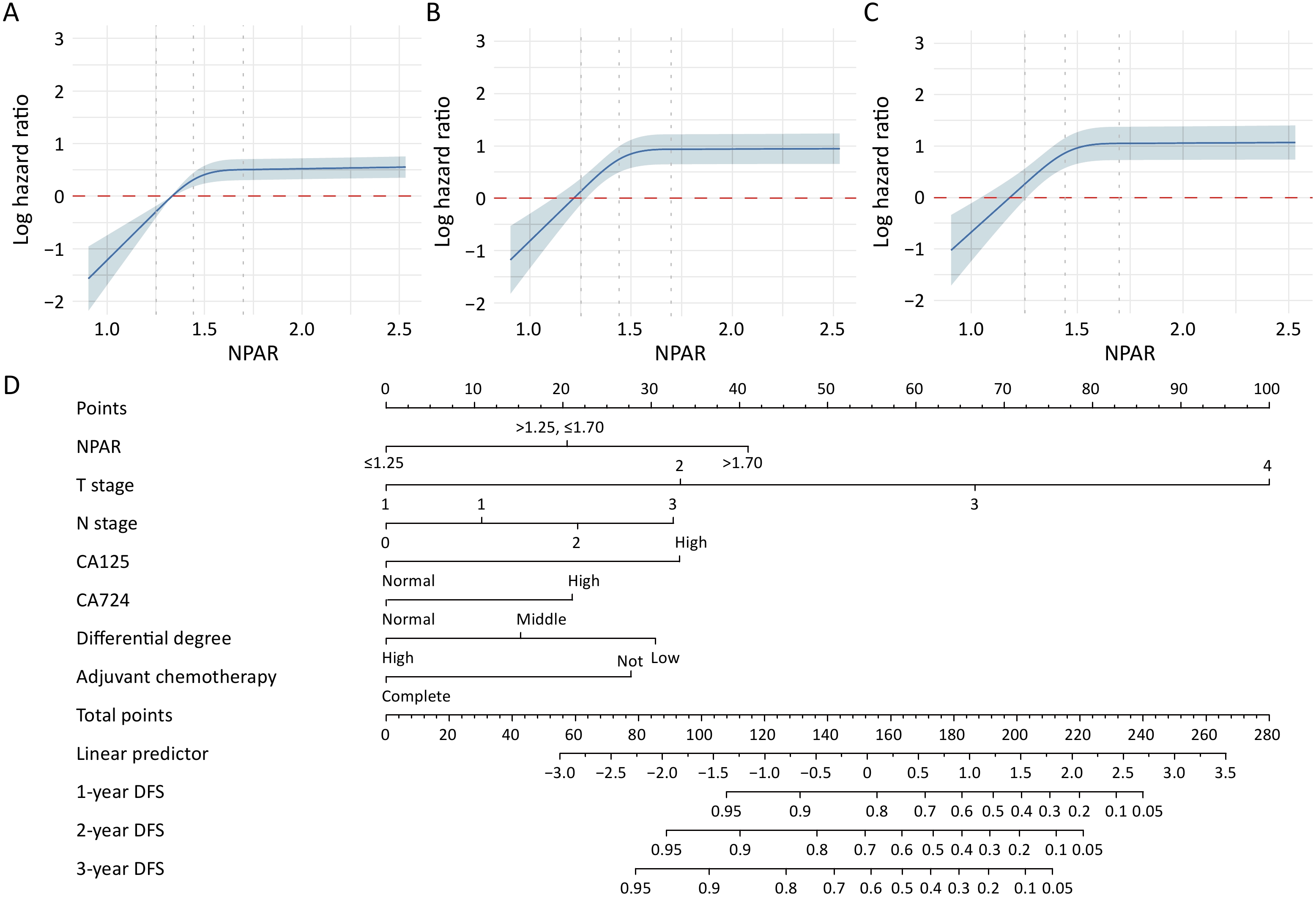
ObjectiveThis study aimed to clarify the predictive value of the neutrophil percentage to albumin ratio (NPAR) for postoperative survival in patients with locally advanced gastric cancer (LAGC) and to develop a prognostic model on the basis of these findings. MethodsPatients with LAGC who underwent radical surgery at Peking University Cancer Hospital between June 2010 and January 2021 were retrospectively screened. Three analytical approaches, percentile classification, cutoff value analysis, and restricted cubic splines (RCS), were utilized to evaluate the association between the NPAR and 3-year disease-free survival (DFS) rates. Survival curves were generated using the Kaplan-Meier method. Univariate and multivariate Cox regression analyses were used to identify the risk factors for 3-year DFS. A novel prognostic nomogram was then constructed and validated using both internal validation (via a 7:3 random split) and temporal external validation (stratified by the surgery dates before and after December 2017). ResultsA total of 348 patients were enrolled. All three analytical approaches consistently identified a high NPAR as a robust predictor of an unfavorable prognosis. Specifically, NPAR>1.70 (75th percentile) was associated with significantly lower DFS rates [hazard ratio (HR)=2.506; 95% confidence interval (95% CI): 1.964−3.198]. The optimal cutoff analysis confirmed that NPAR of 1.60 exhibited good discriminative ability (HR=3.639; 95% CI: 2.640−5.016), whereas the RCS analysis revealed a non-linear dose-response relationship between an elevated NPAR and low DFS rates. Multivariate Cox regression revealed the NPAR as an independent risk factor, along with pathological stage, differentiation type, and incomplete postoperative chemotherapy. The resulting prognostic nomogram demonstrated excellent and stable predictive performance across both internal and external temporal validation. ConclusionsThe NPAR was strongly associated with 3-year DFS rates in LAGC patients. Nomogram based on the NPAR exhibits high predictive accuracy and represents a practical tool for assessing DFS in clinical practice.