2015 Vol.27(4)
Display Mode: |
2015, 27(4): 318-320.
doi: 10.3978/j.issn.1000-9604.2015.06.10
 Abstract
Abstract FullText HTML
FullText HTML PDF 408KB
PDF 408KB
Abstract:

2015, 27(4): 332-348.
doi: 10.3978/j.issn.1000-9604.2015.06.07
Abstract:
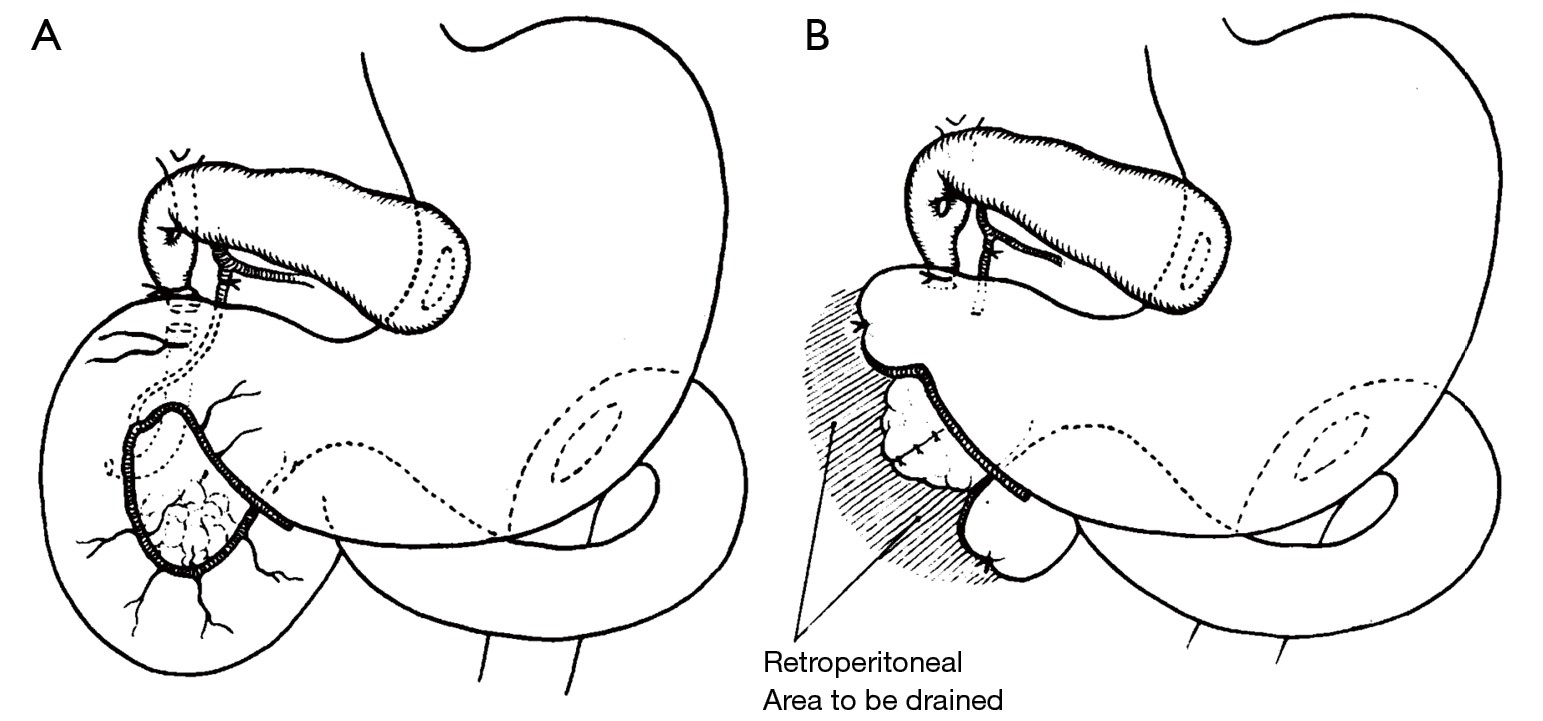
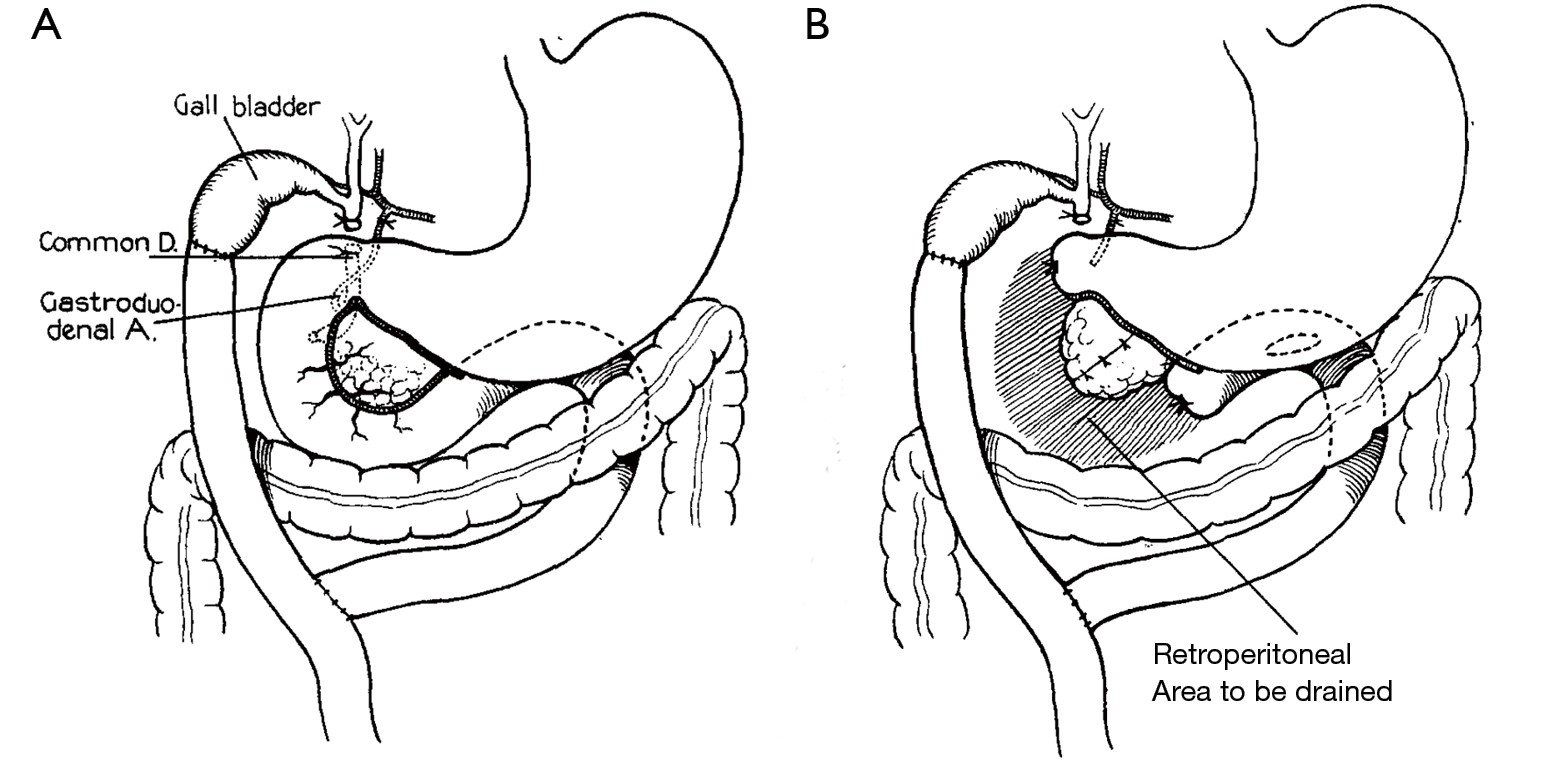
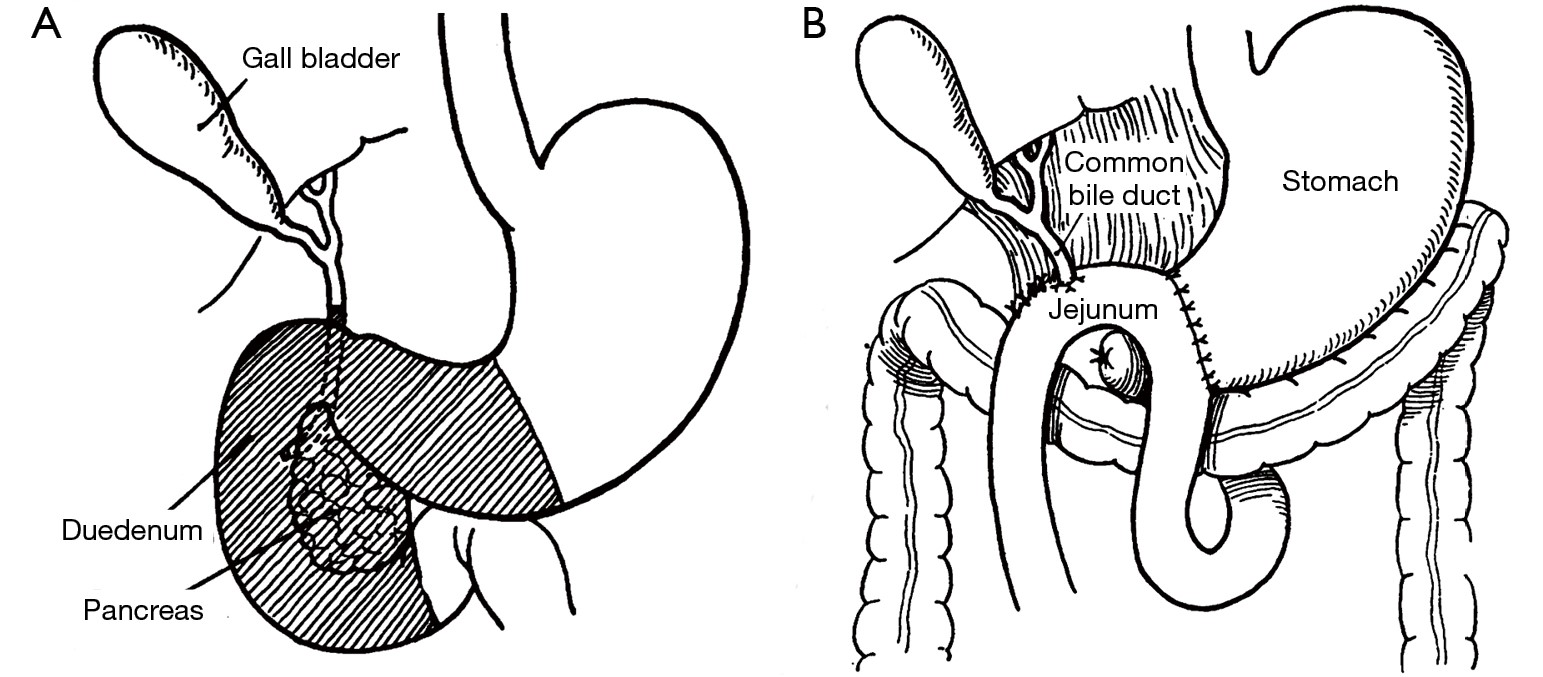
The history of pancreatic cancer surgery, though fraught with failure and setbacks, is punctuated by periods of incremental progress dependent upon the state of the art and the mettle of the surgeons daring enough to attempt it. Surgical anesthesia and the aseptic techniques developed during the latter half of the 19th century were instrumental in establishing a viable setting for pancreatic surgery to develop. Together, they allowed for bolder interventions and improved survival through the post-operative period. Surgical management began with palliative procedures to address biliary obstruction in advanced disease. By the turn of the century, surgical pioneers such as Alessandro Codivilla and Walther Kausch were demonstrating the technical feasibility of pancreatic head resections and applying principles learned from palliation to perform complicated anatomical reconstructions. Allen O. Whipple, the namesake of the pancreaticoduodenectomy (PD), was the first to take a systematic approach to refining the procedure. Perhaps his greatest contribution was sparking a renewed interest in the surgical management of periampullary cancers and engendering a community of surgeons who advanced the field through their collective efforts. Though the work of Whipple and his contemporaries legitimized PD as an accepted surgical option, it was the establishment of high-volume centers of excellence and a multidisciplinary approach in the later decades of the 20th century that made it a viable surgical option. Today, pancreatic surgeons are experimenting with minimally invasive surgical techniques, expanding indications for resection, and investigating new methods for screening and early detection. In the future, the effective management of pancreatic cancer will depend upon our ability to reliably detect the earliest cancers and precursor lesions to allow for truly curative resections.
The history of pancreatic cancer surgery, though fraught with failure and setbacks, is punctuated by periods of incremental progress dependent upon the state of the art and the mettle of the surgeons daring enough to attempt it. Surgical anesthesia and the aseptic techniques developed during the latter half of the 19th century were instrumental in establishing a viable setting for pancreatic surgery to develop. Together, they allowed for bolder interventions and improved survival through the post-operative period. Surgical management began with palliative procedures to address biliary obstruction in advanced disease. By the turn of the century, surgical pioneers such as Alessandro Codivilla and Walther Kausch were demonstrating the technical feasibility of pancreatic head resections and applying principles learned from palliation to perform complicated anatomical reconstructions. Allen O. Whipple, the namesake of the pancreaticoduodenectomy (PD), was the first to take a systematic approach to refining the procedure. Perhaps his greatest contribution was sparking a renewed interest in the surgical management of periampullary cancers and engendering a community of surgeons who advanced the field through their collective efforts. Though the work of Whipple and his contemporaries legitimized PD as an accepted surgical option, it was the establishment of high-volume centers of excellence and a multidisciplinary approach in the later decades of the 20th century that made it a viable surgical option. Today, pancreatic surgeons are experimenting with minimally invasive surgical techniques, expanding indications for resection, and investigating new methods for screening and early detection. In the future, the effective management of pancreatic cancer will depend upon our ability to reliably detect the earliest cancers and precursor lesions to allow for truly curative resections.





2015, 27(4): 358-367.
doi: 10.3978/j.issn.1000-9604.2015.05.02
Abstract:
The incidence of pancreatic adenocarcinoma (PDAC) has steadily increased over the past several decades. The majority of PDAC patients will present with distant metastases, limiting surgical management in this population. Hepatectomy and pulmonary metastasectomy (PM) has been well established for colorectal cancer patients with isolated, resectable hepatic or pulmonary metastatic disease. Recent advancements in effective systemic therapy for PDAC have led to the selection of certain patients where metastectomy may be potentially indicated. However, the indication for resection of oligometastases in PDAC is not well defined. This review will discuss the current literature on the surgical management of metastatic disease for PDAC with a specific focus on surgical resection for isolated hepatic and pulmonary metastases.
The incidence of pancreatic adenocarcinoma (PDAC) has steadily increased over the past several decades. The majority of PDAC patients will present with distant metastases, limiting surgical management in this population. Hepatectomy and pulmonary metastasectomy (PM) has been well established for colorectal cancer patients with isolated, resectable hepatic or pulmonary metastatic disease. Recent advancements in effective systemic therapy for PDAC have led to the selection of certain patients where metastectomy may be potentially indicated. However, the indication for resection of oligometastases in PDAC is not well defined. This review will discuss the current literature on the surgical management of metastatic disease for PDAC with a specific focus on surgical resection for isolated hepatic and pulmonary metastases.



2015, 27(4): 368-375.
doi: 10.3978/j.issn.1000-9604.2015.06.05
Abstract:
Laparoscopic pancreaticoduodenectomy (LPD) is an extremely challenging surgery. First described in 1994, it has been slow to gain in popularity. Recently, however, we have seen an increase in the number of centers performing this operation, including our own institution, as well as an increase in the quantity of published data. The purpose of this review is to describe the current status of LPD as described in the literature. We performed a literature search in the PubMed database using MeSH terms “laparoscopy” and “pancreaticoduodenectomy”. We then identified articles in the English language with over 20 patients that focused on LPD only. Review articles were excluded and only one article per institution was used for descriptive analysis in order to avoid overlap. There were a total of eight articles meeting review criteria, consisting of 492 patients. On descriptive analysis we found that percent of LPD due to high-grade malignancy averaged 47% over all articles. Average operative time was 452 minutes, blood loss 369 cc’s, pancreatic leak rate 15%, delayed gastric emptying 8.6%, length of hospital stay 9.4 days, and short term mortality 2.3%. Comparison studies between open pancreaticoduodenectomy (OPD) and LPD suggested decreased blood loss, longer operative time, similar post-operative complication rate, decreased pain, and shorter hospital length of stay for LPD. There was also increased number of lymph nodes harvested and similar margin free resections with LPD in the majority of studies. LPD is a safe surgery, providing many of the advantages typically associated with laparoscopic procedures. We expect this operation to continue to gain in popularity as well as be offered in increasingly more complex cases. In future studies, it will be beneficial to look further at the oncologic outcome data of LPD including survival.
Laparoscopic pancreaticoduodenectomy (LPD) is an extremely challenging surgery. First described in 1994, it has been slow to gain in popularity. Recently, however, we have seen an increase in the number of centers performing this operation, including our own institution, as well as an increase in the quantity of published data. The purpose of this review is to describe the current status of LPD as described in the literature. We performed a literature search in the PubMed database using MeSH terms “laparoscopy” and “pancreaticoduodenectomy”. We then identified articles in the English language with over 20 patients that focused on LPD only. Review articles were excluded and only one article per institution was used for descriptive analysis in order to avoid overlap. There were a total of eight articles meeting review criteria, consisting of 492 patients. On descriptive analysis we found that percent of LPD due to high-grade malignancy averaged 47% over all articles. Average operative time was 452 minutes, blood loss 369 cc’s, pancreatic leak rate 15%, delayed gastric emptying 8.6%, length of hospital stay 9.4 days, and short term mortality 2.3%. Comparison studies between open pancreaticoduodenectomy (OPD) and LPD suggested decreased blood loss, longer operative time, similar post-operative complication rate, decreased pain, and shorter hospital length of stay for LPD. There was also increased number of lymph nodes harvested and similar margin free resections with LPD in the majority of studies. LPD is a safe surgery, providing many of the advantages typically associated with laparoscopic procedures. We expect this operation to continue to gain in popularity as well as be offered in increasingly more complex cases. In future studies, it will be beneficial to look further at the oncologic outcome data of LPD including survival.



2015, 27(4): 376-391.
doi: 10.3978/j.issn.1000-9604.2015.05.01
Abstract:
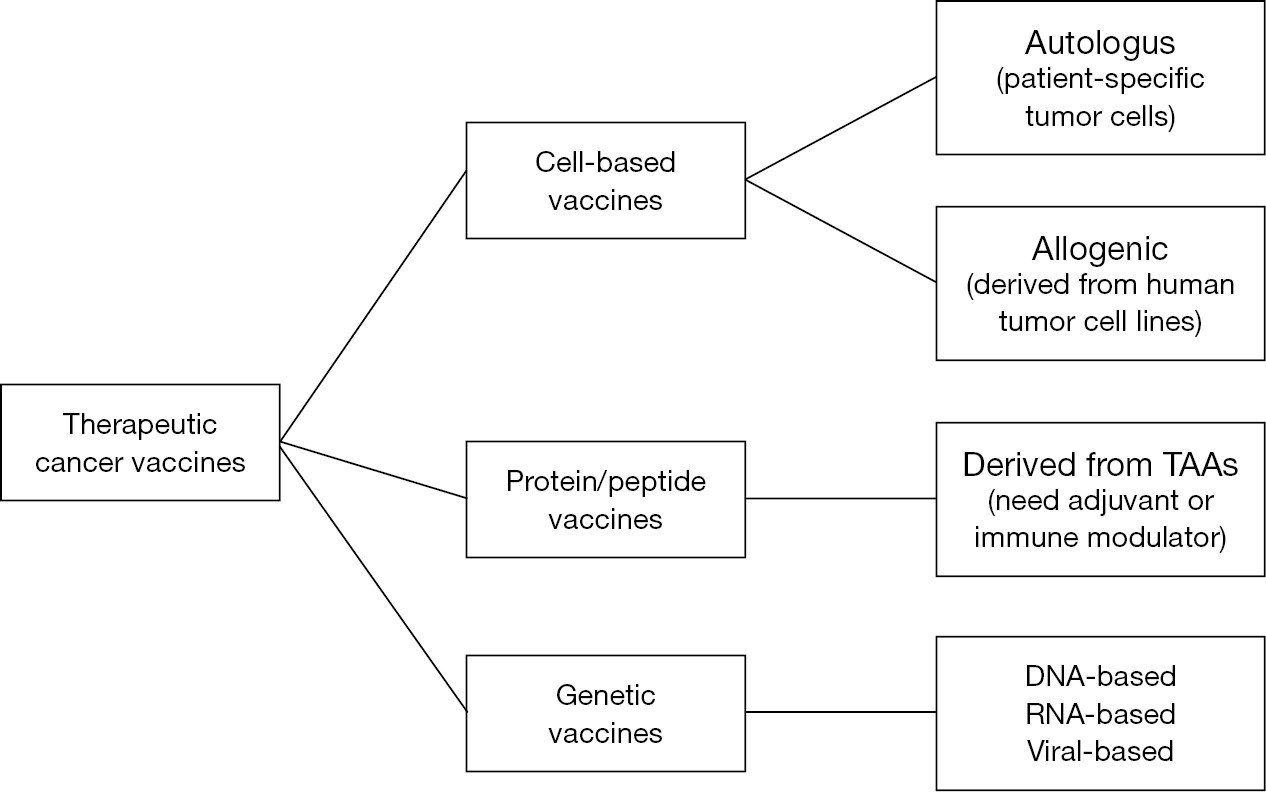
Pancreatic ductal adenocarcinoma (PDAC) is the fourth leading cause of cancer-related death and current therapeutic strategies are often unsatisfactory. Identification and development of more efficacious therapies is urgently needed. Immunotherapy offered encouraging results in preclinical models during the last decades, and several clinical trials have explored its therapeutic application in PDAC. The aim of this review is to summarize the results of clinical trials conducted to evaluate the future perspective of immunotherapy in the treatment of PDAC.
Pancreatic ductal adenocarcinoma (PDAC) is the fourth leading cause of cancer-related death and current therapeutic strategies are often unsatisfactory. Identification and development of more efficacious therapies is urgently needed. Immunotherapy offered encouraging results in preclinical models during the last decades, and several clinical trials have explored its therapeutic application in PDAC. The aim of this review is to summarize the results of clinical trials conducted to evaluate the future perspective of immunotherapy in the treatment of PDAC.


2015, 27(4): 392-396.
doi: 10.3978/j.issn.1000-9604.2015.04.13
Abstract:
As we have a deeper and more thorough understanding of the biological behavior of pancreatic head cancer, surgical treatment concepts of this lethal disease are changing all the time. Meanwhile, numerous arguments emerge. Thus, we will probe into the focuses and arguments in the surgical treatment of pancreatic head cancer in this article, including the scope of lymphadenectomy, total mesopancreas excision (TMpE), vascular resection, minimally invasive pancreaticoduodenectomy (PD), palliative resection, surgery for recurrent disease and surgery for primary pancreatic cancer and liver metastasis.
As we have a deeper and more thorough understanding of the biological behavior of pancreatic head cancer, surgical treatment concepts of this lethal disease are changing all the time. Meanwhile, numerous arguments emerge. Thus, we will probe into the focuses and arguments in the surgical treatment of pancreatic head cancer in this article, including the scope of lymphadenectomy, total mesopancreas excision (TMpE), vascular resection, minimally invasive pancreaticoduodenectomy (PD), palliative resection, surgery for recurrent disease and surgery for primary pancreatic cancer and liver metastasis.



2015, 27(4): 397-407.
doi: 10.3978/j.issn.1000-9604.2015.07.04
Abstract:
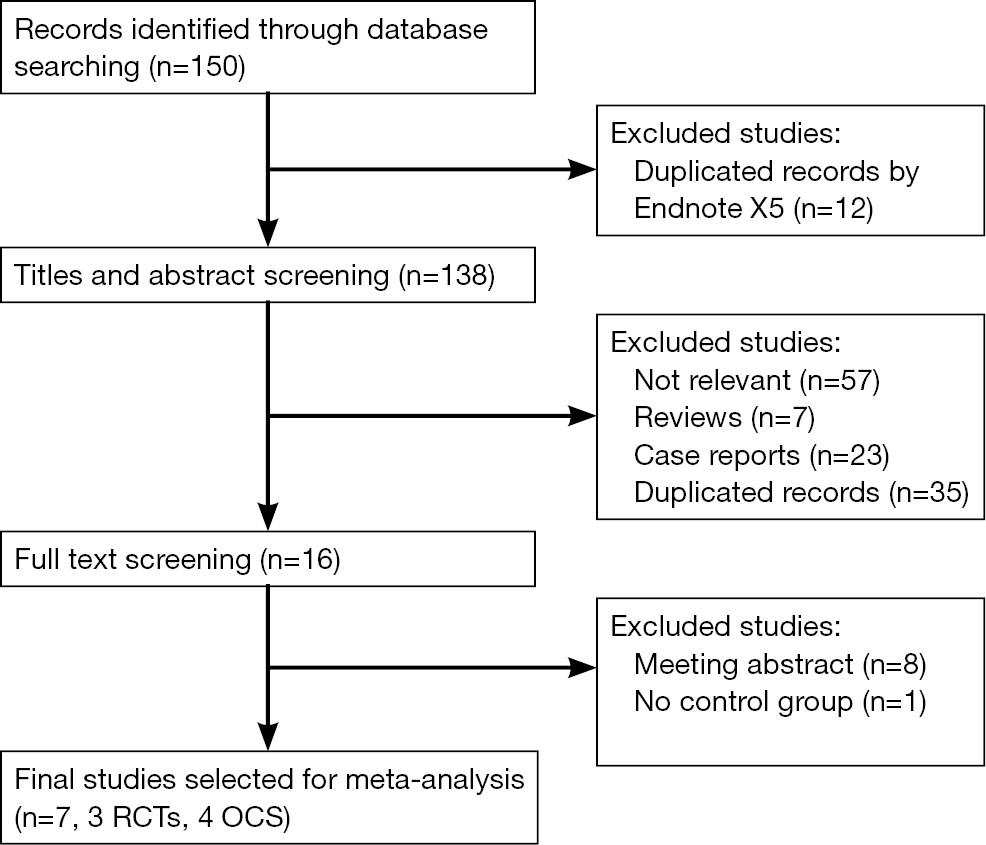
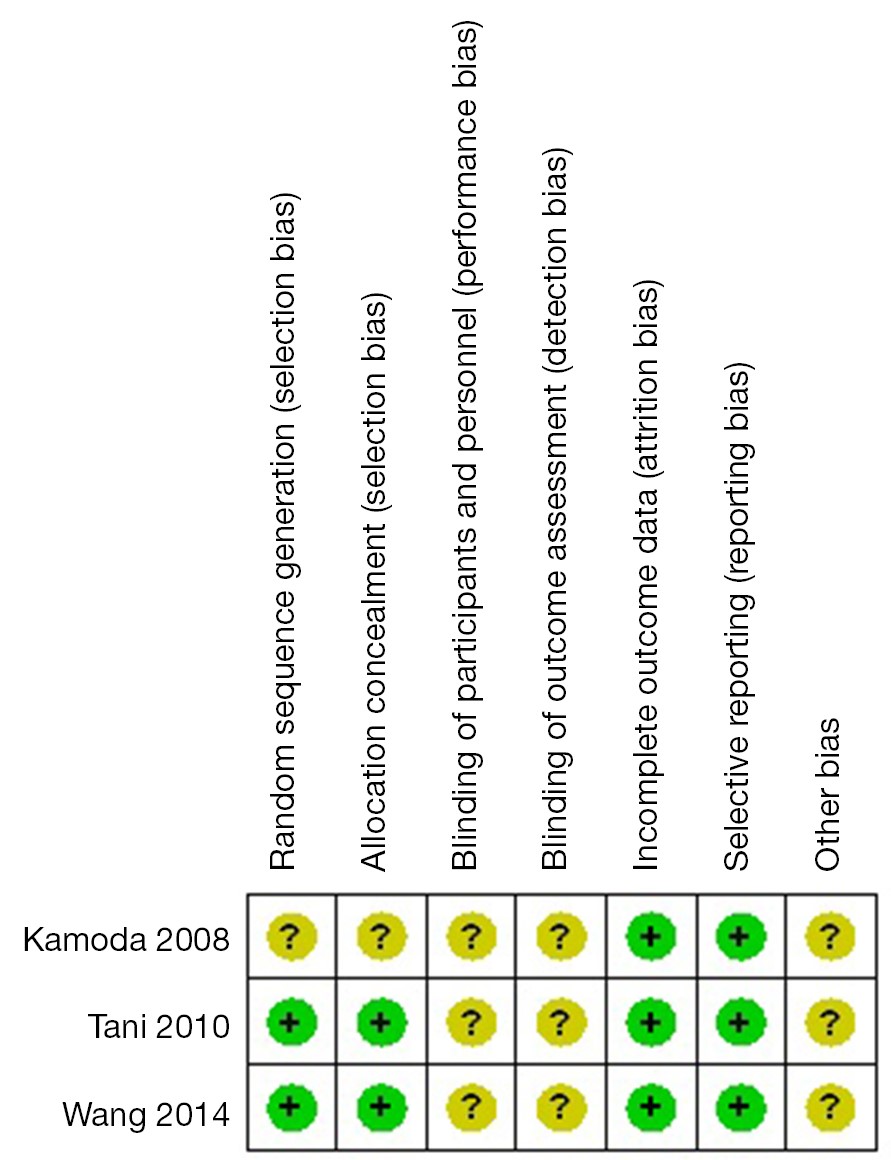
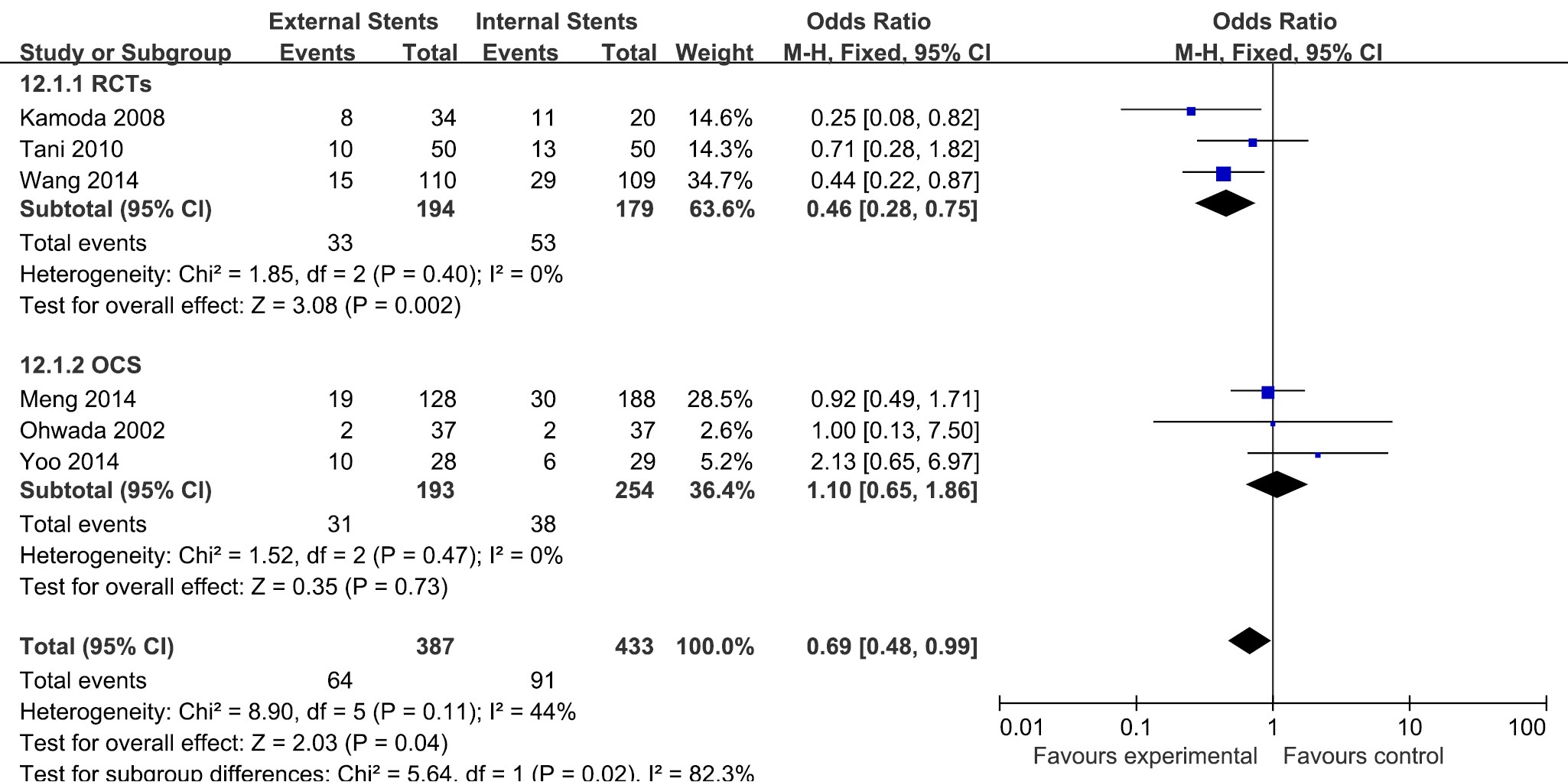
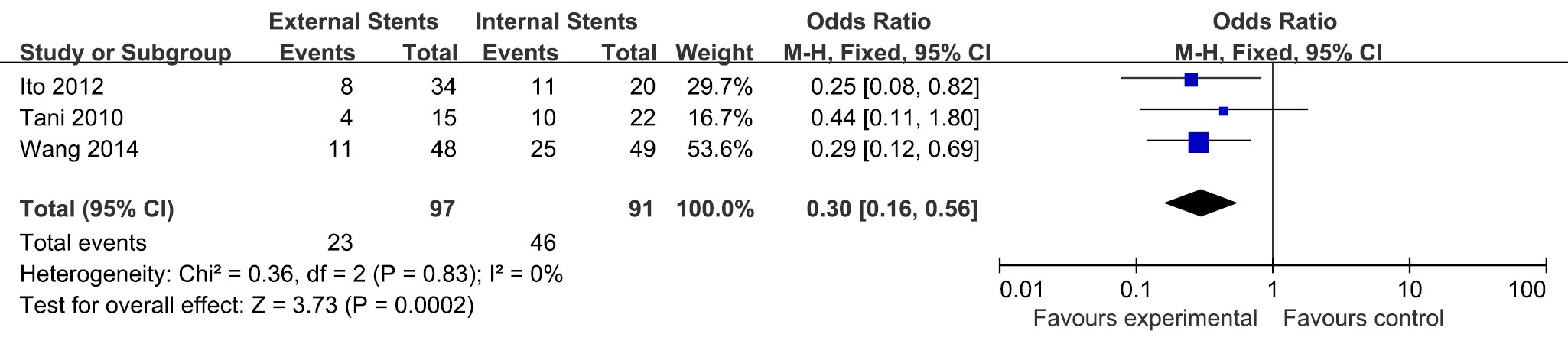
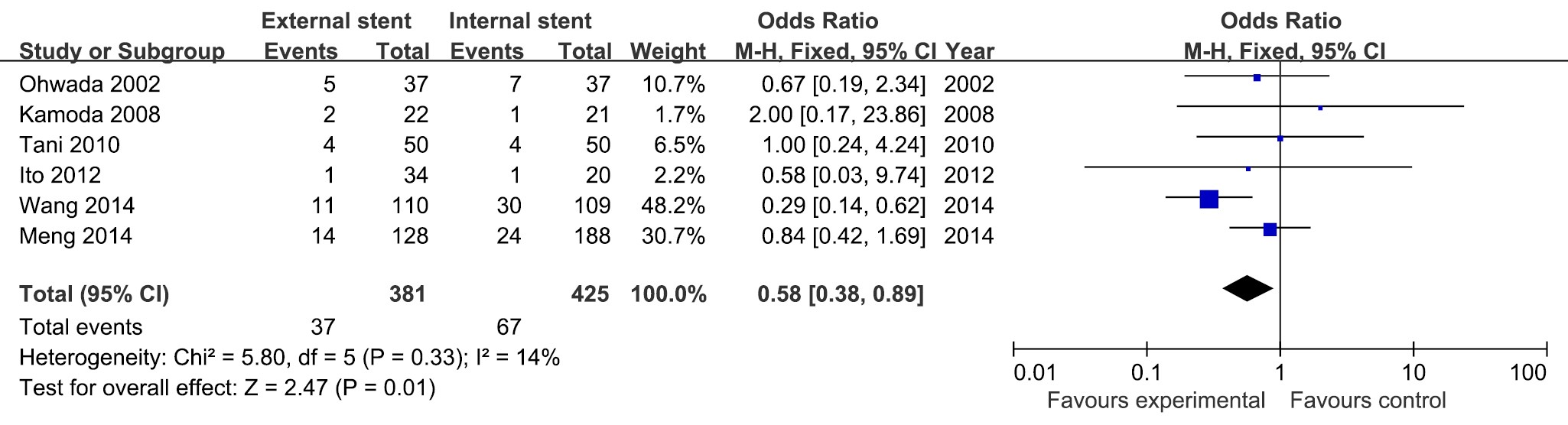
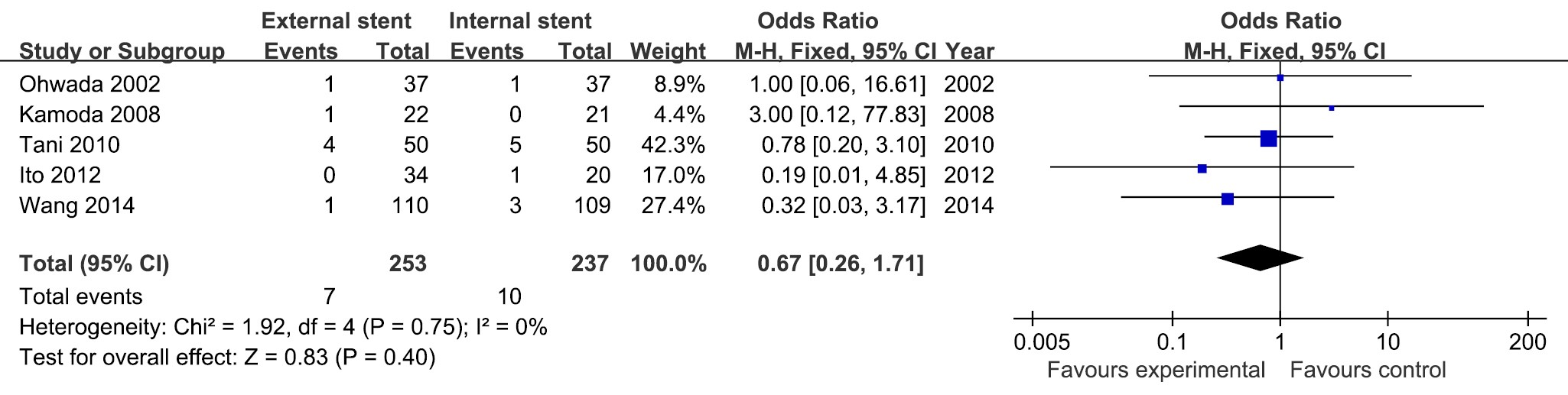
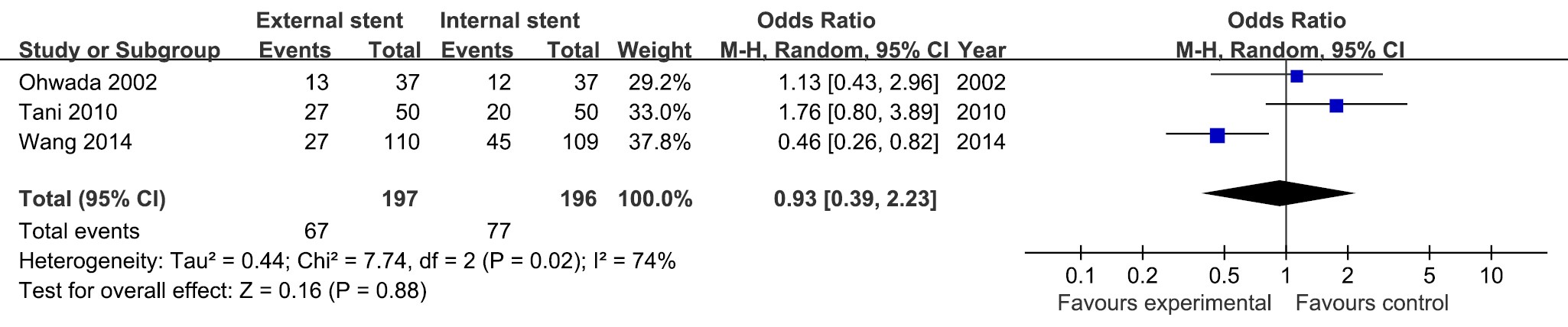
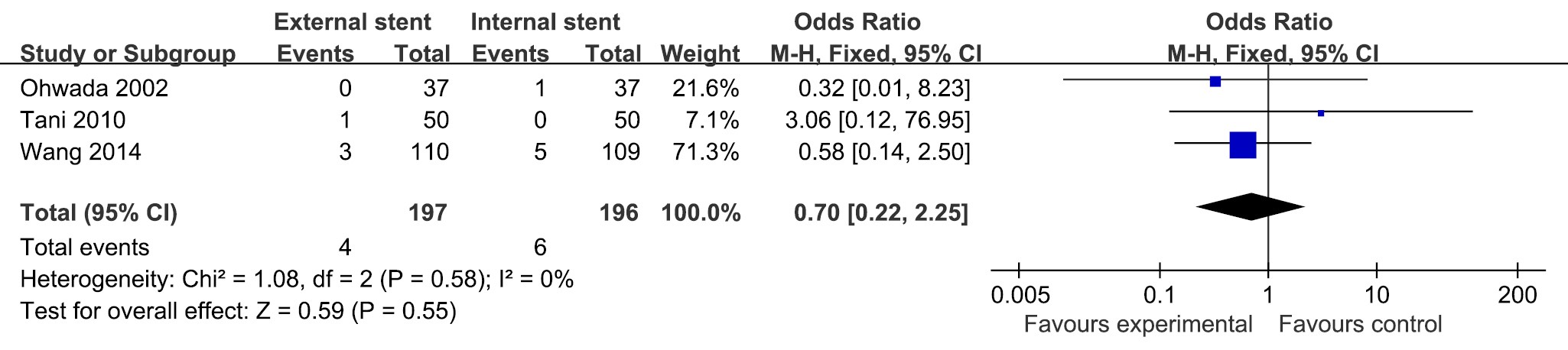
BackgroundTwo types of pancreatic duct stents are used to improve postoperative outcomes of pancreatic anastomosis. The aim of this meta-analysis was to evaluate and compare the postoperative outcomes of patients with internal or external stenting during pancreaticoduodenectomy (PD). MethodsWe searched PubMed, EMBASE, the Cochrane Library and Web of Science databases until the end of December, 2014. Studies comparing outcomes of external vs. internal stent placement in PD were eligible for inclusion. Included literature was extracted and assessed by two independent reviewers. ResultsSeven articles were identified for inclusion: three randomized controlled trials (RCTs) and four observational clinical studies (OCS). The meta-analyses revealed that use of external stents had advantage on reducing the incidences of pancreatic fistula (PF) in total [odds ratio (OR) =0.69; 95% confidence interval (CI), 0.48-0.99; P=0.04], PF in soft pancreas (OR =0.30; 95% CI, 0.16-0.56; P=0.0002) and delayed gastric emptying (DGE) (OR =0.58; 95% CI, 0.38-0.89; P=0.01) compared with internal stents. There were no significant differences in other postoperative outcomes between two stenting methods, including postoperative morbidity (OR =0.93; 95% CI, 0.39-2.23; P=0.88), overall mortality (OR =0.70; 95% CI, 0.22-2.25; P=0.55), and intra-abdominal collections (OR =0.67; 95% CI, 0.26-1.71; P=0.40). ConclusionsBased upon this meta-analysis, the use of external pancreatic stents might have potential benefit in reducing the incidence of PF and DGE. Due to the limited number of original studies, more RCTs are needed to further support our result and clarify the issue.



2015, 27(4): 417-422.
doi: 10.3978/j.issn.1000-9604.2015.06.09
Abstract:
2015, 27(4): 423-427.
doi: 10.3978/j.issn.1000-9604.2015.08.01
Abstract:
Cancer has become the first leading cause of death in the world, particularly in low- and middle-income countries. Facing the increasing trend of cancer incidence and mortality, China issued and implemented “three-early (early prevention, early diagnosis and early treatment)” national cancer prevention plan. As the main body and dependence of social governance, non-governmental organizations (NGOs) take over the role of government in the field of cancer prevention and treatment. American Cancer Society (ACS) made a research on cancer NGOs and civil society in cancer control and found that cancer NGOs in developing countries mobilize civil society to work together and advocate governments in their countries to develop policies to address the growing cancer burden. Union for International Cancer Control (UICC), Cancer Council Australia (CCA), and Malaysian cancer NGOs are the representatives of cancer NGOs in promoting cancer control. Selecting Chinese Anti-Cancer Association (CACA) as an example in China, this article is to investigate how NGOs undertake systematic cancer prevention work in China. By conducting real case study, we found that, as a NGO, CACA plays a significant role in intensifying the leading role of government in cancer control, optimizing cancer outcomes, decreasing cancer incidence and mortality rates and improving public health.
Cancer has become the first leading cause of death in the world, particularly in low- and middle-income countries. Facing the increasing trend of cancer incidence and mortality, China issued and implemented “three-early (early prevention, early diagnosis and early treatment)” national cancer prevention plan. As the main body and dependence of social governance, non-governmental organizations (NGOs) take over the role of government in the field of cancer prevention and treatment. American Cancer Society (ACS) made a research on cancer NGOs and civil society in cancer control and found that cancer NGOs in developing countries mobilize civil society to work together and advocate governments in their countries to develop policies to address the growing cancer burden. Union for International Cancer Control (UICC), Cancer Council Australia (CCA), and Malaysian cancer NGOs are the representatives of cancer NGOs in promoting cancer control. Selecting Chinese Anti-Cancer Association (CACA) as an example in China, this article is to investigate how NGOs undertake systematic cancer prevention work in China. By conducting real case study, we found that, as a NGO, CACA plays a significant role in intensifying the leading role of government in cancer control, optimizing cancer outcomes, decreasing cancer incidence and mortality rates and improving public health.
2015, 27(4): 428-436.
doi: 10.3978/j.issn.1000-9604.2015.08.02
Abstract:
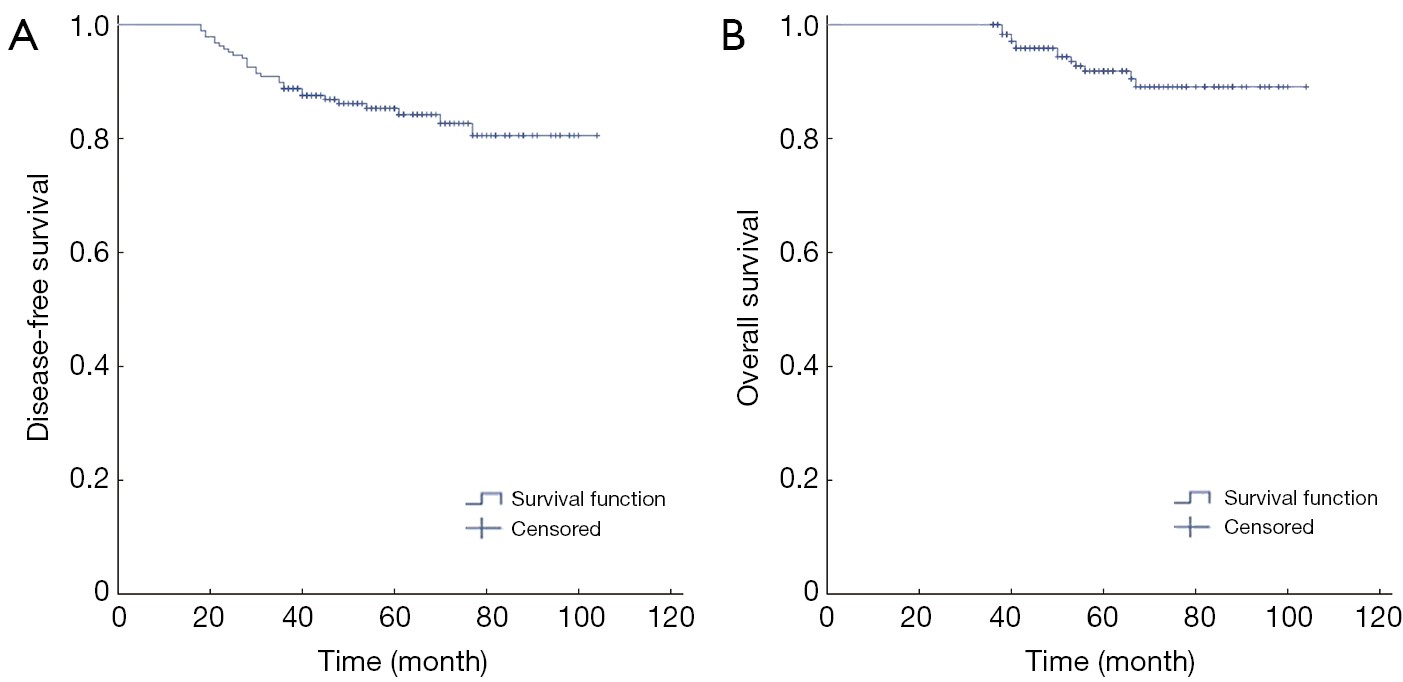
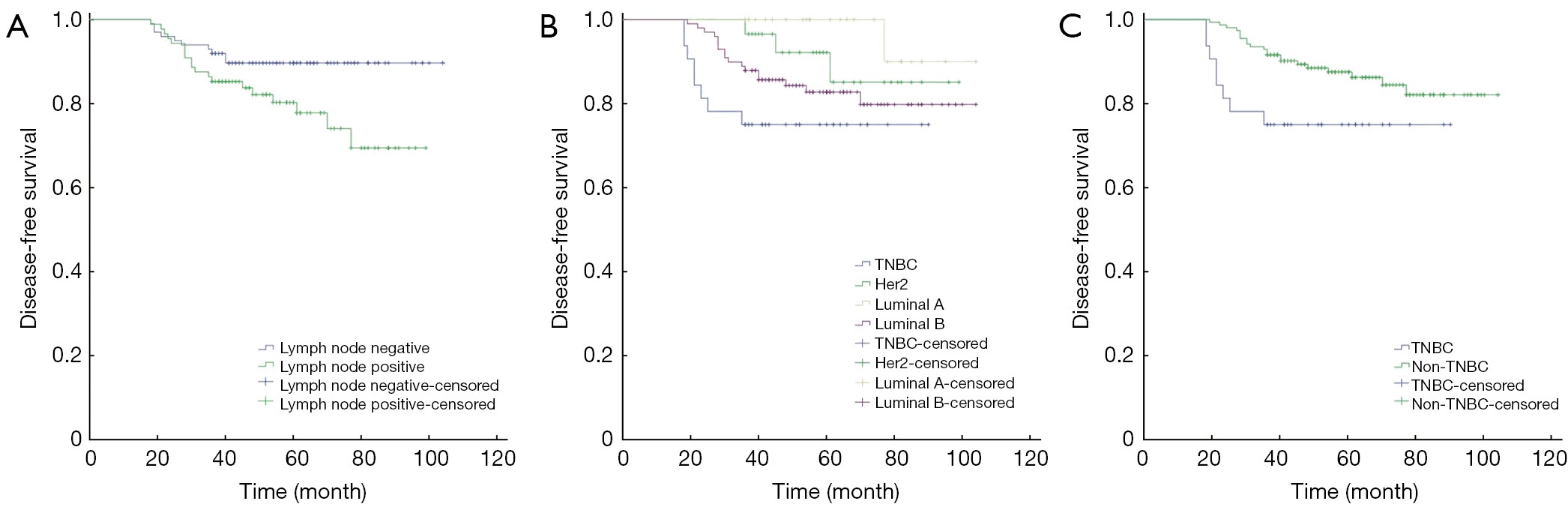
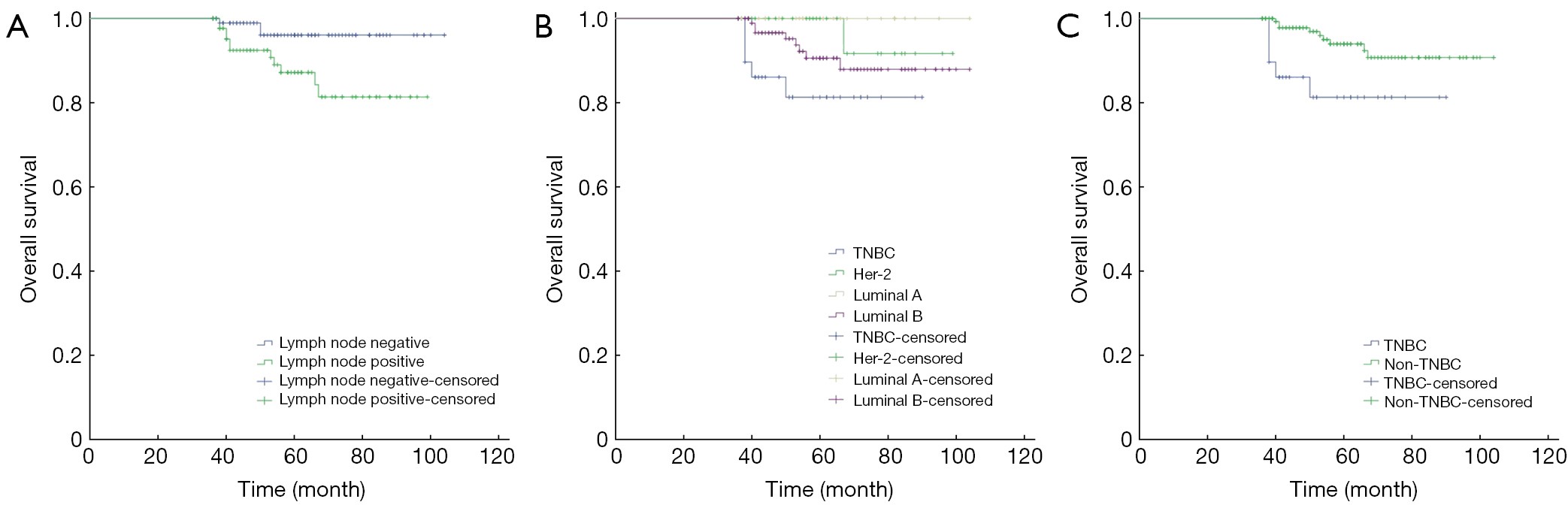
ObjectiveTo make a prognostic effect analysis of molecular subtype on young breast cancer patients. MethodsTotally 187 cases of young breast cancer patients less than 40 years old treated in Obstetrics and Gynecology Hospital of Fudan University between June 2005 and June 2011 were included in our study. We described their clinical-pathological characteristics, disease-free survival (DFS) rate, and overall survival (OS) rate after a median follow-up period of 61 months. The factors associated with prognosis were also evaluated by univariate and multivariate analyses. ResultsAll patients were premenopausal, with an average age of 35.36±3.88 years old. The mean tumor size was 2.43±1.53 cm. Eighty-one cases had lymph node metastasis (43.3%), 126 cases had lymphovascular invasion (67.4%), and 125 cases had histological grade III (66.8%) disease. Twenty-seven cases (14.4%) were Luminal A subtype, 99 cases (52.9%) were Luminal B subtype, 29 cases (15.5%) were human epidermal growth factor receptor 2 (HER-2) overexpression subtype, while 32 cases (17.1%) were triple negative breast cancer (TNBC) subtype according to 2013 St Gallen expert consensus. One hundred and thirty-five cases underwent mastectomy whereas 52 cases had breast-conserving surgery. One hundred and seventy-eight cases underwent adjuvant or neoadjuvant chemotherapy. Recurrence or metastasis occurred in 29 cases, 13 of which died. The 5-year DFS and OS rates were 84% and 92%. Multivariate analysis showed that nodal status (P=0.041) and molecular subtype (P=0.037) were both independent prognostic factors of DFS, while nodal status (P=0.037) and TNBC subtype (P=0.048) were both independent prognostic factors of OS. ConclusionsMolecular subtype is an independent prognostic factor of young breast cancer patients. TNBC has a high risk of relapse and death.