
2015 Vol.27(6)
Display Mode: |
2015, 27(6): 538-544.
doi: 10.3978/j.issn.1000-9604.2014.11.04
 Abstract
Abstract FullText HTML
FullText HTML PDF 180KB
PDF 180KB
Abstract:
BackgroundWe want to establish a lobe-specific mediastinal lymphadenectomy protocol for solitary pulmonary nodules (SPNs) in non-small cell lung cancer (NSCLC). MethodsWe retrospectively analyzed 401 patients with pathological diagnoses of NSCLC who underwent lobectomy, bilobectomy, or pneumonectomy with systematic lymphadenectomy from March 2004 to June 2011 in our hospital. All of the patients enrolled had a SPN preoperatively. Information about the primary tumor location, lymph node metastasis, and other baseline data were collected. Stepwise logistic regression was used to identify the key factors indicating non-regional mediastinal lymph node metastases (NRM). ResultsOf the primary tumors, 117, 39, 74, 104, and 67 were in the right upper lung (RUL), right middle lung (RML), right lower lung (RLL), left upper lung (LUL), and left lower lung (LLL), respectively. Stepwise regression showed that #2,4, #10,11, and #10,11 as well as #7 was the key lymph node station for RUL, LUL, and lower lobes: #2,4 [odds ratio (OR)=28.000, 95% confidence interval (CI): 2.917-268.790, P=0.004] for RUL, #10,11 (OR=31.667, 95% CI: 2.502-400.833, P=0.008) for LUL, #10,11 (OR=19.540, 95% CI: 4.217-90.541, P<0.001) and #7 (OR=7.395, 95% CI: 1.586-34.484, P=0.011) for lower lobes, respectively. Patients with tumors >2 cm rarely had NRM without primary regional mediastinal involvement. ConclusionsWith rigid consideration, a lobe-specific lymphadenectomy is feasible in practice. This protocol can be used when the lobe-specific key nodes are negative in intraoperative frozen sections, especially for NSCLC diagnosed as SPN <2 cm preoperatively.
2015, 27(6): 545-552.
doi: 10.3978/j.issn.1000-9604.2015.11.02
Abstract:
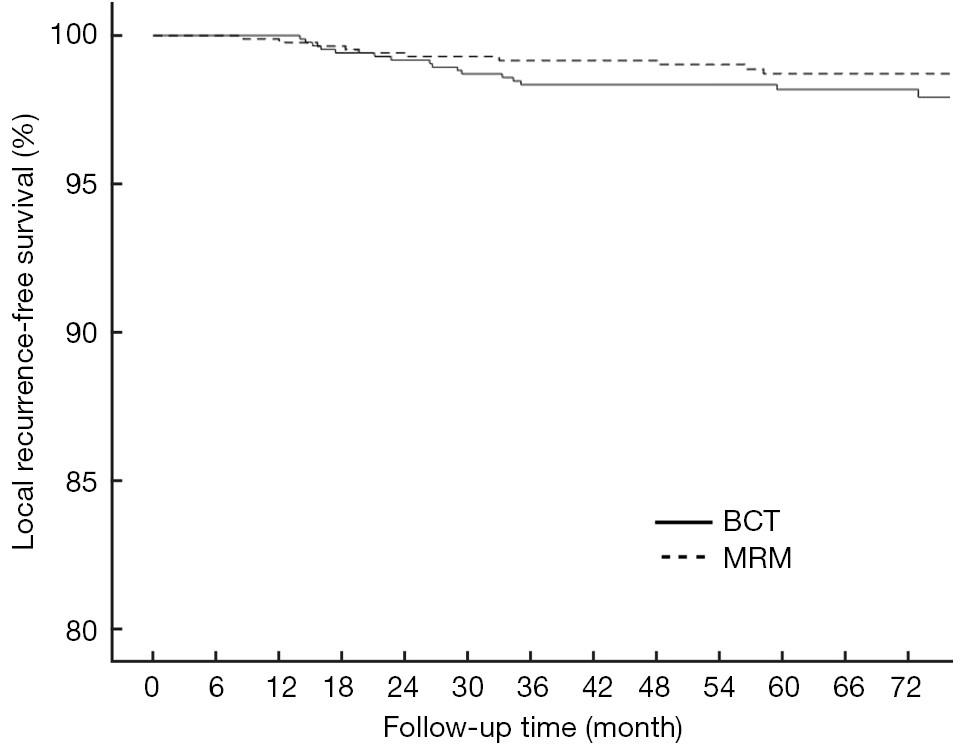
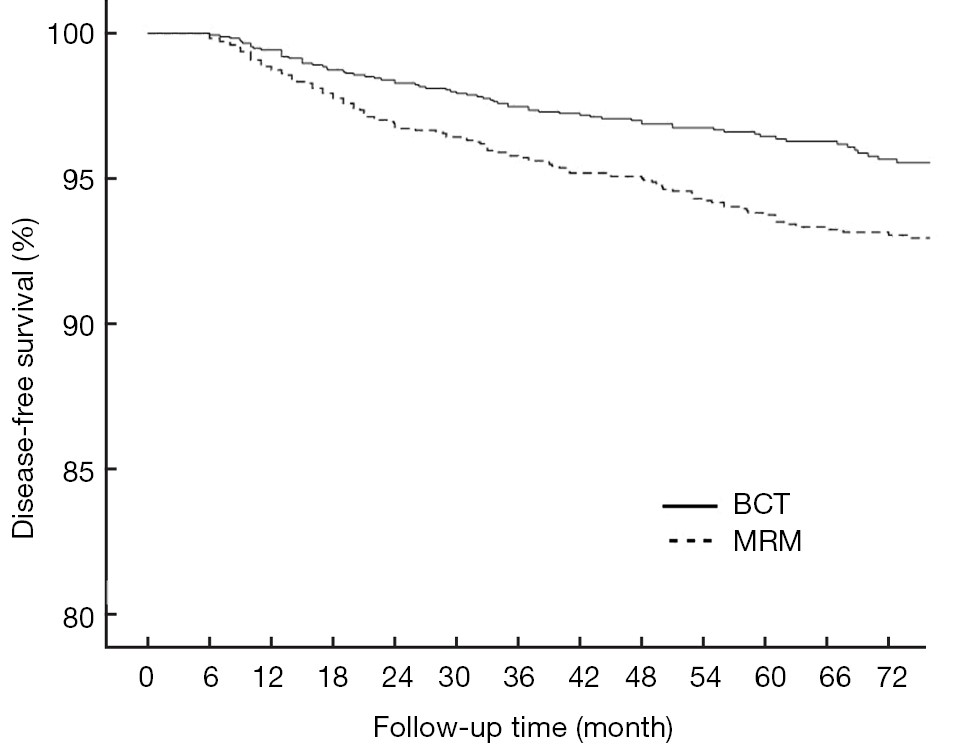
BackgroundTo compare two types of therapy for primary breast carcinoma, breast-conserving therapy (BCT) and modified radical mastectomy (MRM), in a matched cohort study. MethodsA series of 1,746 patients with primary breast cancer treated with BCT or MRM in a single Chinese institute between January 2000 and February 2009 were analyzed retrospectively to compare their outcomes with respect to the incidence of local recurrence (LR), distant metastasis, and survival. The patients were matched with regard to age at diagnosis, spreading to axillary lymph nodes, hormone receptor status, the use of neoadjuvant chemotherapy and maximal tumor diameter. The match ratio was 1:1, and each arm included 873 patients. ResultsThe median follow-up period was 71 months. The 6-year disease-free survival (DFS) and 6-year distant disease-free survival (DDFS) rates differed significantly between two groups. The 6-year local recurrence-free survival (LRFS) rates were 98.2% [95% confidence interval (CI): 0.973-0.989] in the BCT group and 98.7% (95% CI: 0.980-0.994) in the MRM group (P=0.182), respectively. DFS rates in BCT and MRM groups were 91.3% (95% CI: 0.894-0.932) and 86.3% (95% CI: 0.840-0.886) (P<0.001), respectively, whereas the DDFS rates in BCT and MRM groups were 93.6% (95% CI: 0.922-0.950) and 87.7% (95% CI: 0.854-0.900) (P<0.001), respectively. ConclusionsBCT in eligible patients is as effective as MRM with respect to local tumor control, DFS and DDFS, and may result in a better outcome than MRM in Chinese primary breast cancer patients.

2015, 27(6): 553-561.
doi: 10.3978/j.issn.1000-9604.2015.12.03
Abstract:
BackgroundWe recently showed HER2-positive breast cancers are less likely to respond to neoadjuvant anthracycline chemotherapy. Here, we investigated whether HER2-positive breast cancers responded to sequential neoadjuvant anthracycline followed by paclitaxel plus carboplatin regimen in the absence of trastuzumab. MethodsWomen (n=372) with operable primary breast cancer initially received two cycles of neoadjuvant anthracyclines, the clinical tumor response was assessed, then patients were received four cycles of paclitaxel plus carboplatin regimen. All the patients did not received trastuzumab treatment in the neoadjuvant setting. HER2 status was determined by immunohistochemistry and/or by fluorescence in situ hybridization in core-biopsy breast cancer tissue obtained before the neoadjuvant chemotherapy. ResultsEighteen percent (67/372) of patients achieved a pathologic complete response (pCR) in their breast. HER2-positive tumors had a significant higher pCR rate than HER2-negative tumors (33.0% versus 13.5%, P<0.001) in this cohort of 372 patients, and positive HER2 status remained an independent favorable predictor of pCR in a multivariate analysis [odds ratio (OR), 2.26; 95% confidence interval (CI), 1.18 to 4.36, P=0.015]. Furthermore, patients who responded to initial anthracycline regimens were more likely to respond to paclitaxel plus carboplatin than patients who did not (pCR, 27.2% versus 14.6%, P=0.005). Patients with HER2-positive tumors exhibited a significant higher pCR rate than did patients with HER2-negative tumors in both anthracycline response group (40.5% versus 20.0%, P=0.025) and anthracycline non-response group (28.3% versus 11.3%, P=0.002). ConclusionsUnder the circumstance of no trastuzumab treatment, women with HER2-positive cancers derive a large benefit from paclitaxel-carboplatin-based neoadjuvant chemotherapy.
2015, 27(6): 562-571.
doi: 10.3978/j.issn.1000-9604.2015.10.06
Abstract:
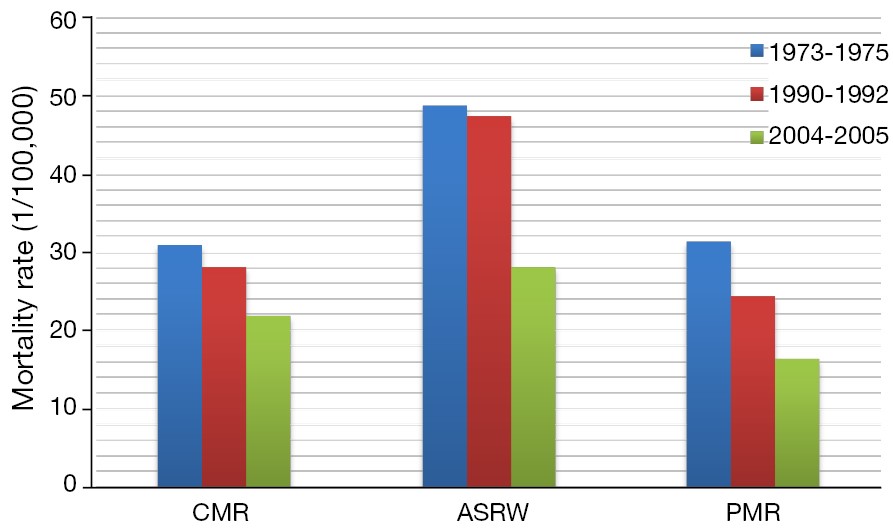
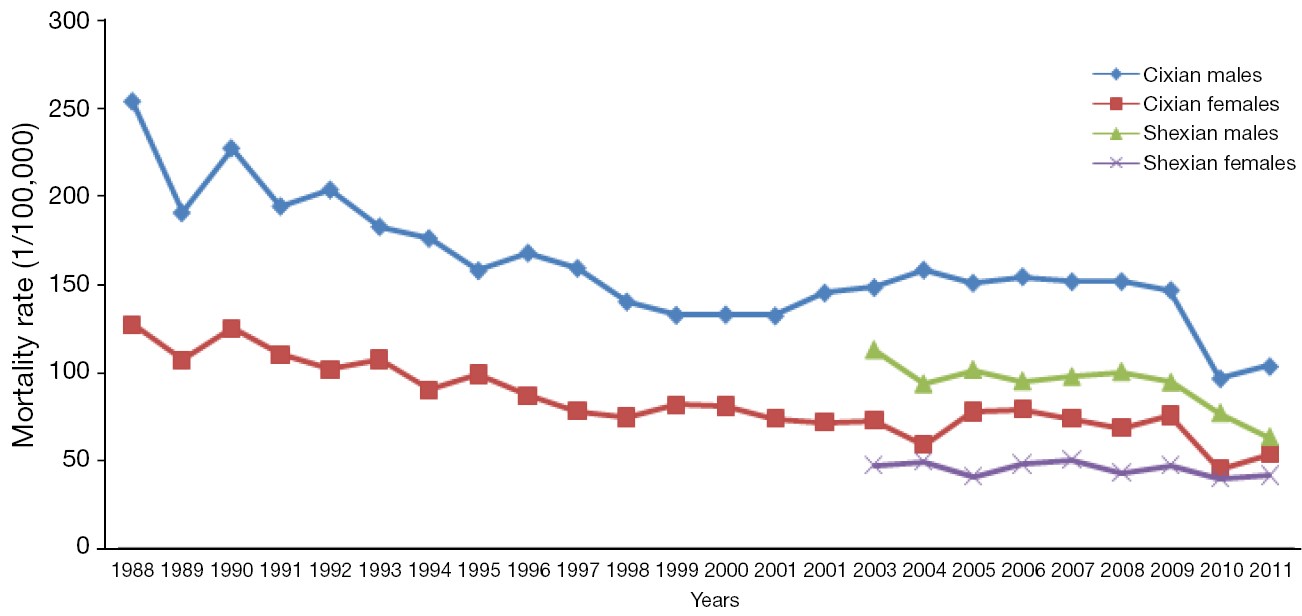
BackgroundHebei province is located in North of China with of approximately 6% of whole national population. It is known as a high-risk area for esophageal cancer in China and worldwide. The aim of our study was to estimate the esophageal cancer burden and trend in Hebei Province. MethodsEight cancer registries in Hebei Province submitted cancer registry data to the Hebei Provincial Cancer Registry Center. All data were qualified and compiled for cancer statistics in 2011. The pooled data were stratified by gender and age group (0, 1-4, 5-9, 10-14…80+). Incidence and mortality rates were age-standardized to World Segi’s population standard and expressed per 100,000 persons. In addition, proportions and cumulative incidence/mortality rates for esophageal cancer were calculated. Esophageal cancer mortality data during the periods 1973-1975, 1990-1992, and 2004-2005 were extracted from the national death surveys. Mortality and incidence rate data from Cixian and Shexian were obtained from population-based cancer registries in each county. ResultsThe estimated number of newly diagnosed esophageal cancer cases and deaths in 2011 in Hebei Province was 24,318 and 18,226, respectively. The crude incidence rate of esophageal cancer was 33.37/100,000 (males, 42.18/100,000 and females, 24.31/100,000). The age-standardized rate by world standard population (ASRW) was 28.09/100,000, ranking third among all cancers. The esophageal cancer mortality rate was 25.01/100,000 (males, 31.40/100,000 and females, 18.45/100,000), ranking third in deaths among all cancers. The mortality rates of esophageal cancer displayed a significant decreasing trend in Hebei Province from 1973-1975 (ASRW =48.69/100,000) to 2004-2005 (ASRW =28.02/100,000), with a decreased rate of 42.45%. In Cixian, the incidence of esophageal cancer decreased from 250.76/100,000 to 106.74/100,000 in males and from 153.86/100,000 to 75.41/100,000 in females, with annual percentage changes (APC) of 2.13 and 2.16, while the mortality rates declined with an APC of 2.46 for males and 3.10 for females from 1988 to 2011. In Shexian, the incidence rate decreased from 116.90/100,000 to 74.12/100,000 in males and from 46.98/100,000 to 40.64/100,000 in females, while the mortality rates declined, with an APC of 4.89 in males from 2003 to 2011. ConclusionsAlthough the incidence and mortality rates of esophageal cancer remain high, an obvious decreasing trend has been observed in Hebei Province, as well as in high-risk regions, such as Cixian and Shexian, over the past 40 years.


2015, 27(6): 572-579.
doi: 10.3978/j.issn.1000-9604.2015.12.06
Abstract:
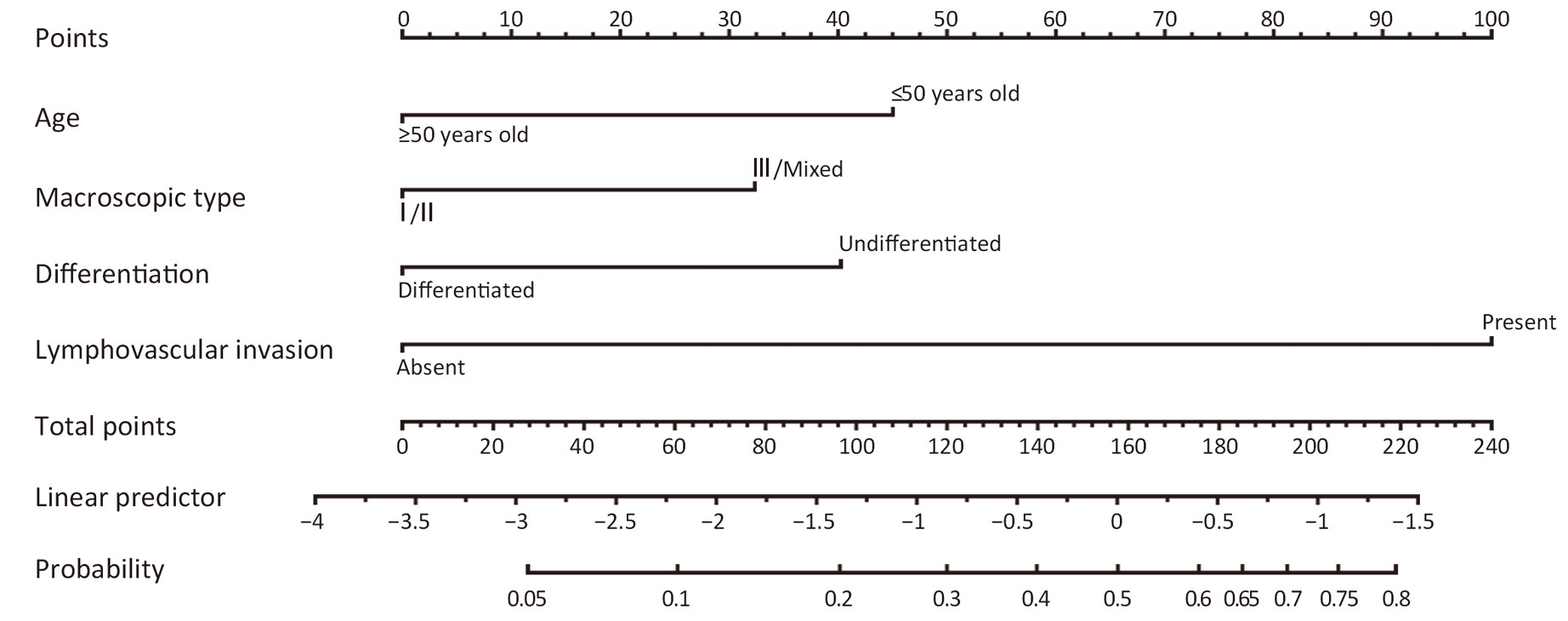
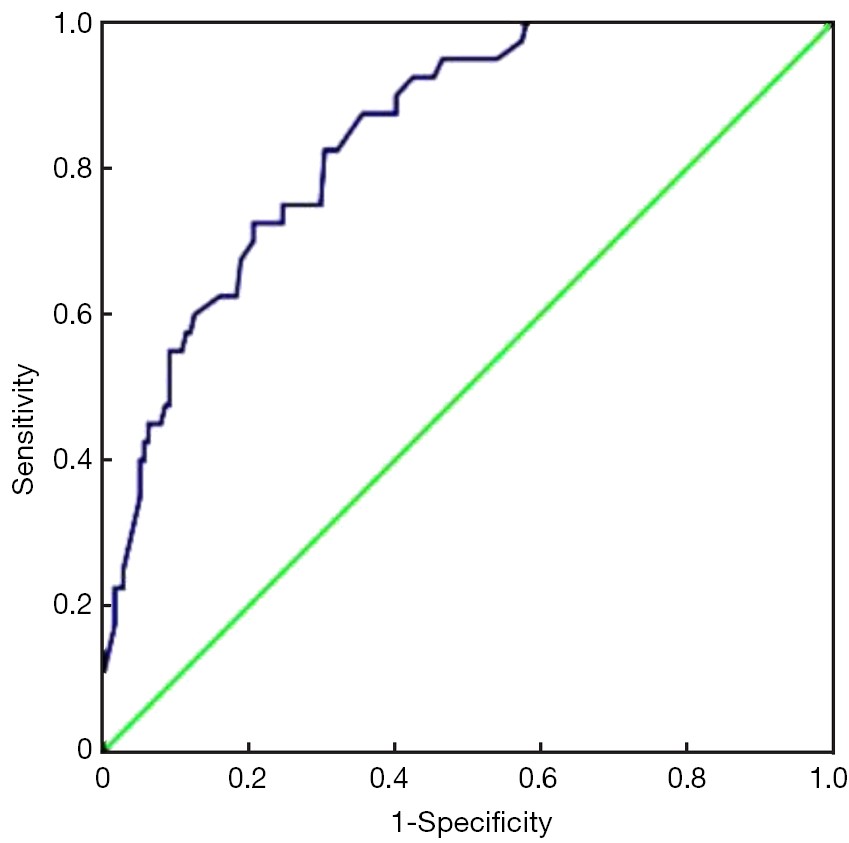
BackgroundTo combine clinicopathological characteristics associated with lymph node metastasis for submucosal gastric cancer into a nomogram. MethodsWe retrospectively analyzed 262 patients with submucosal gastric cancer who underwent D2 gastrectomy between 1996 and 2012. The relationship between lymph node metastasis and clinicopathological features was statistically analyzed. With multivariate logistic regression analysis, we made a nomogram to predict the possibility of lymph node metastasis. Receiver operating characteristic (ROC) analysis was also performed to assess the predictive value of the model. Discrimination and calibration were performed using internal validation. ResultsA total number of 48 (18.3%) patients with submucosal gastric cancer have pathologically lymph node metastasis. For submucosal gastric carcinoma, lymph node metastasis was associated with age, tumor location, macroscopic type, size, differentiation, histology, the existence of ulcer and lymphovascular invasion in univariate analysis (all P<0.05). The multivariate logistic regression analysis identified that age ≤50 years old, macroscopic type III or mixed, undifferentiated type, and presence of lymphovascular invasion were independent risk factors of lymph node metastasis in submucosal gastric cancer (all P<0.05). We constructed a predicting nomogram with all these factors for lymph node metastasis in submucosal gastric cancer with good discrimination [area under the curve (AUC) =0.844]. Internal validation demonstrated a good discrimination power that the actual probability corresponds closely with the predicted probability. ConclusionsWe developed a nomogram to predict the rate of lymph node metastasis for submucosal gastric cancer. With good discrimination and internal validation, the nomogram improved individualized predictions for assisting clinicians to make appropriated treatment decision for submucosal gastric cancer patients.

2015, 27(6): 580-587.
doi: 10.3978/j.issn.1000-9604.2015.12.02
Abstract:
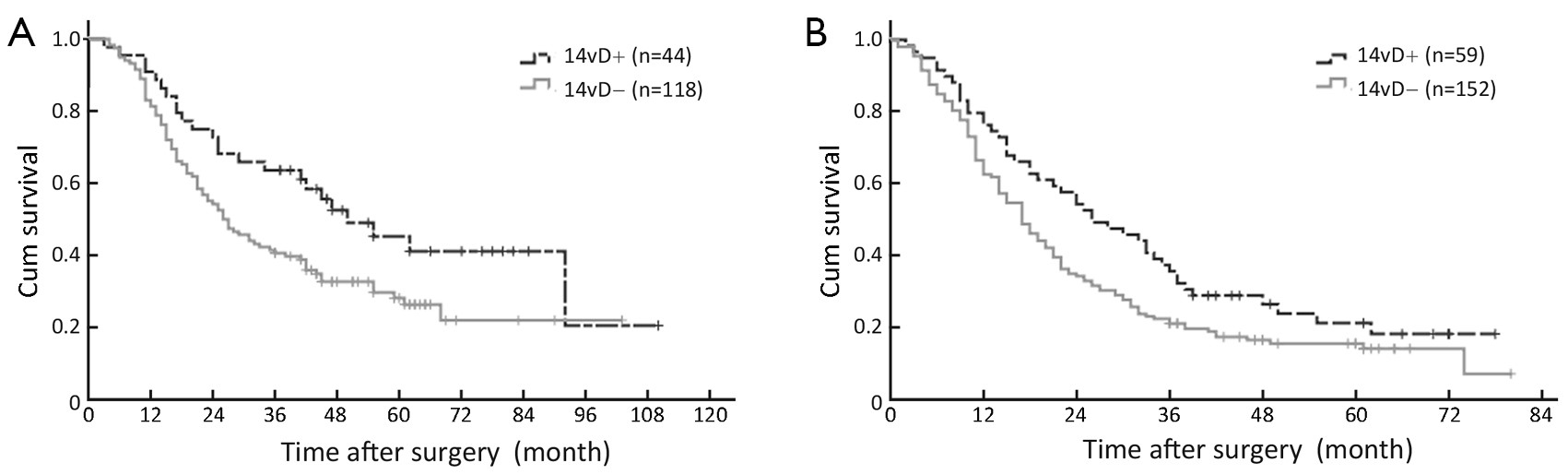
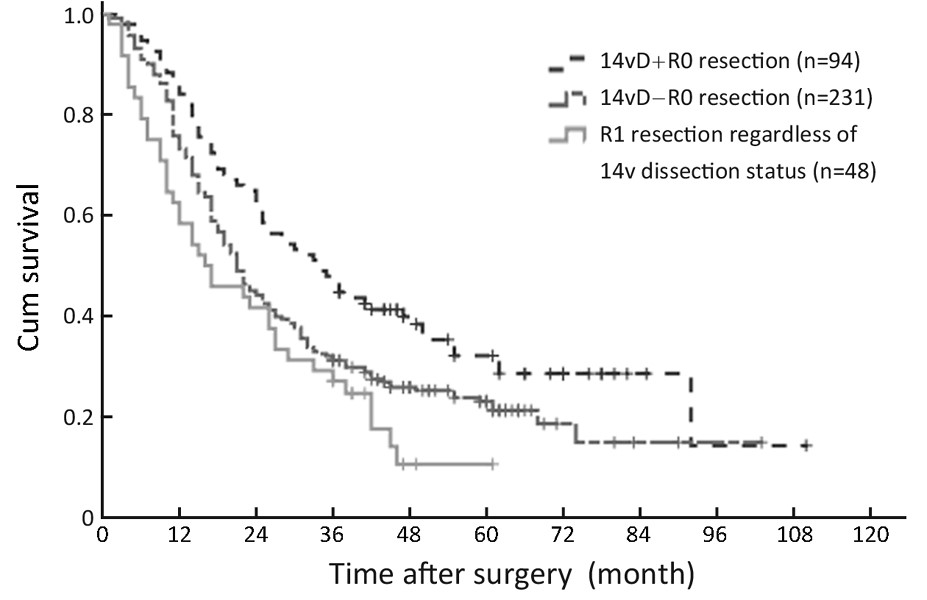
BackgroundD2 lymphadenectomy has been increasingly regarded as standard surgical procedure for advanced gastric cancer (GC), while the necessity of No.14v lymph node (14v) dissection for distal GC is still controversial. MethodsA total of 920 distal GC patients receiving at least a D2 lymph node dissection in Department of Gastric Cancer, Tianjin Medical University Cancer Institute and Hospital were enrolled in this study, of whom, 243 patients also had the 14v dissected. Other 677 patients without 14v dissection were used for comparison. ResultsForty-five (18.5%) patients had 14v metastasis. There was no significant difference in 3-year overall survival (OS) rate between patients with and without 14v dissection. Following stratified analysis, in TNM stages I, II, IIIa and IV, 14v dissection did not affect 3-year OS; in contrast, patients with 14v dissection had a significant higher 3-year OS than those without in TNM stages IIIb and IIIc. In multivariate analysis, 14v dissection was found to be an independent prognostic factor for GC patients with TNM stage IIIb/IIIc disease [hazard ratio (HR), 1.568; 95% confidence interval (CI): 1.186-2.072; P=0.002]. GC patients with 14v dissection had a significant lower locoregional, especially lymph node, recurrence rate than those without 14v dissection (11.7% vs. 21.1%, P=0.035). ConclusionsAdding 14v to D2 lymphadenectomy may be associated with improved 3-year OS for distal GC staged TNM IIIb/IIIc.
2015, 27(6): 588-596.
doi: 10.3978/j.issn.1000-9604.2015.12.05
Abstract:
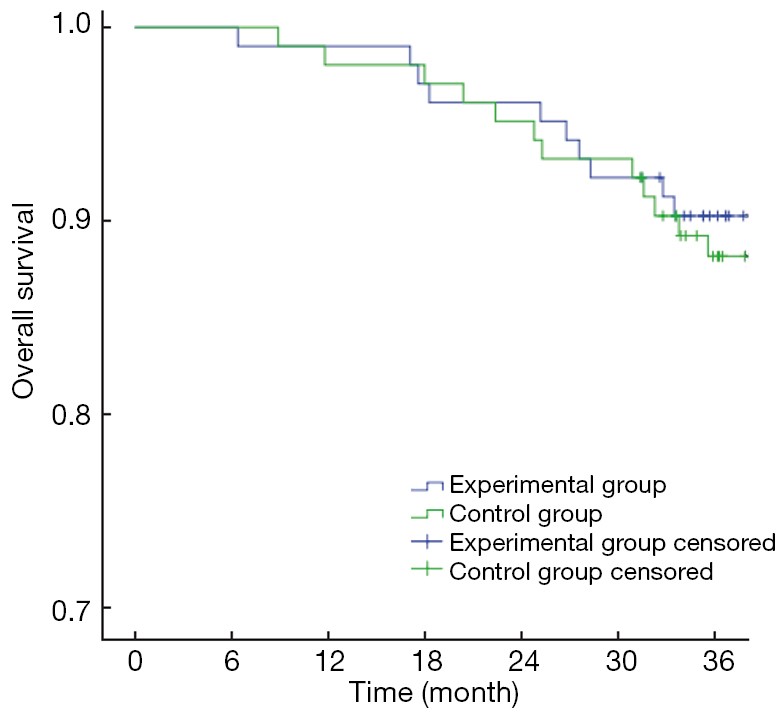
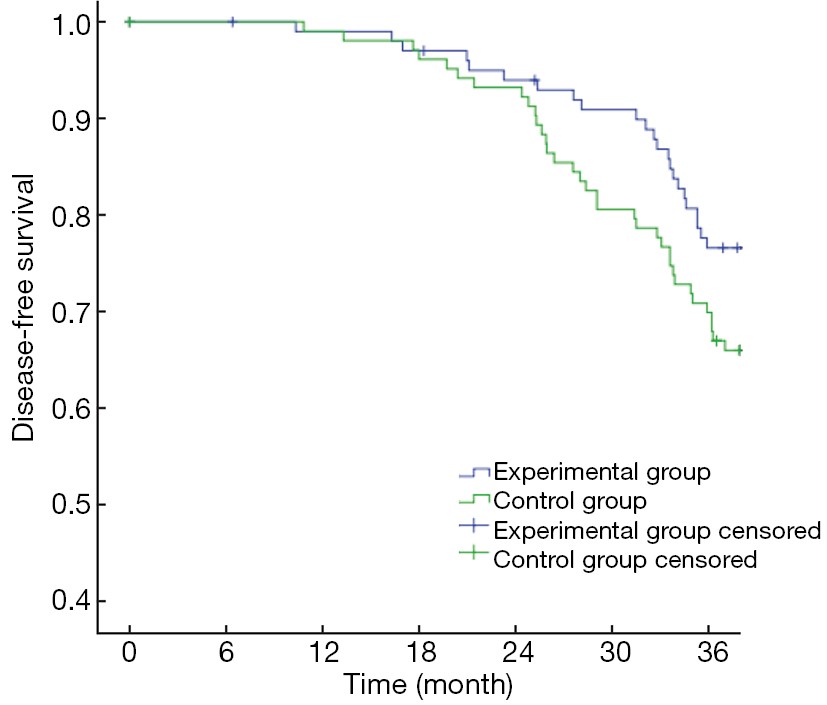
BackgroundFluorouracil-based preoperative chemoradiotherapy has become the standard treatment for stage II/III rectal cancer. In order to improve the overall survival (OS) and disease-free survival (DFS), we added oxaliplatin to the standard treatment, and compared the effectiveness of these two treatment patterns. MethodsA total of 206 patients enrolled in the prospective study had histologically confirmed rectal cancer of clinical stage II/III during July 2007 to July 2010. They were randomized into the experimental group received oxaliplatin and capecitabine in combination with radiotherapy, and the control group received capecitabine in combination with radiotherapy. All patients received surgery in 6−10 weeks after chemoradiotherapy and adjuvant chemotherapy with mFOLFOX6. The primary endpoints were DFS and OS, and the secondary endpoints included toxicity, compliance, and histopathological response. ResultsThe 3-year OS in the experimental group and the control group was 90.29% vs. 86.41% (P>0.05), and the 3-year DFS was 80.58% vs. 69.90% (P>0.05). The pathological complete remission (pCR) rates were 23.30% and 19.42%, respectively (P=0.497). The 3-year local recurrence rates were 4.85% vs. 5.83% (P=0.694), and the 3-year distant metastasis rates were 16.50% and 28.16%, respectively (P=0.045). There were no significant differences in most grade 3−4 toxicities between two groups, however, grade 3−4 diarrhea occurred in 16.50% (17/103) of the experimental group, compared with 6.80% (7/103) of the control group (P=0.030). Also, the total grade 3−4 acute toxicity showed a significant difference (10.68% vs. 21.36%, P=0.037). ConclusionsThe experimental treatment did not lead significantly improved OS and DFS, and thus longer follow-up is warranted for our patient cohort. Adding oxaliplatin to capecitabine-based preoperative chemoradiotherapy can significantly reduce metastasis, but has only minimal impact on local recurrence. Although grade 3−4 toxicity rate increased (primarily gastrointestinal toxicity), patients can stand to be followed up with allopathic treatment.

2015, 27(6): 597-603.
doi: 10.3978/j.issn.1000-9604.2015.12.07
Abstract:
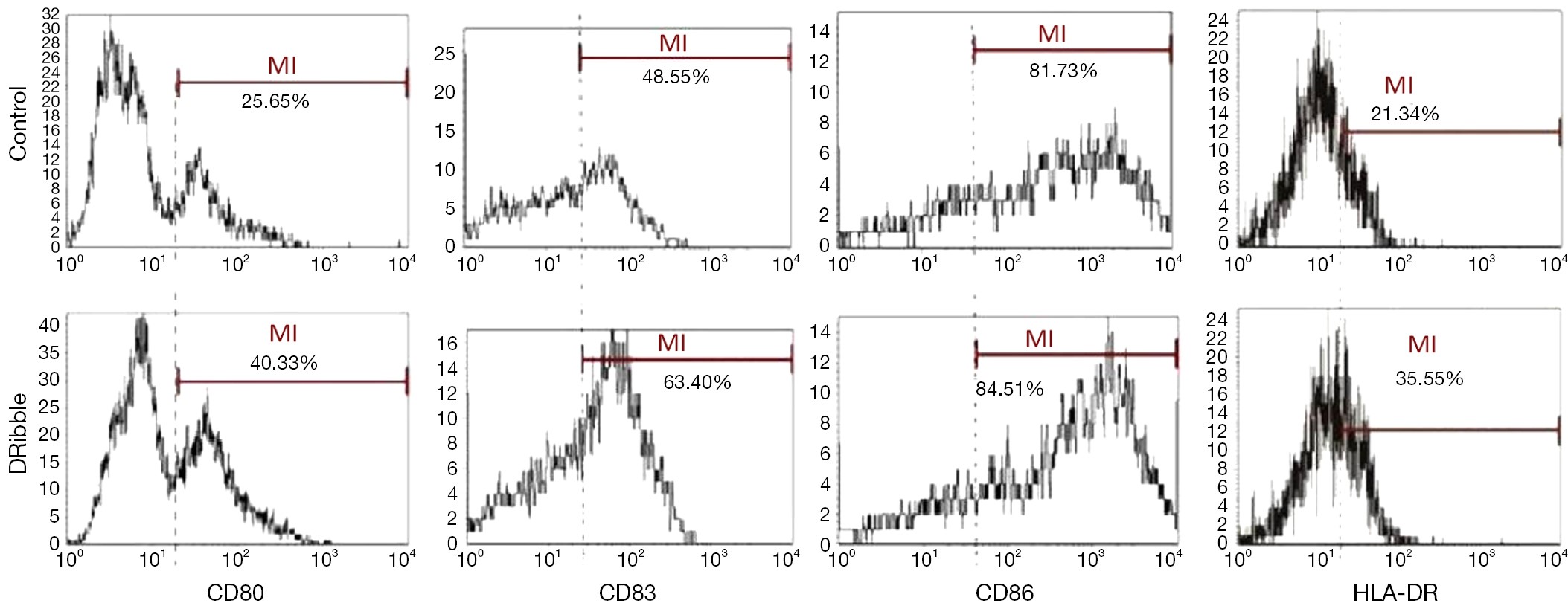
BackgroundTo induce and collect tumor-derived autophagosomes (DRibbles) from tumor cells as an antitumor vaccine by inhibiting the functions of proteasomes and lysosomes. MethodsDendritic cells (DCs) generated from peripheral blood mononuclear cell (PBMC) of hepatocellular carcinoma (HCC) patients were cocultured with DRibbles, and then surface molecules of DCs, as well as surface molecules on DCs, were determined by flow cytometry. Meanwhile, immune responses of the DCs-DRibbles were examined by mixed lymphocyte reactions. ResultsDRibbles significantly induced the expression of CD80, CD83, CD86 and HLA-DR on DCs. The enzyme-linked immunosorbnent assay (ELISA) showed that IFN-γ levels after vaccination increased than before in most patients, but CD8+ proportion of PBMC increased only in nine patients. Higher levels of IFN-γ were detected in the CD8+ cells than CD4+ T cells. These results suggested that DCs-DRibbles vaccine could induce antigen-specific cellular immune response on HCC and could prime strong CD8+ T cell responses, supporting it as a tumor vaccine candidate. ConclusionsOur results demonstrate that HCC/DRibbles-pulsed DCs immunotherapy might be deployed as an effective antitumor vaccine for HCC immunotherapy in clinical trials.
2015, 27(6): 604-610.
doi: 10.3978/j.issn.1000-9604.2015.05.05
Abstract:
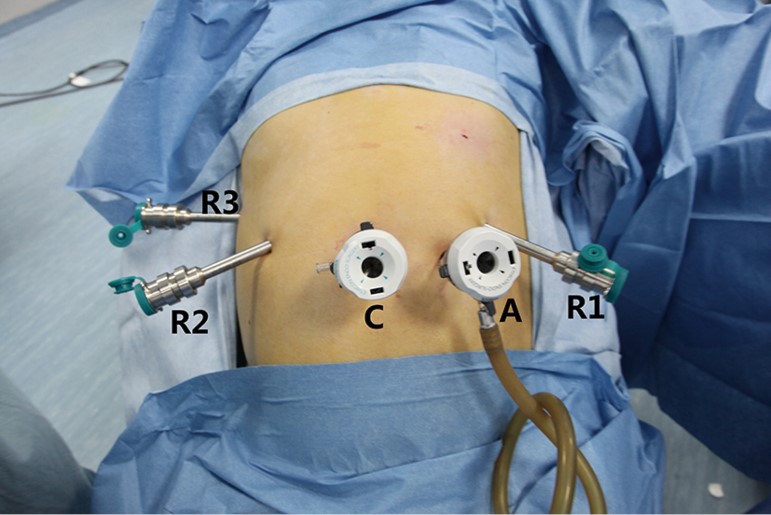
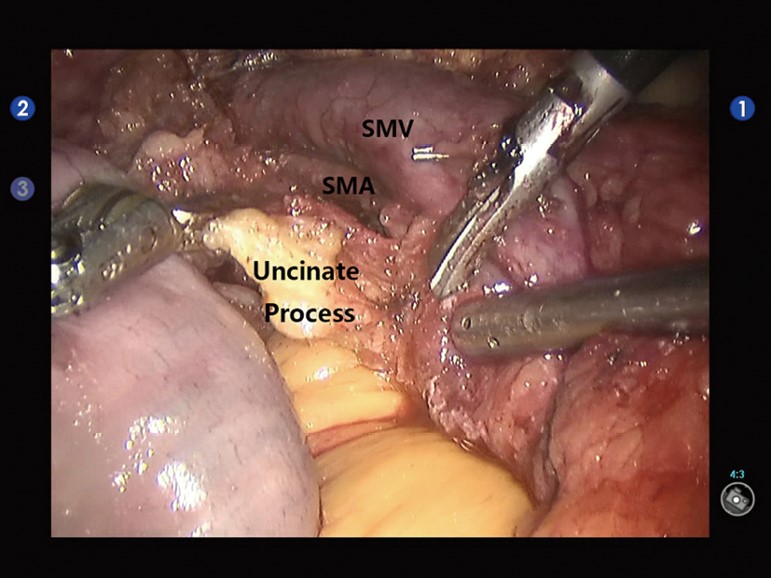
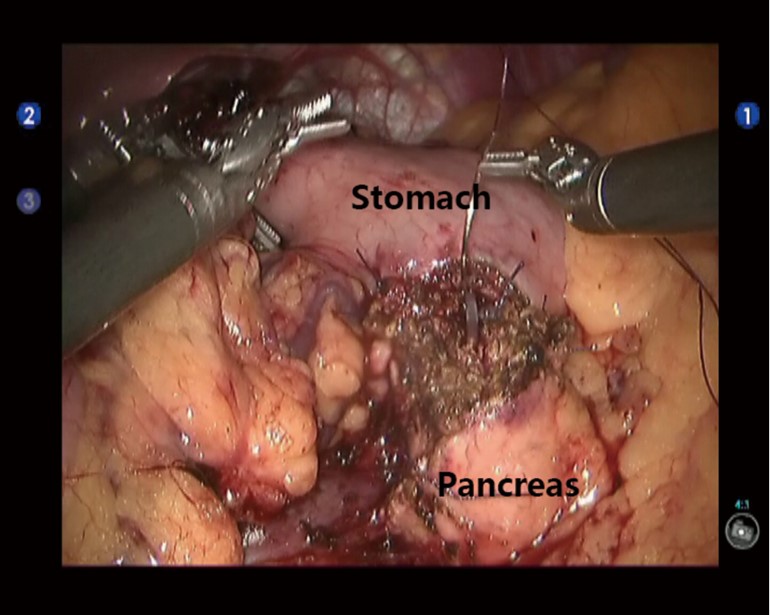
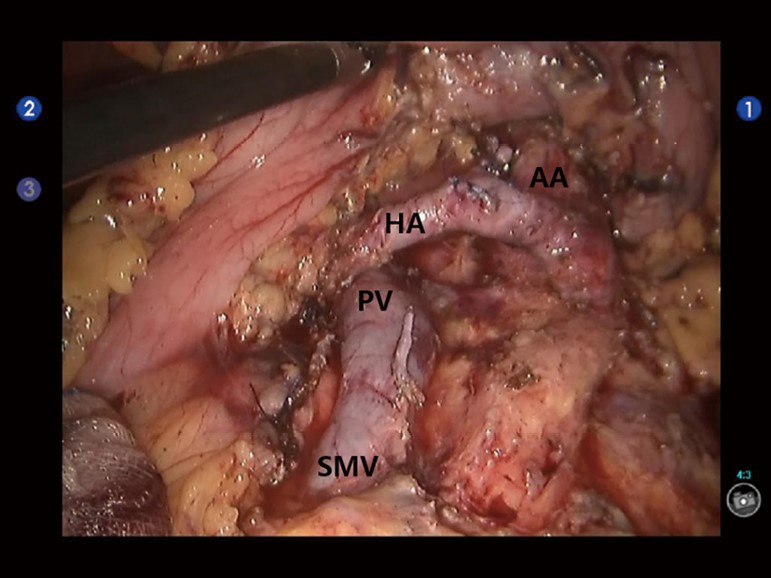
BackgroundTo explore the effectiveness, safety, and efficacy of the robot-assisted surgery in the radical resection of pancreatic ductal adenocarcinoma (PDAC). MethodsThe clinical data of 72 patients with PDAC who underwent radical resection using the da Vinci Surgical System from April 2010 to December 2014 were retrospectively analyzed. ResultsAmong these 72 patients, three were converted to conventional laparotomy due to the vascular invasion or due to the difficulties in tissue isolation from the surrounding organs. Among 39 patients who underwent the pancreatoduodenectomy, the average operative time was 395.3±118.8 min, and the mean intra-operative blood loss was 447.3±269.9 mL. Among 31 patients who underwent the distal pancreatectomy (DP), the average operative time was 185.5±74.1 min, and the mean intra-operative blood loss was 267.1±305.3 mL. In two patients who received the middle pancreatectomy (MP), the average operative time was 225 min and mean intra-operative blood loss was 100 mL. Among all the 72 patients, an average of 4.2±2.6 lymph nodes were dissected, with an average hospital stay of 22.6±10.7 days. Complications were observed in 18 patients, which included pancreatic fistula (n=11), bile leak (n=5), anastomotic bleeding (n=2), pancreatic fistula complicated with portal vein thrombosis (n=1), and anastomotic bleeding complicated with acute renal failure (n=1). Except that one patient died due to post-operative bleeding and acute renal failure, all the other patients were cured after conservative treatment. These 72 patients were followed for 1-45 (15.6±5.8) months, during which 10 patients died. Eleven patients suffered from recurrence or metastasis, among which 6 had local recurrence, 4 had liver metastasis, and 1 had ascites accompnaied with incision site tumor metastasis. ConclusionsRadical resection of PDAC by robotic surgical system is safe and feasible. It has less surgical trauma and enables faster post-operative recovery, and therefore can achieve the lymph node dissection scope and tumor resection margin required by the standards of radical resection for pancreatic cancer. Nevertheless, its long-term efficacy requires further validation.



2015, 27(6): 611-626.
doi: 10.3978/j.issn.1000-9604.2015.07.02
Abstract:
2015, 27(6): 617-618.
doi: 10.3978/j.issn.1000-9604.2015.12.04
Abstract:


