
2016 Vol.28(1)
Display Mode: |
2016, 28(1): 1-11.
doi: 10.3978/j.issn.1000-9604.2016.02.08
 Abstract
Abstract FullText HTML
FullText HTML PDF 364KB
PDF 364KB
Abstract:
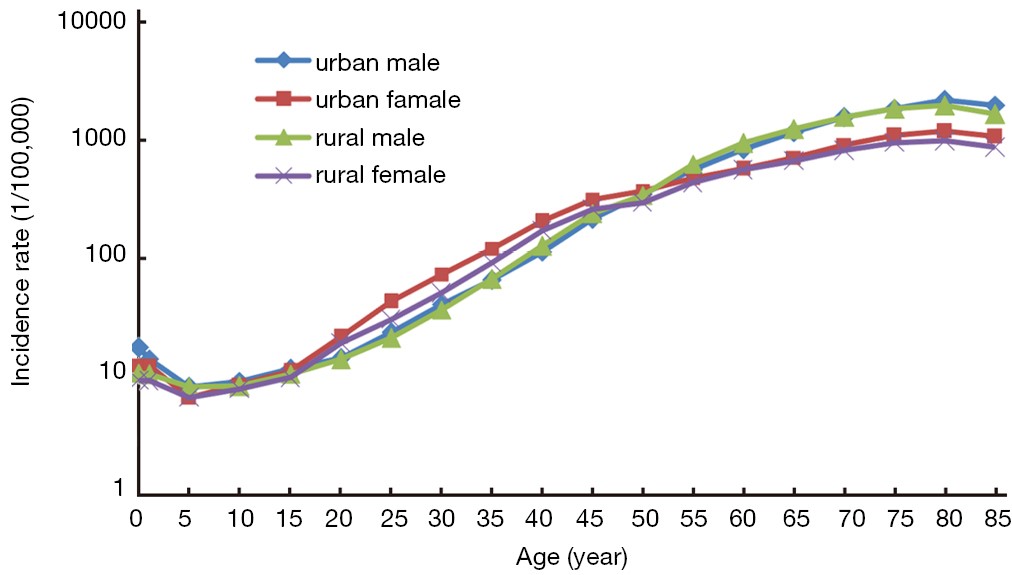
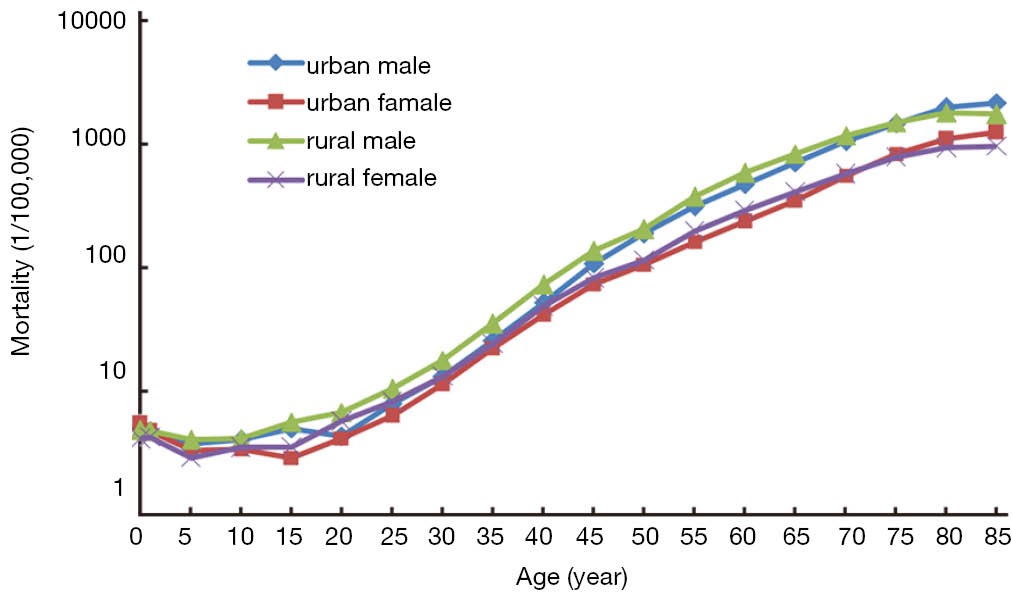
BackgroundPopulation-based cancer registration data in 2012 from all available cancer registries were collected by the National Central Cancer Registry (NCCR). NCCR estimated the numbers of new cancer cases and cancer deaths in China with compiled cancer incidence and mortality rates. MethodsIn 2015, there were 261 cancer registries submitted cancer incidence and deaths occurred in 2012. All the data were checked and evaluated based on the NCCR criteria of data quality. Qualified data from 193 registries were used for cancer statistics analysis as national estimation. The pooled data were stratified by area (urban/rural), gender, age group [0, 1–4, 5–9, 10–14, …, 85+] and cancer type. New cancer cases and deaths were estimated using age-specific rates and corresponding national population in 2012. The Chinese census data in 2000 and Segi’s population were applied for age-standardized rates. All the rates were expressed per 100,000 person-year. ResultsQualified 193 cancer registries (74 urban and 119 rural registries) covered 198,060,406 populations (100,450,109 in urban and 97,610,297 in rural areas). The percentage of cases morphologically verified (MV%) and death certificate-only cases (DCO%) were 69.13% and 2.38%, respectively, and the mortality to incidence rate ratio (M/I) was 0.62. A total of 3,586,200 new cancer cases and 2,186,600 cancer deaths were estimated in China in 2012. The incidence rate was 264.85/100,000 (289.30/100,000 in males, 239.15/100,000 in females), the age-standardized incidence rates by Chinese standard population (ASIRC) and by world standard population (ASIRW) were 191.89/100,000 and 187.83/100,000 with the cumulative incidence rate (0–74 age years old) of 21.82%. The cancer incidence, ASIRC and ASIRW in urban areas were 277.17/100,000, 195.56/100,000 and 190.88/100,000 compared to 251.20/100,000, 187.10/100,000 and 183.91/100,000 in rural areas, respectively. The cancer mortality was 161.49/100,000 (198.99/100,000 in males, 122.06/100,000 in females), the age-standardized mortality rates by Chinese standard population (ASMRC) and by world standard population (ASMRW) were 112.34/100,000 and 111.25/100,000, and the cumulative mortality rate (0–74 years old) was 12.61%. The cancer mortality, ASMRC and ASMRW were 159.00/100,000, 107.231/100,000 and 106.13/100,000 in urban areas, 164.24/100,000, 118.22/100,000 and 117.06/100,000 in rural areas, respectively. Cancers of lung, stomach, liver, colorectum, esophagus, female breast, thyroid cervix, brain tumor and pancreas were the most common cancers, accounting for about 77.4% of all cancer new cases. Lung cancer, liver cancer, stomach cancer, esophageal cancer, colorectal cancer, pancreatic cancer, female breast cancer, brain tumor, leukemia and lymphoma were the leading causes of cancer death, accounting for about 84.5% of all cancer deaths. The cancer spectrum showed difference between urban and rural, males and females both in incidence and mortality rates. ConclusionsCancer surveillance information in China is making great progress with the increasing number of cancer registries, population coverage and the improving data quality. Cancer registration plays a fundamental role in cancer control by providing basic information on population-based cancer incidence, mortality, survival and time trend. The disease burden of cancer is serious in China, so that, cancer prevention and control, including health education, health promotion, cancer screening and cancer care services in China, should be enhanced.
2016, 28(1): 12-18.
doi: 10.3978/j.issn.1000-9604.2016.02.07
Abstract:
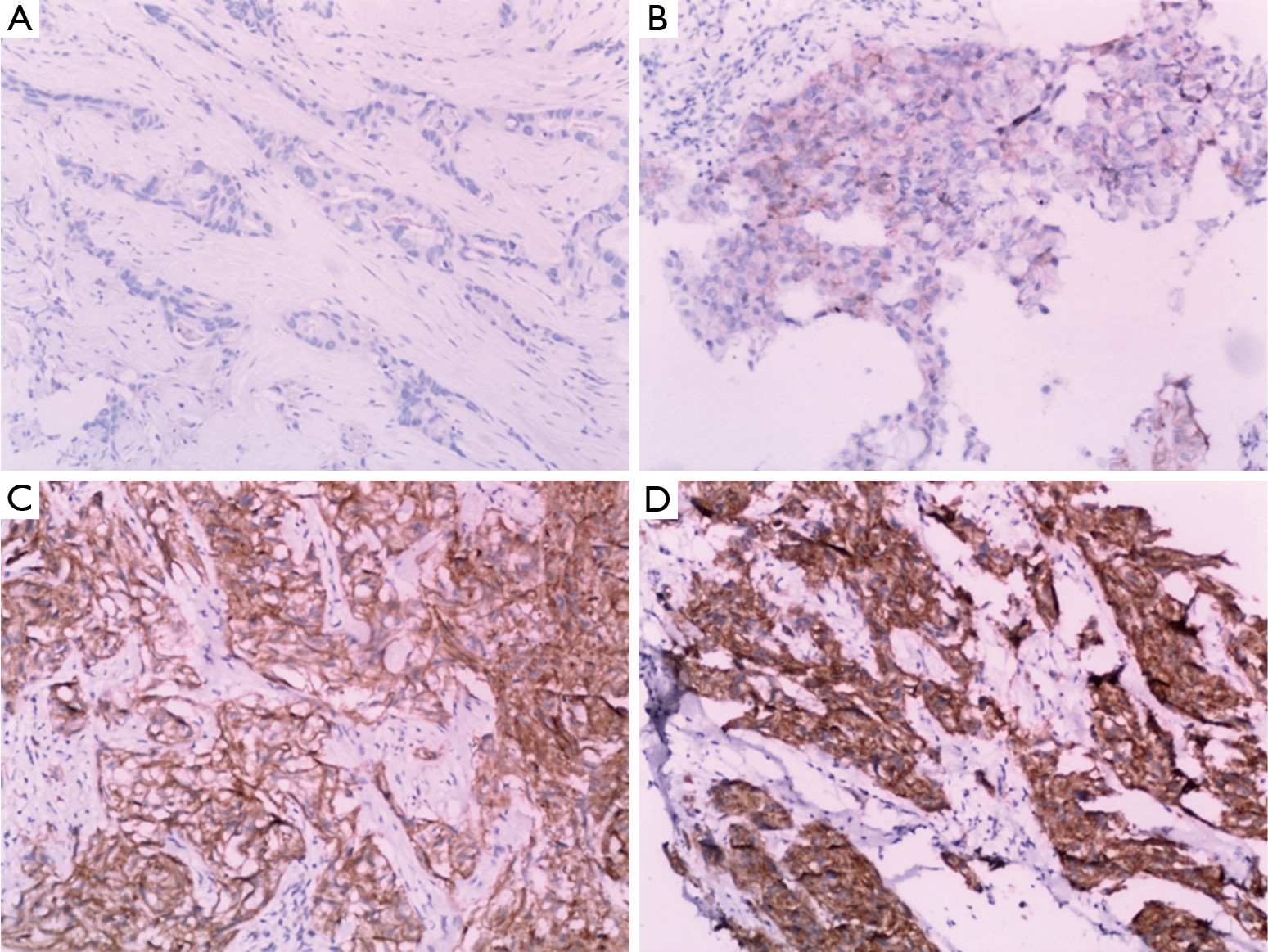
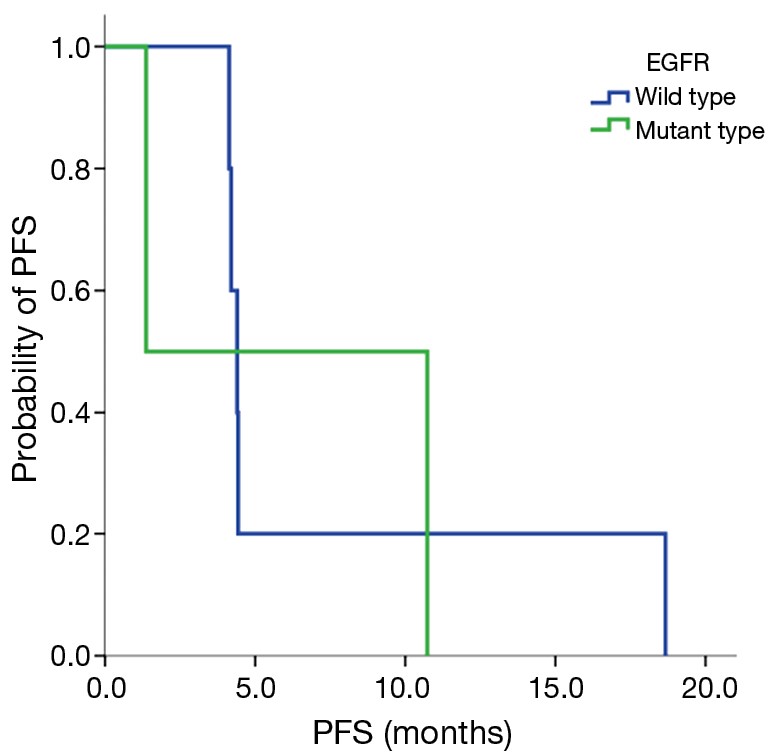
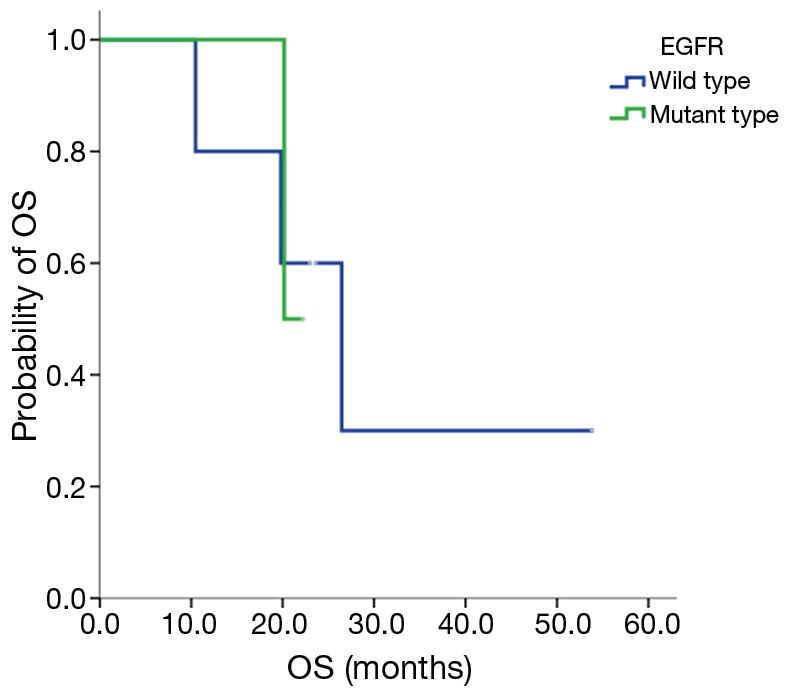
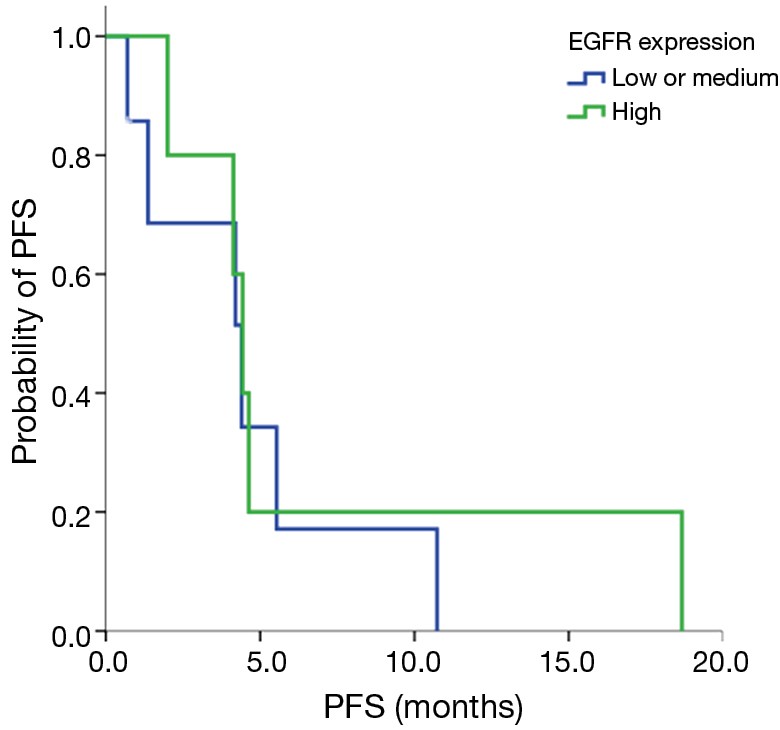
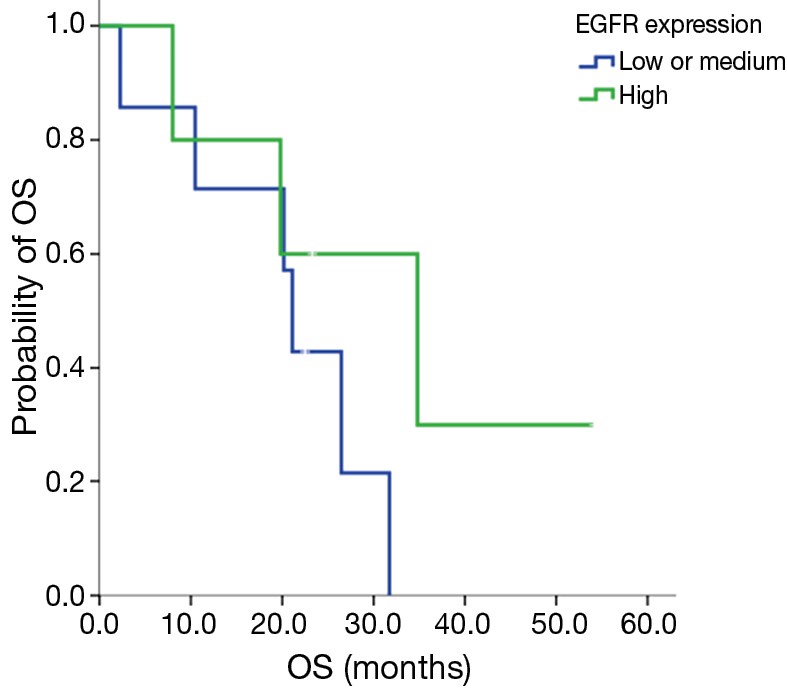
BackgroundTo determine the safety and therapeutic efficacy of nimotuzumab (h-R3) combined with docetaxel in advanced non-small-cell lung cancer (NSCLC) patients who have failed to respond to prior first-line chemotherapy. MethodsIn this single-center, open-label, dose-escalating phase I trial, patients with epidermal growth factor receptor (EGFR)-expressing stage IV NSCLC were treated with nimotuzumab plus docetaxel according to a dose escalation schedule. The safety and efficacy of the combination treatment were observed and analyzed. ResultsThere were 12 patients with EGFR-expressing stage IV NSCLC enrolled. The dose of nimotuzumab was escalated from 200 to 600 mg/week. The longest administration of study drug was 40 weeks at the 600 mg/week dose level. Grade III–IV toxicities included neutropenia and fatigue, and other toxicities included rash. Dose-limiting toxicity occurred with Grade 3 fatigue at the 200 mg dose level of nimotuzumab and Grade 4 neutropenia with pneumonia at the 600 mg dose level of nimotuzumab. No objective responses were observed, and stable disease was observed in eight patients (66.7%). The median progression-free survival (PFS) was 4.4 months in all patients, 1.3 months in patients with the EGFR mutation, and 4.4 months in those with wild type EGFR (EGFR WT). The median survival time (MST) was 21.1 months in all patients, 21.1 months in patients with EGFR mutation, and 26.4 months in patients with EGFR WT. ConclusionsNimotuzumab and docetaxel combination therapy was found to be well tolerated and efficacious. Further study of nimotuzumab is warranted in advanced NSCLC patients.
2016, 28(1): 19-28.
doi: 10.3978/j.issn.1000-9604.2016.02.06
Abstract:
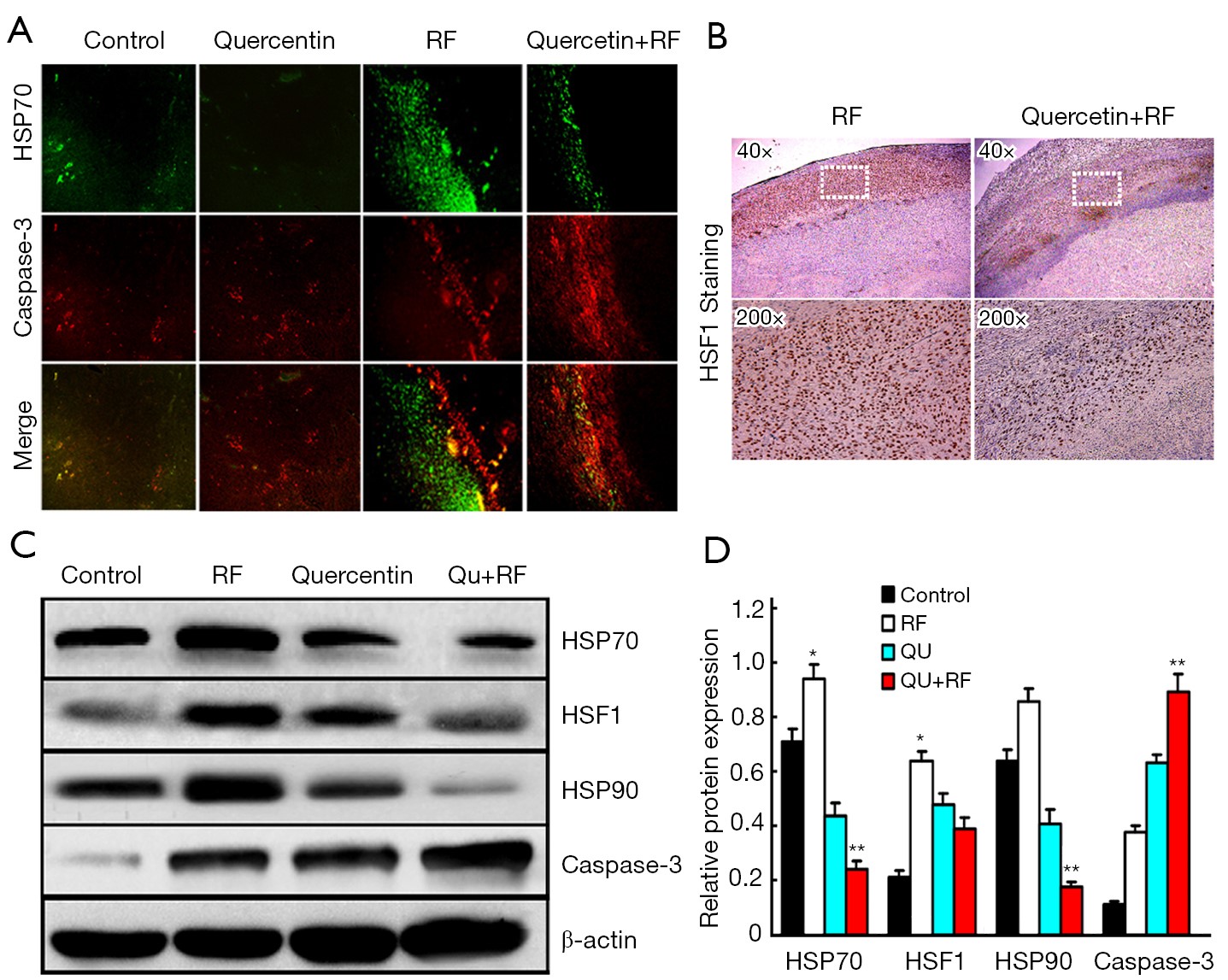
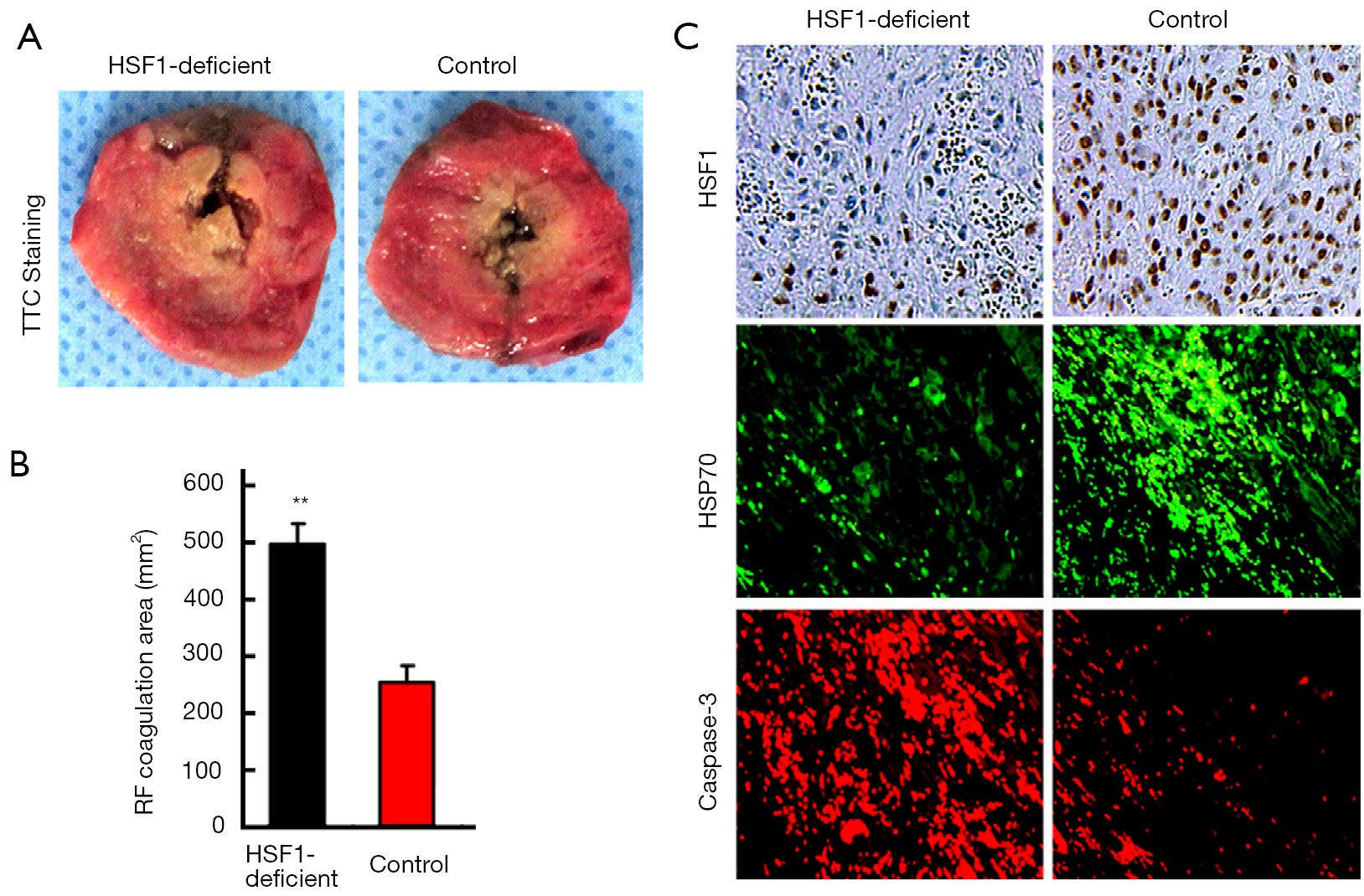
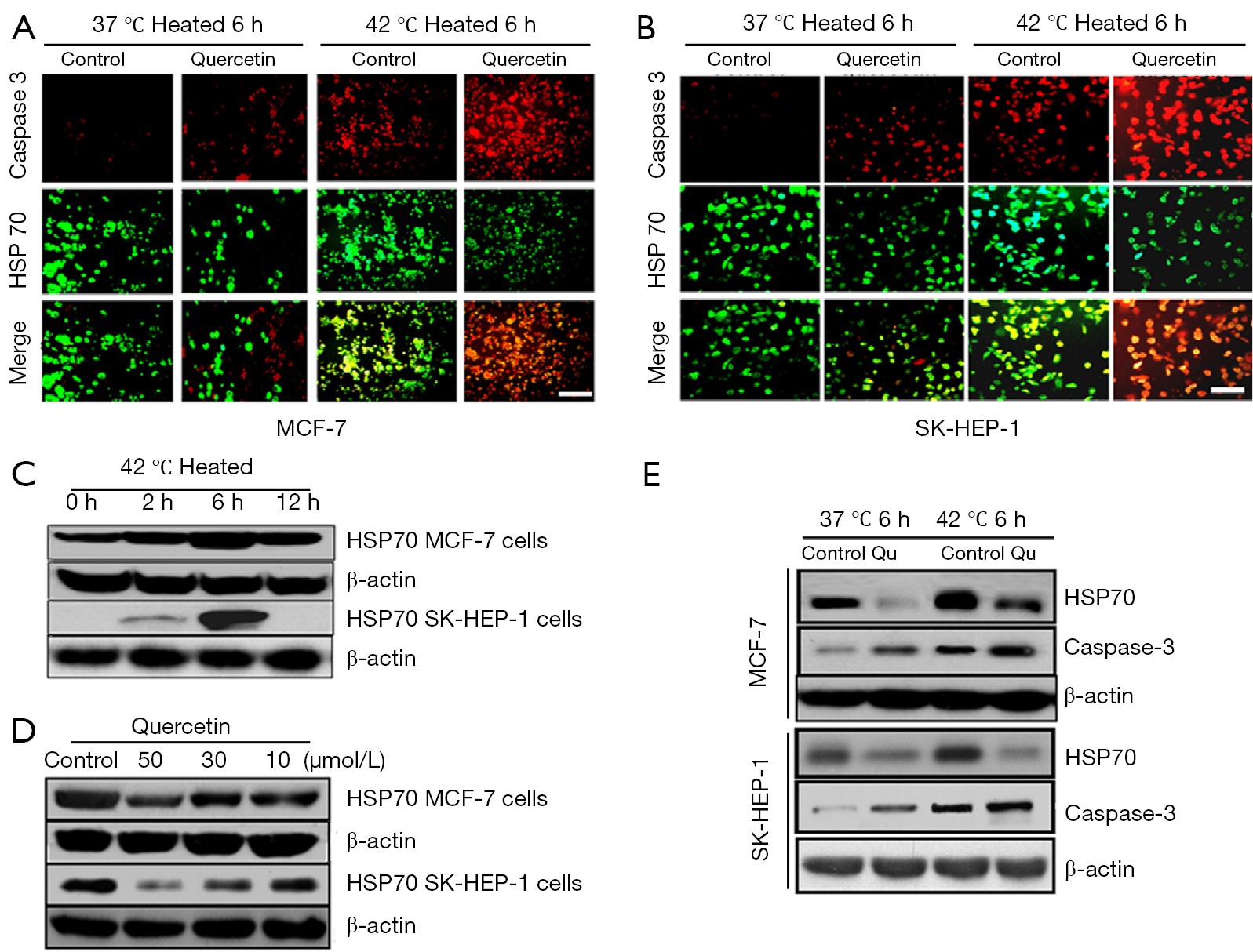
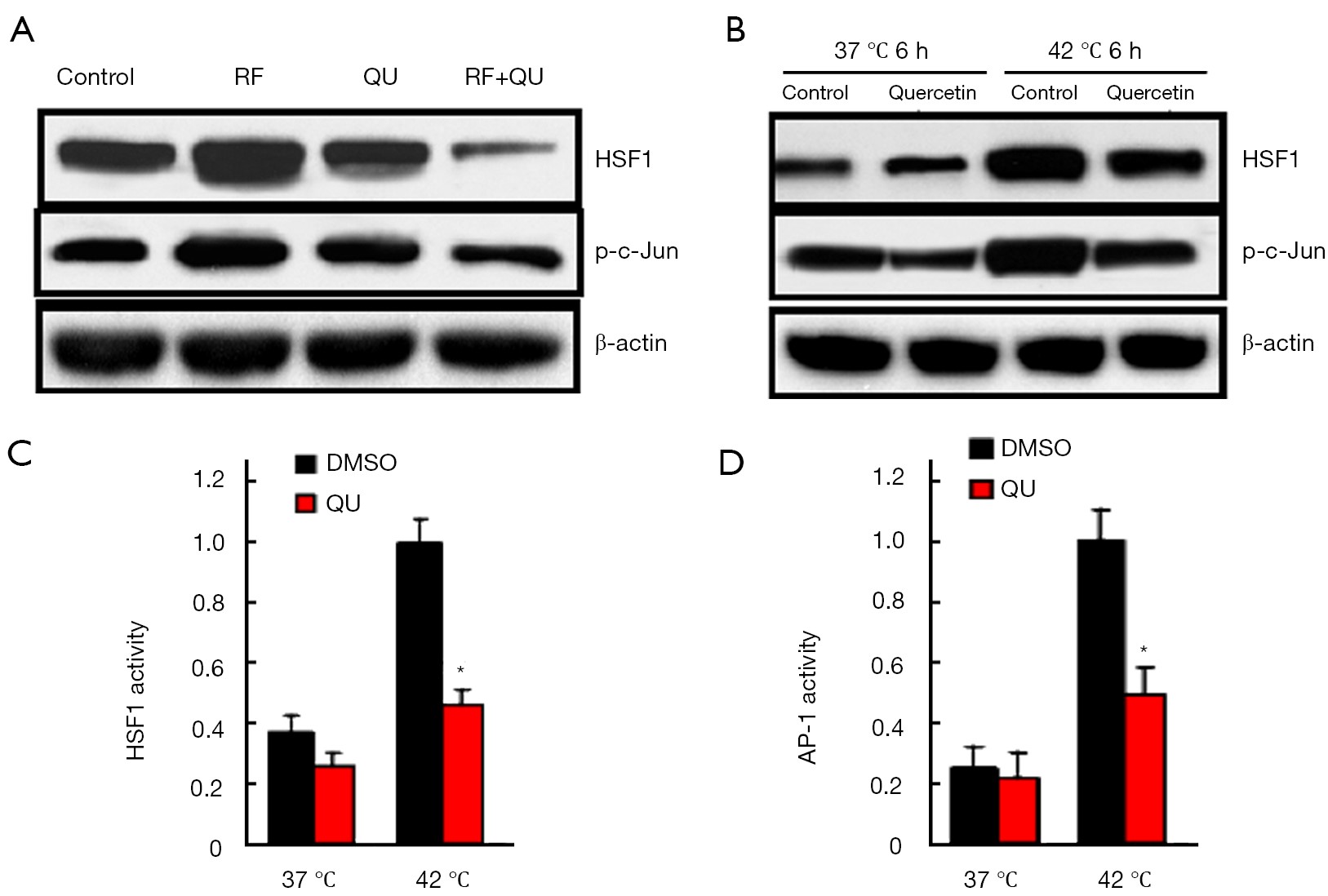
BackgroundWe investigated the effect of a small molecular inhibitor of heat shock protein (HSP), quercetin, on tumor radiofrequency (RF) ablation, and explored the underlying molecular mechanisms. MethodsIn in vivo study, rats with R3230 breast adenocarcinoma were sacrificed 24 h post-treatment and gross coagulation areas were compared, and next, randomized into four treatment arms (control, quercetin alone, RF alone, and combination) for Kaplan-Meier analysis of defined endpoint survival. Then the distribution and expression levels of heat shock protein 70 (HSP70), cleaved caspase-3 and heat shock factor 1 (HSF1) were analyzed after different treatments. In in vitro study, we used quercetin to promote SK-HEP-1 (hepatic) and MCF-7 (breast) cancer cell apoptosis in heat shock cell model, and siRNA was used to block c-Jun and to explore the role of activating protein-1 (AP-1) signaling pathways. ResultsWe found the effects of quercetin plus RFA resulted in increase on the tumor destruction/endpoint survival (26.5±3.4 d) in vivo, compared with RF alone (17.6±2.5 d) and quercetin alone (15.7±3.1 d). Most importantly, quercetin-induced cancer cell death required the presence of HSF1 in animal model. Furthermore, quercetin directly down-regulated expression of HSF1 in vitro, which our findings have revealed, required the activation of AP-1 signaling pathways by loss-of-function analysis using siRNA mediated targeting of c-Jun. ConclusionsThese results indicated a protective role of quercetin in tumor ablation and highlighted a novel mechanism involving HSP70 with HSF1 pathway in thermal ablation of solid tumors.

2016, 28(1): 29-49.
doi: 10.3978/j.issn.1000-9604.2016.01.03
Abstract:
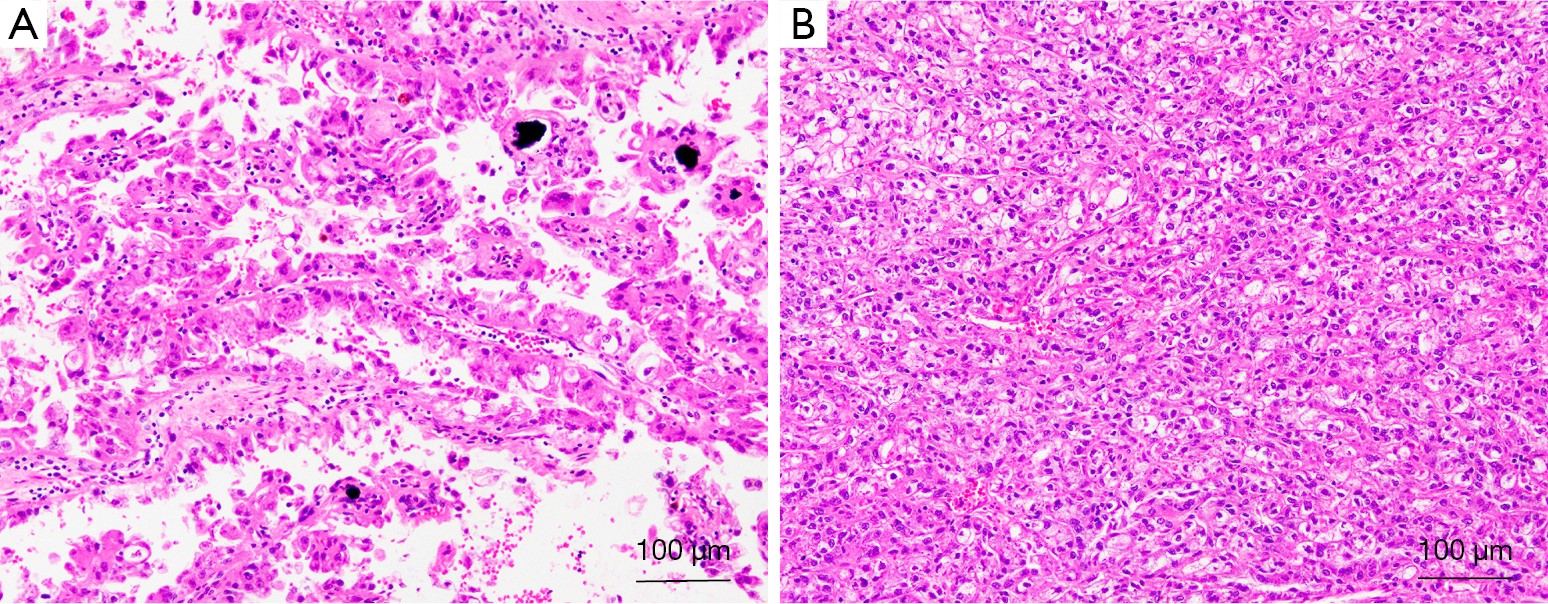
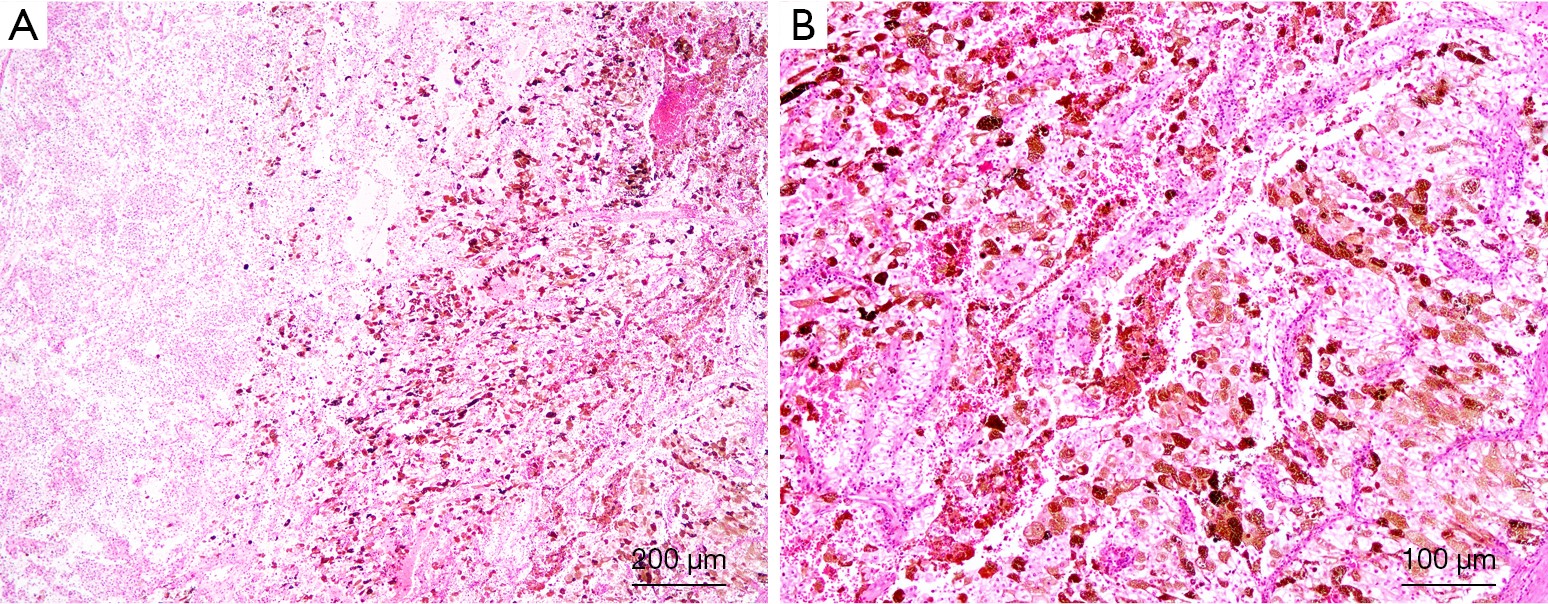
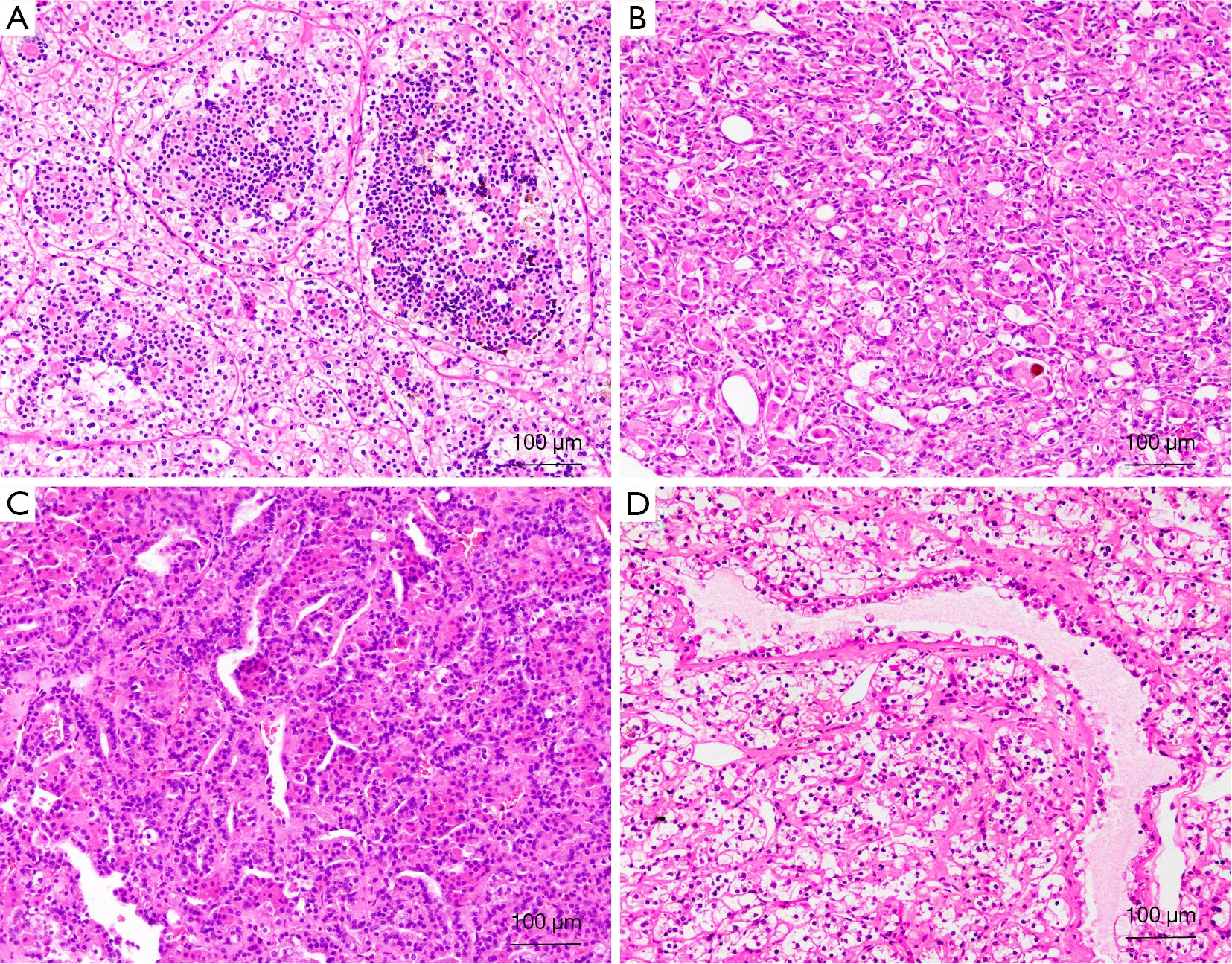
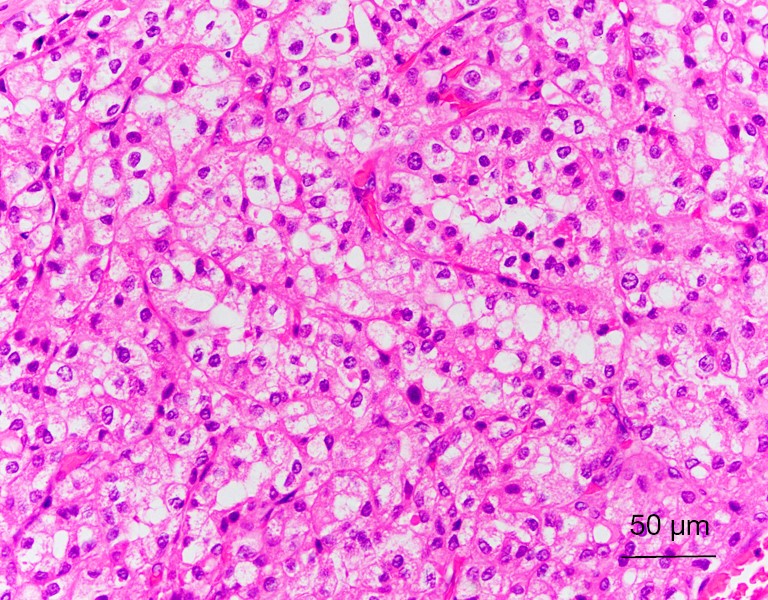
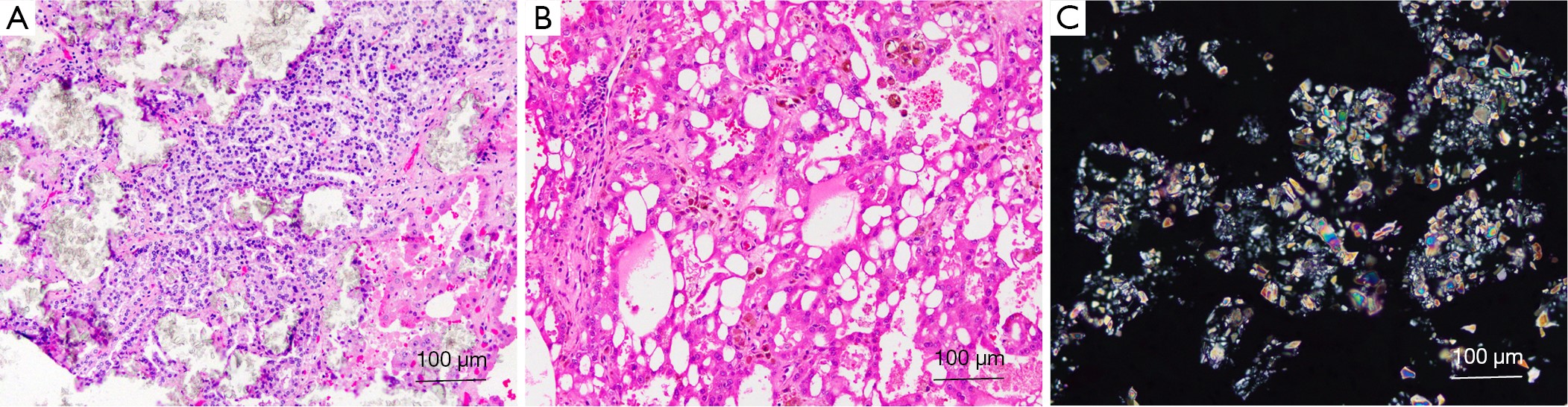
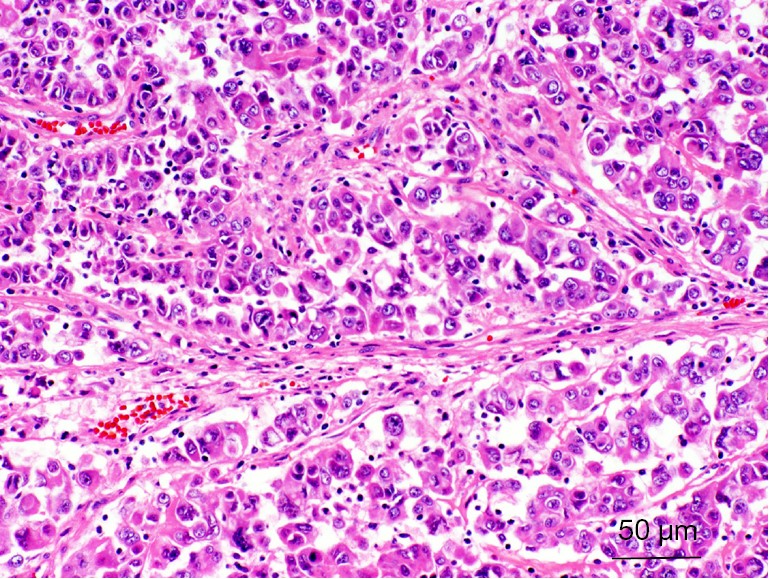
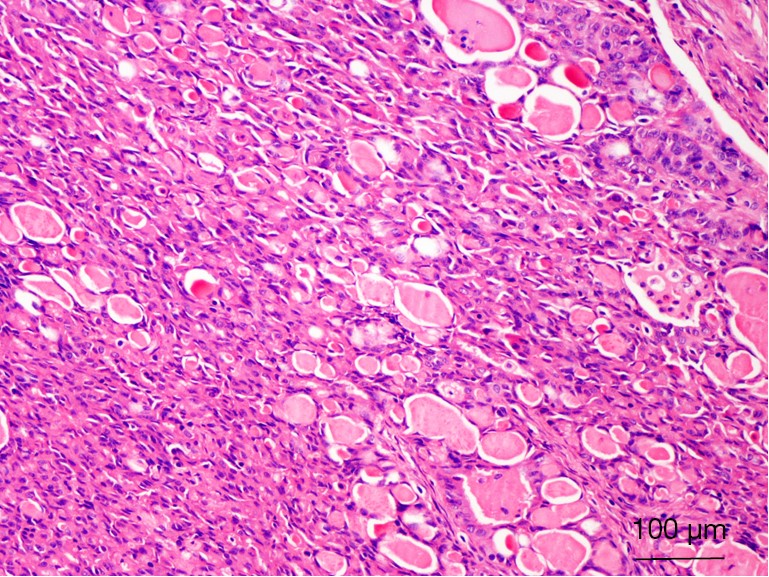
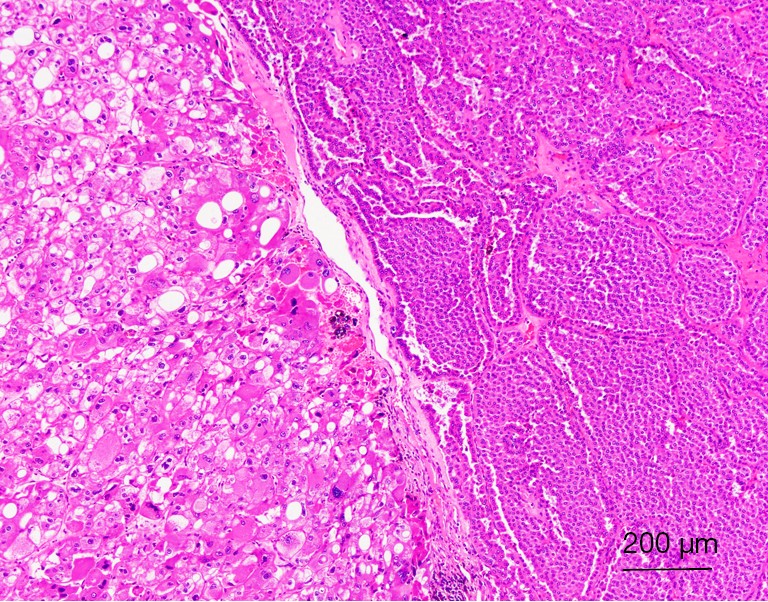
Renal cell carcinoma (RCC) compromises multiple types and has been emerging dramatically over the recent several decades. Advances and consensus have been achieved targeting common RCCs, such as clear cell carcinoma, papillary RCC and chromophobe RCC. Nevertheless, little is known on the characteristics of several newly-identified RCCs, including clear cell (tubulo) papillary RCC, Xp11 translocation RCC, t(6;11) RCC, succinate dehydrogenase (SDH)-deficient RCC, acquired cystic disease-associated RCC, hereditary leiomyomatosis RCC syndrome-associated RCC, ALK translocation RCC, thyroid-like follicular RCC, tubulocystic RCC and hybrid oncocytic/chromophobe tumors (HOCT). In current review, we will collect available literature of these newly-described RCCs, analyze their clinical pathologic characteristics, discuss their morphologic and immunohistologic features, and finally summarize their molecular and genetic evidences. We expect this review would be beneficial for the understanding of RCCs, and eventually promote clinical management strategies.
Renal cell carcinoma (RCC) compromises multiple types and has been emerging dramatically over the recent several decades. Advances and consensus have been achieved targeting common RCCs, such as clear cell carcinoma, papillary RCC and chromophobe RCC. Nevertheless, little is known on the characteristics of several newly-identified RCCs, including clear cell (tubulo) papillary RCC, Xp11 translocation RCC, t(6;11) RCC, succinate dehydrogenase (SDH)-deficient RCC, acquired cystic disease-associated RCC, hereditary leiomyomatosis RCC syndrome-associated RCC, ALK translocation RCC, thyroid-like follicular RCC, tubulocystic RCC and hybrid oncocytic/chromophobe tumors (HOCT). In current review, we will collect available literature of these newly-described RCCs, analyze their clinical pathologic characteristics, discuss their morphologic and immunohistologic features, and finally summarize their molecular and genetic evidences. We expect this review would be beneficial for the understanding of RCCs, and eventually promote clinical management strategies.

2016, 28(1): 50-57.
doi: 10.3978/j.issn.1000-9604.2016.02.02
Abstract:
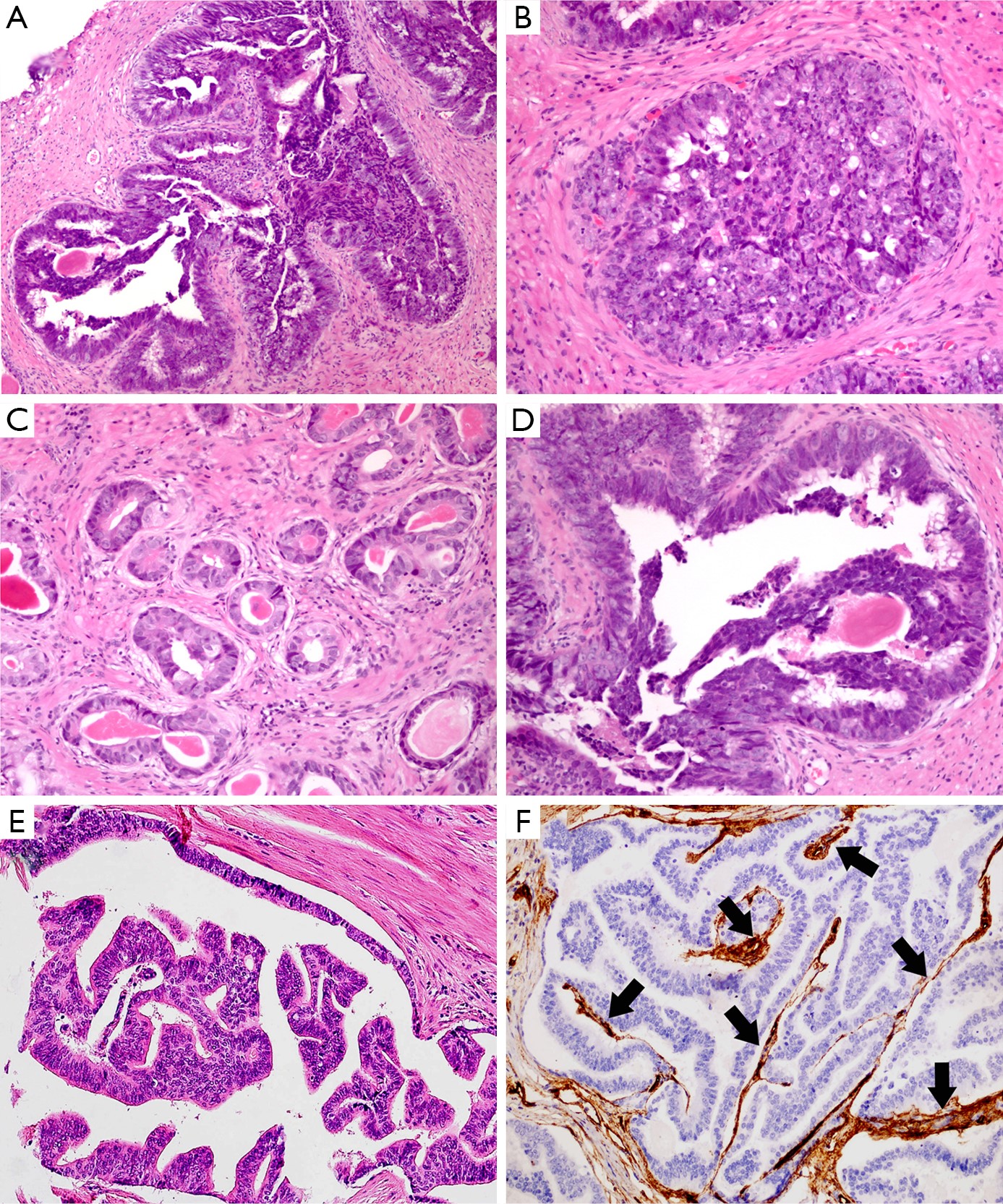
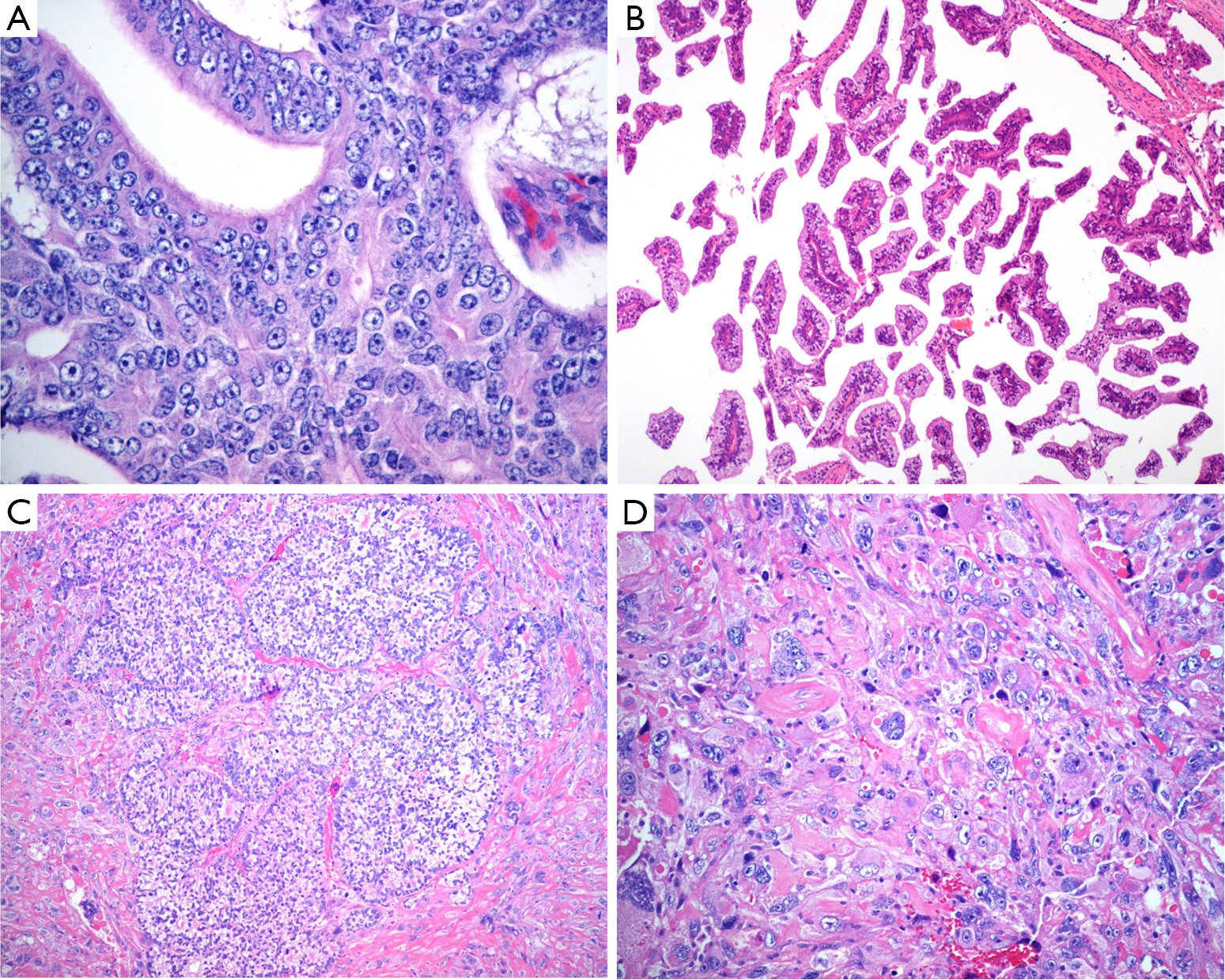
Since initially described in 1967, prostatic ductal adenocarcinoma (PDA) has engendered a series of controversies on its origin, histological features, and biological behavior. Owing to the improvement of molecular biological technique, there are some updated findings on the characteristics of PDA. In the current review, we will mainly analyze its origin, clinical manifestations, morphological features, differential diagnosis, immunophenotype and molecular genetics, with the purpose of enhancing recognition of this tumor and making a correct diagnosis and treatment choice.
Since initially described in 1967, prostatic ductal adenocarcinoma (PDA) has engendered a series of controversies on its origin, histological features, and biological behavior. Owing to the improvement of molecular biological technique, there are some updated findings on the characteristics of PDA. In the current review, we will mainly analyze its origin, clinical manifestations, morphological features, differential diagnosis, immunophenotype and molecular genetics, with the purpose of enhancing recognition of this tumor and making a correct diagnosis and treatment choice.
2016, 28(1): 58-64.
doi: 10.3978/j.issn.1000-9604.2016.02.04
Abstract:
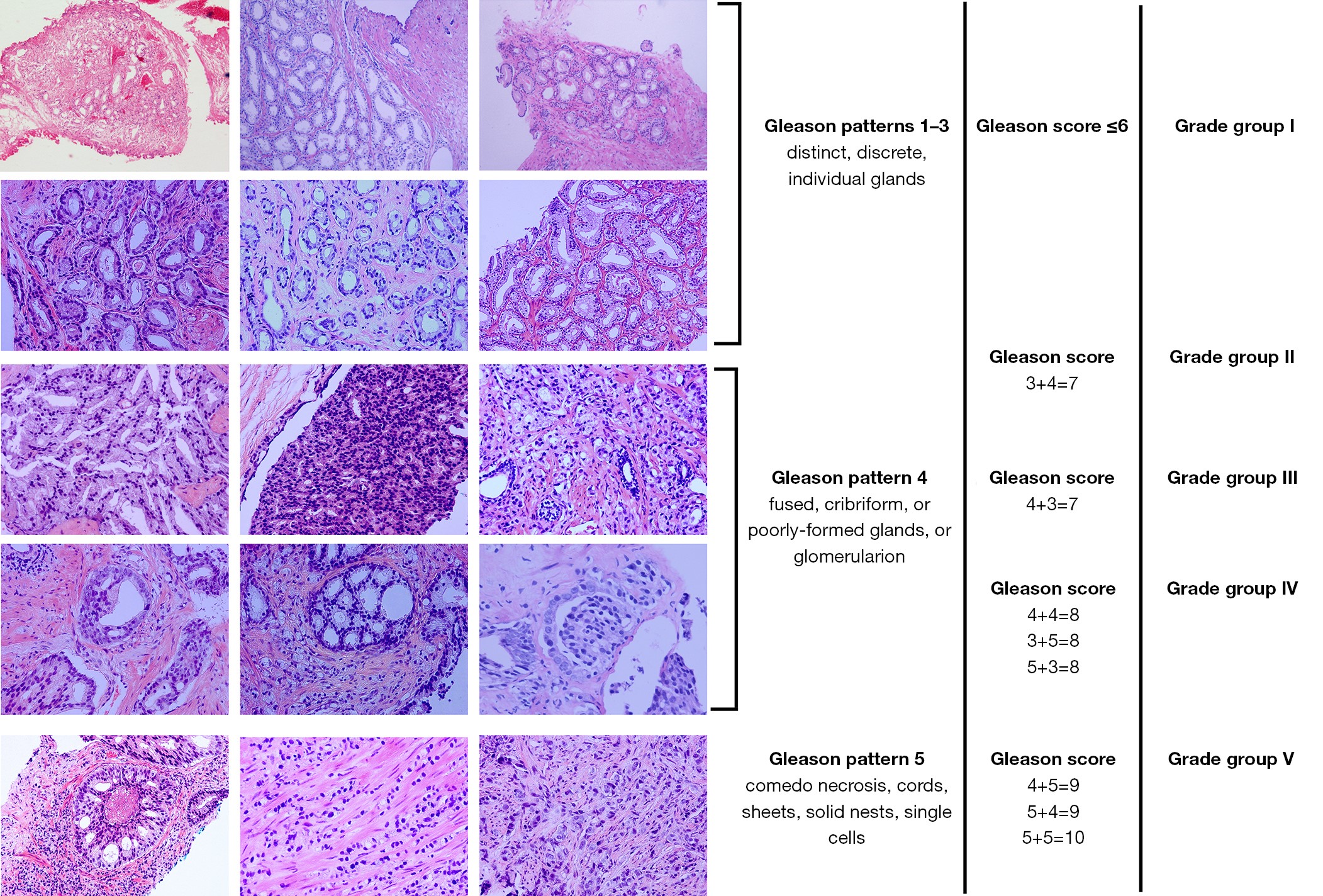
The Gleason grading system for prostate adenocarcinoma has evolved from its original scheme established in the 1960s–1970s, to a significantly modified system after two major consensus meetings conducted by the International Society of Urologic Pathology (ISUP) in 2005 and 2014, respectively. The Gleason grading system has been incorporated into the WHO classification of prostate cancer, the AJCC/UICC staging system, and the NCCN guidelines as one of the key factors in treatment decision. Both pathologists and clinicians need to fully understand the principles and practice of this grading system. We here briefly review the historical aspects of the original scheme and the recent developments of Gleason grading system, focusing on major changes over the years that resulted in the modern Gleason grading system, which has led to a new “Grade Group” system proposed by the 2014 ISUP consensus, and adopted by the 2016 WHO classification of tumours of the prostate.
The Gleason grading system for prostate adenocarcinoma has evolved from its original scheme established in the 1960s–1970s, to a significantly modified system after two major consensus meetings conducted by the International Society of Urologic Pathology (ISUP) in 2005 and 2014, respectively. The Gleason grading system has been incorporated into the WHO classification of prostate cancer, the AJCC/UICC staging system, and the NCCN guidelines as one of the key factors in treatment decision. Both pathologists and clinicians need to fully understand the principles and practice of this grading system. We here briefly review the historical aspects of the original scheme and the recent developments of Gleason grading system, focusing on major changes over the years that resulted in the modern Gleason grading system, which has led to a new “Grade Group” system proposed by the 2014 ISUP consensus, and adopted by the 2016 WHO classification of tumours of the prostate.
2016, 28(1): 65-71.
doi: 10.3978/j.issn.1000-9604.2016.01.05
Abstract:
The incidence of prostate cancer (PCa) is rising steadily among males in many countries. Serum prostate-specific antigen (PSA) is widely applied to clinical diagnosis and screening of PCa. However, the so-called grey area of PSA levels 4.0–10.0 ng/mL has a low specificity of 25–40% resulting in a high rate of negative biopsy and overtreatment. So in order to treat PCa patients in early stage, there is an urgent need for new biomarkers in PCa diagnosis. The PCA3 gene, a non-coding RNA (ncRNA) that is highly expressed in prostate cancer (PCa) cells, has been identified as a molecular biomarkers to detect PCa, of which PCA3 has already under clinical application. PCA3 is strongly overexpressed in malignant prostate tissue compared to benign or normal adjacent one. Newly, PCA3 is considered to be a promising biomarker in clinical diagnosis and targeted therapy. The diagnostic significance of PCA3, however, is awaiting further researches. Moreover, it has been demonstrated recently that TMPRSS2-ERG gene fusion is identified as the predominant genetic change in patients diagnosed with PCa. Recent study revealed that combination of the PCA3 and TMPRSS2-ERG gene fusion test optimizes PCa detection compared with that of single biomarker, which would lead to a considerable reduction of the number of prostate biopsies. In this review, we focused on the potential use of PCA3 and TMPRSS2-ERG gene fusion detection in the diagnosis of PCa.
The incidence of prostate cancer (PCa) is rising steadily among males in many countries. Serum prostate-specific antigen (PSA) is widely applied to clinical diagnosis and screening of PCa. However, the so-called grey area of PSA levels 4.0–10.0 ng/mL has a low specificity of 25–40% resulting in a high rate of negative biopsy and overtreatment. So in order to treat PCa patients in early stage, there is an urgent need for new biomarkers in PCa diagnosis. The PCA3 gene, a non-coding RNA (ncRNA) that is highly expressed in prostate cancer (PCa) cells, has been identified as a molecular biomarkers to detect PCa, of which PCA3 has already under clinical application. PCA3 is strongly overexpressed in malignant prostate tissue compared to benign or normal adjacent one. Newly, PCA3 is considered to be a promising biomarker in clinical diagnosis and targeted therapy. The diagnostic significance of PCA3, however, is awaiting further researches. Moreover, it has been demonstrated recently that TMPRSS2-ERG gene fusion is identified as the predominant genetic change in patients diagnosed with PCa. Recent study revealed that combination of the PCA3 and TMPRSS2-ERG gene fusion test optimizes PCa detection compared with that of single biomarker, which would lead to a considerable reduction of the number of prostate biopsies. In this review, we focused on the potential use of PCA3 and TMPRSS2-ERG gene fusion detection in the diagnosis of PCa.
2016, 28(1): 72-79.
doi: 10.3978/j.issn.1000-9604.2016.01.01
Abstract:
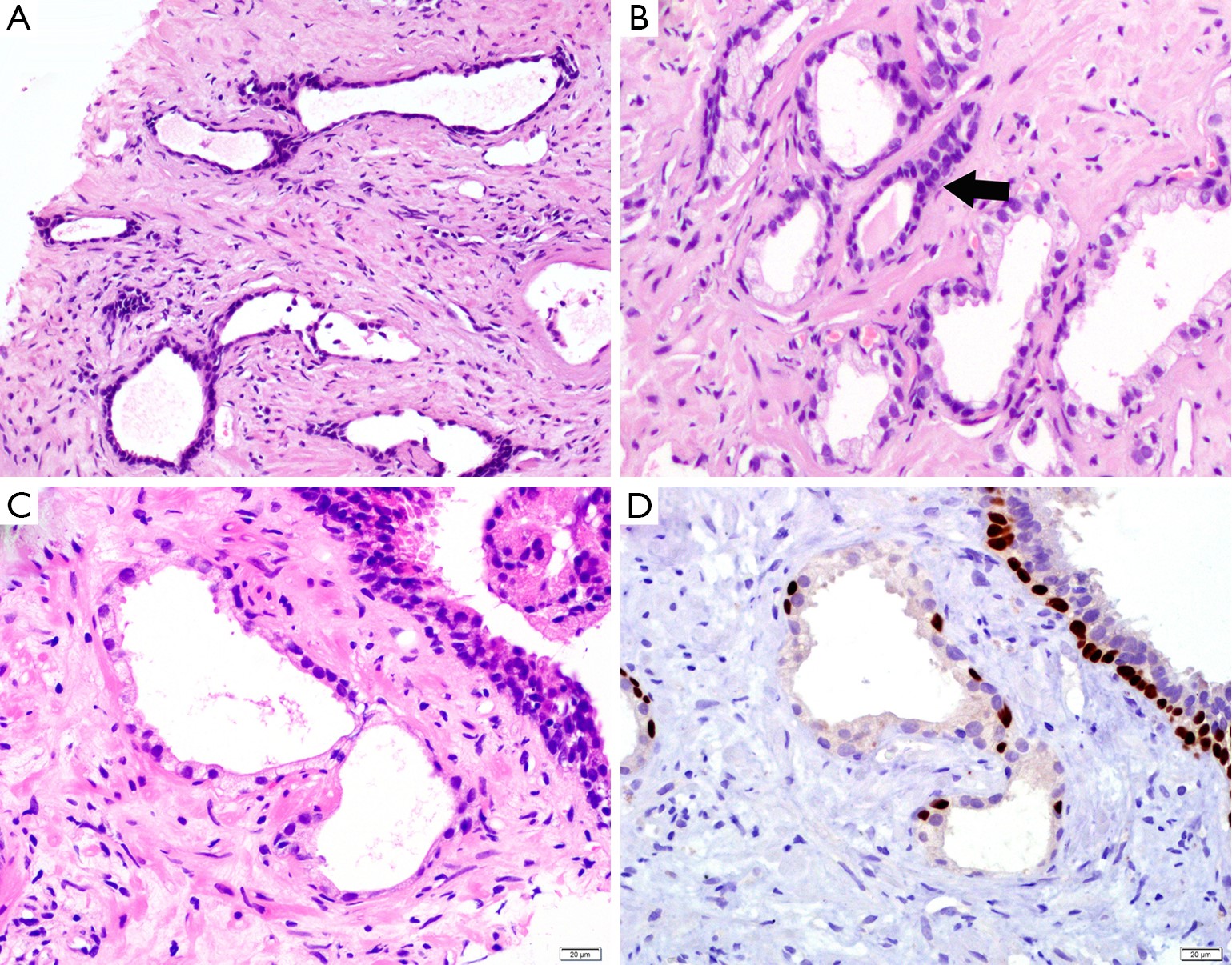
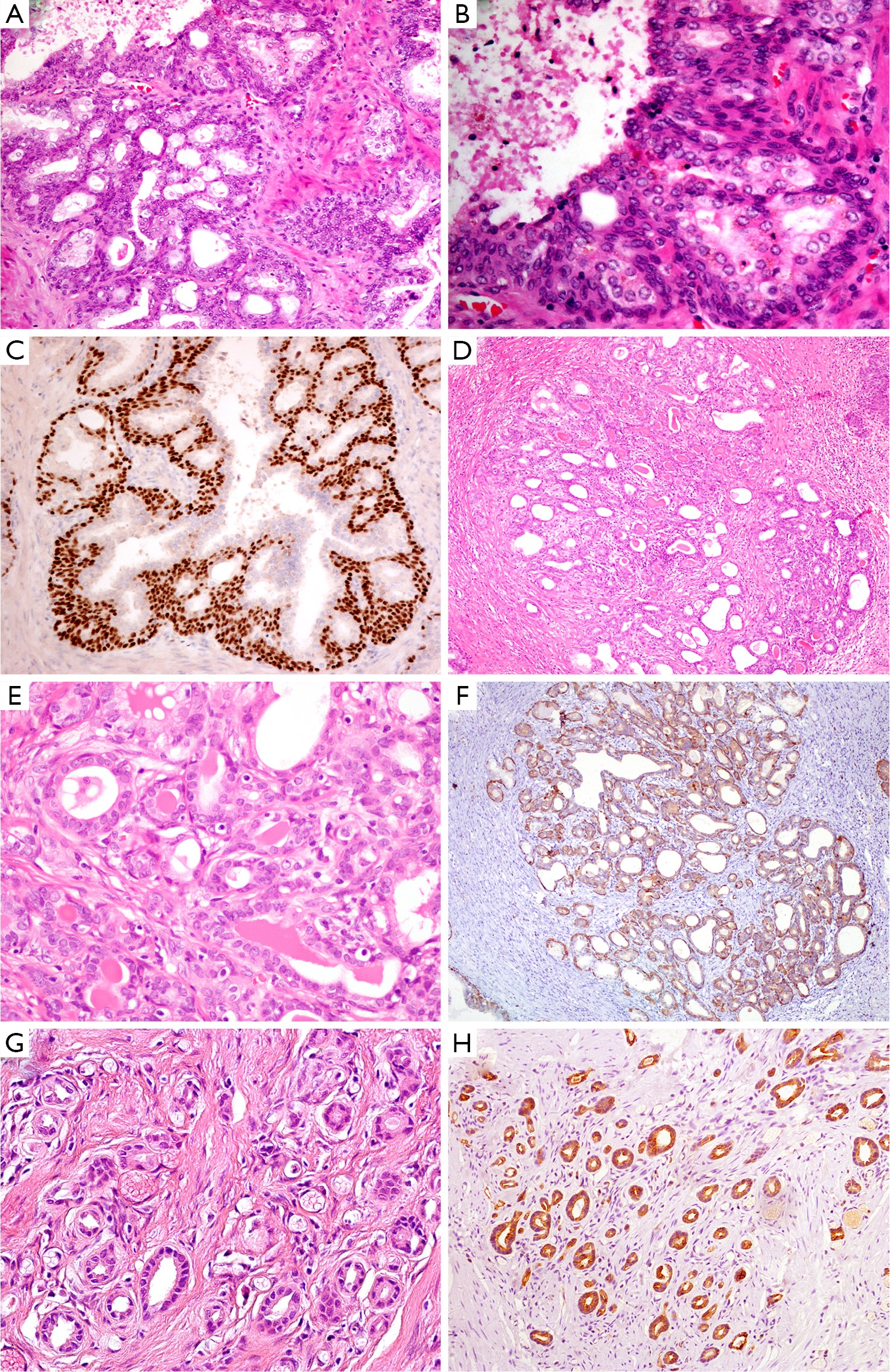
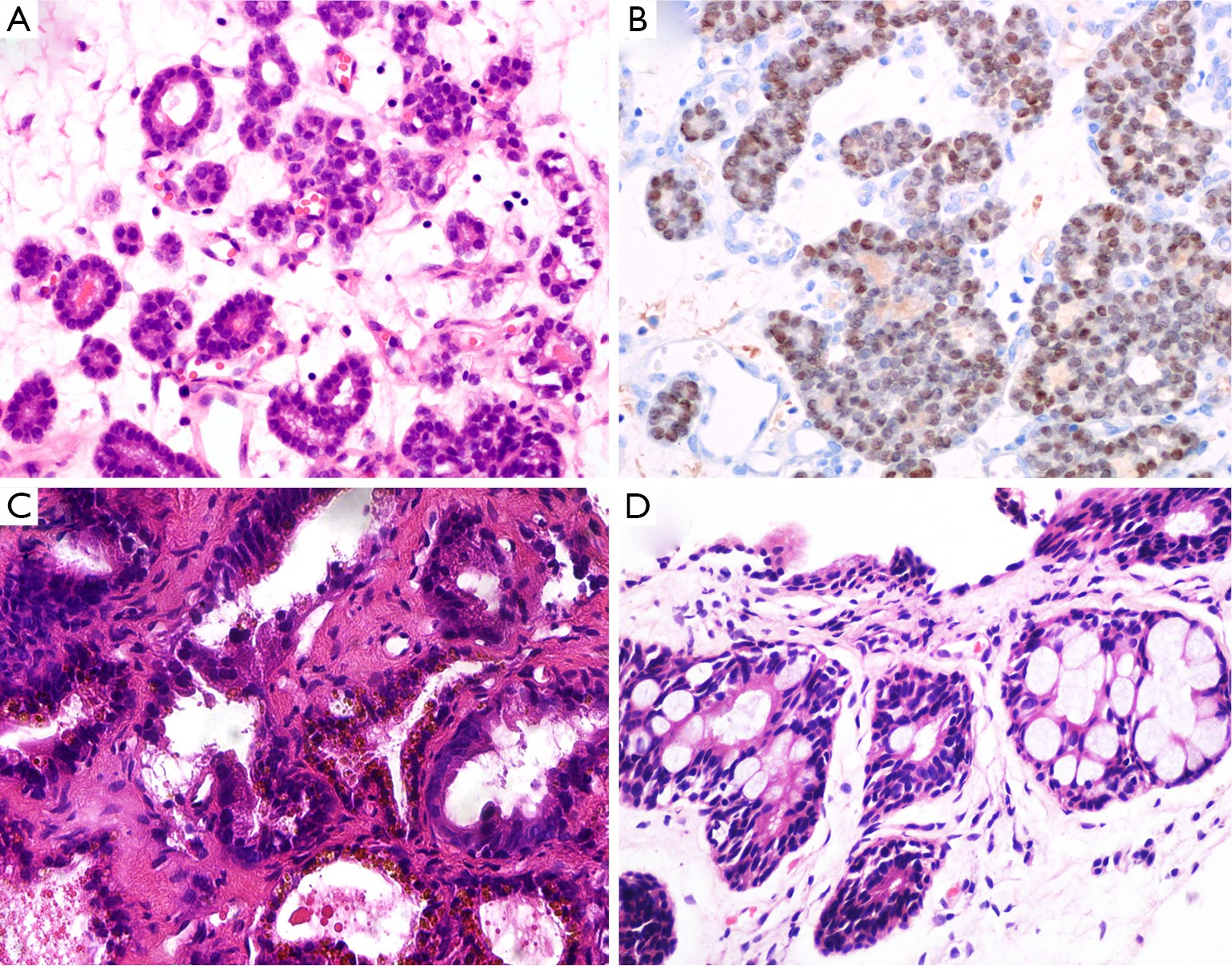
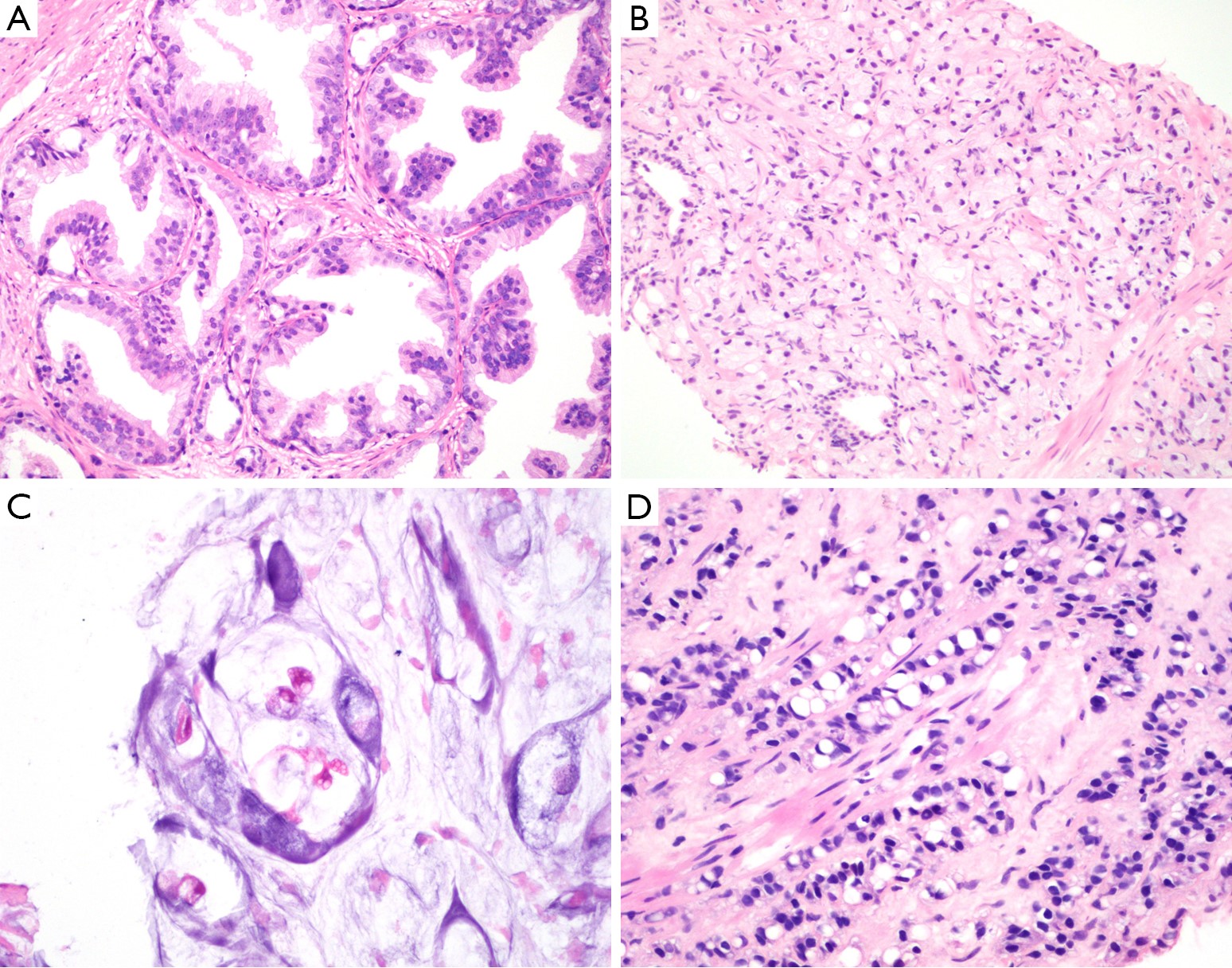
As the most frequent malignant histological subtype in prostatic cancer, prostatic acinar adenocarcinoma (PAA) has a series of benign mimickers including prostatic or non-prostatic lesions and normal structures, which may lead to an erroneous diagnosis and inappropriate treatment. It is very important to be aware of the existence of these mimickers and to recognize their histological features. The differential diagnosis should be based on a comprehensive evaluation of clinical history, histological structure, cytological morphology and the results of immunohistochemistry (IHC) staining, rather than on single criteria (e.g., the presence of prominent nucleoli or basal cell layer).
As the most frequent malignant histological subtype in prostatic cancer, prostatic acinar adenocarcinoma (PAA) has a series of benign mimickers including prostatic or non-prostatic lesions and normal structures, which may lead to an erroneous diagnosis and inappropriate treatment. It is very important to be aware of the existence of these mimickers and to recognize their histological features. The differential diagnosis should be based on a comprehensive evaluation of clinical history, histological structure, cytological morphology and the results of immunohistochemistry (IHC) staining, rather than on single criteria (e.g., the presence of prominent nucleoli or basal cell layer).
2016, 28(1): 92-98.
doi: 10.3978/j.issn.1000-9604.2016.02.05
Abstract:
The knowledge of cellular mechanisms in malignances of the bladder has grown exponentially. Molecular technologies have led to the discovery of the molecular pathways distinguishing low-and high-grade urothelial neoplasms. This trend portends the future in which the classification and diagnosis of the bladder tumors through morphologic analysis will be supported by molecular information correlating with prognosis and targeted therapy. This article outlines tumor molecular pathology of bladder cancer with an emphasis on several promising candidate biomarkers that may soon make their transition to the realm of clinical management of bladder cancer.
The knowledge of cellular mechanisms in malignances of the bladder has grown exponentially. Molecular technologies have led to the discovery of the molecular pathways distinguishing low-and high-grade urothelial neoplasms. This trend portends the future in which the classification and diagnosis of the bladder tumors through morphologic analysis will be supported by molecular information correlating with prognosis and targeted therapy. This article outlines tumor molecular pathology of bladder cancer with an emphasis on several promising candidate biomarkers that may soon make their transition to the realm of clinical management of bladder cancer.

2016, 28(1): 99-106.
doi: 10.3978/j.issn.1000-9604.2016.01.04
Abstract:
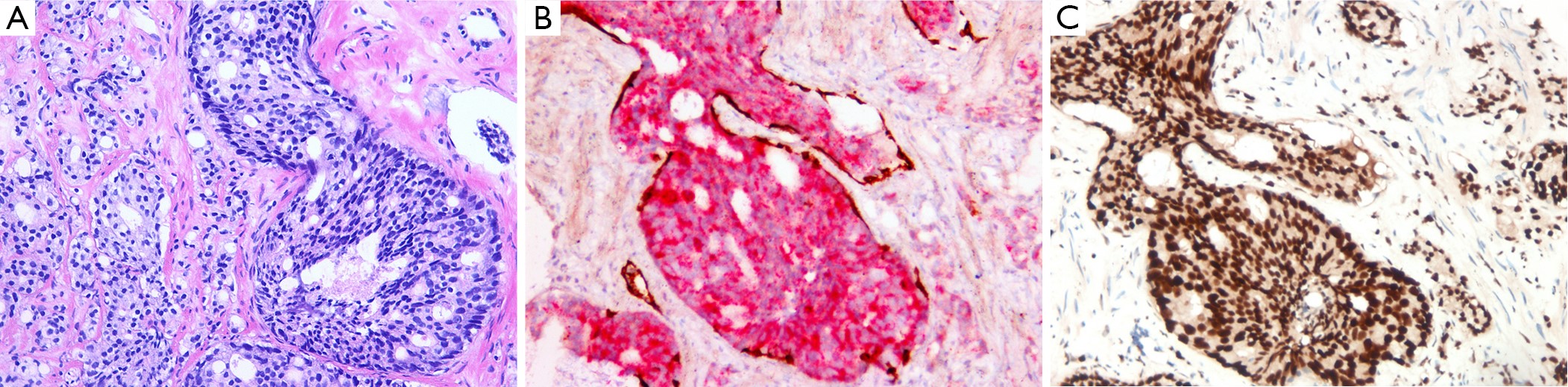
The concept of intraductal carcinoma of prostate (IDC-P) has evolved over the years and its clinicopathologic significance has come to be more clearly appreciated. In contrast to morphologically malignant intraductal lesions that represent earlier stages of the malignant process in other anatomic sites such as the breast, IDC-P has now been generally recognized as a prognostically unfavorable manifestation of later stage spreading of its invasive counterpart. We here briefly review the evolution of the IDC-P concept, the histological diagnostic criteria and differential diagnosis, the clinical significance, as well as recent molecular data of IDC-P.
The concept of intraductal carcinoma of prostate (IDC-P) has evolved over the years and its clinicopathologic significance has come to be more clearly appreciated. In contrast to morphologically malignant intraductal lesions that represent earlier stages of the malignant process in other anatomic sites such as the breast, IDC-P has now been generally recognized as a prognostically unfavorable manifestation of later stage spreading of its invasive counterpart. We here briefly review the evolution of the IDC-P concept, the histological diagnostic criteria and differential diagnosis, the clinical significance, as well as recent molecular data of IDC-P.
2016, 28(1): 107-121.
doi: 10.3978/j.issn.1000-9604.2016.02.01
Abstract:
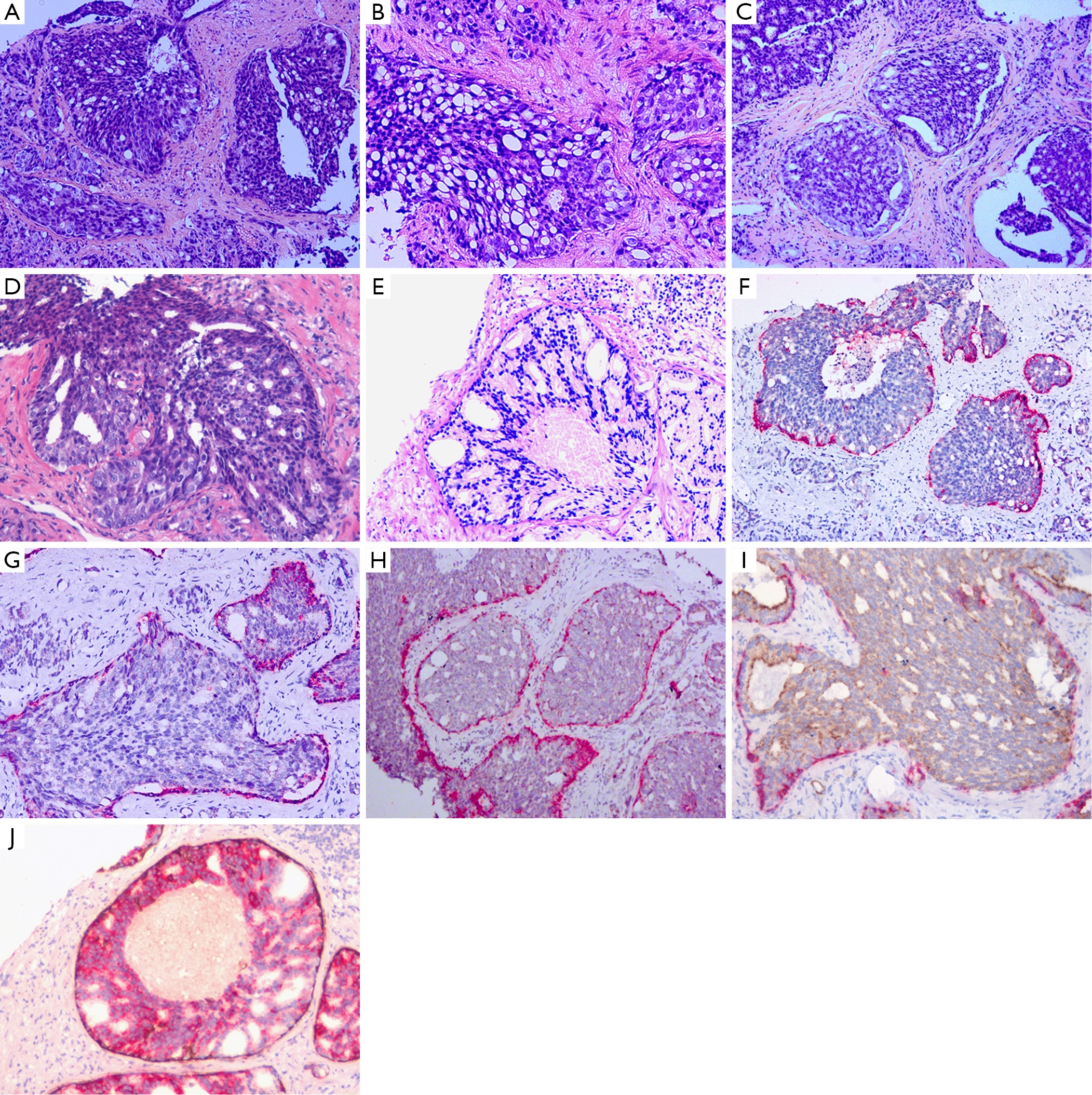
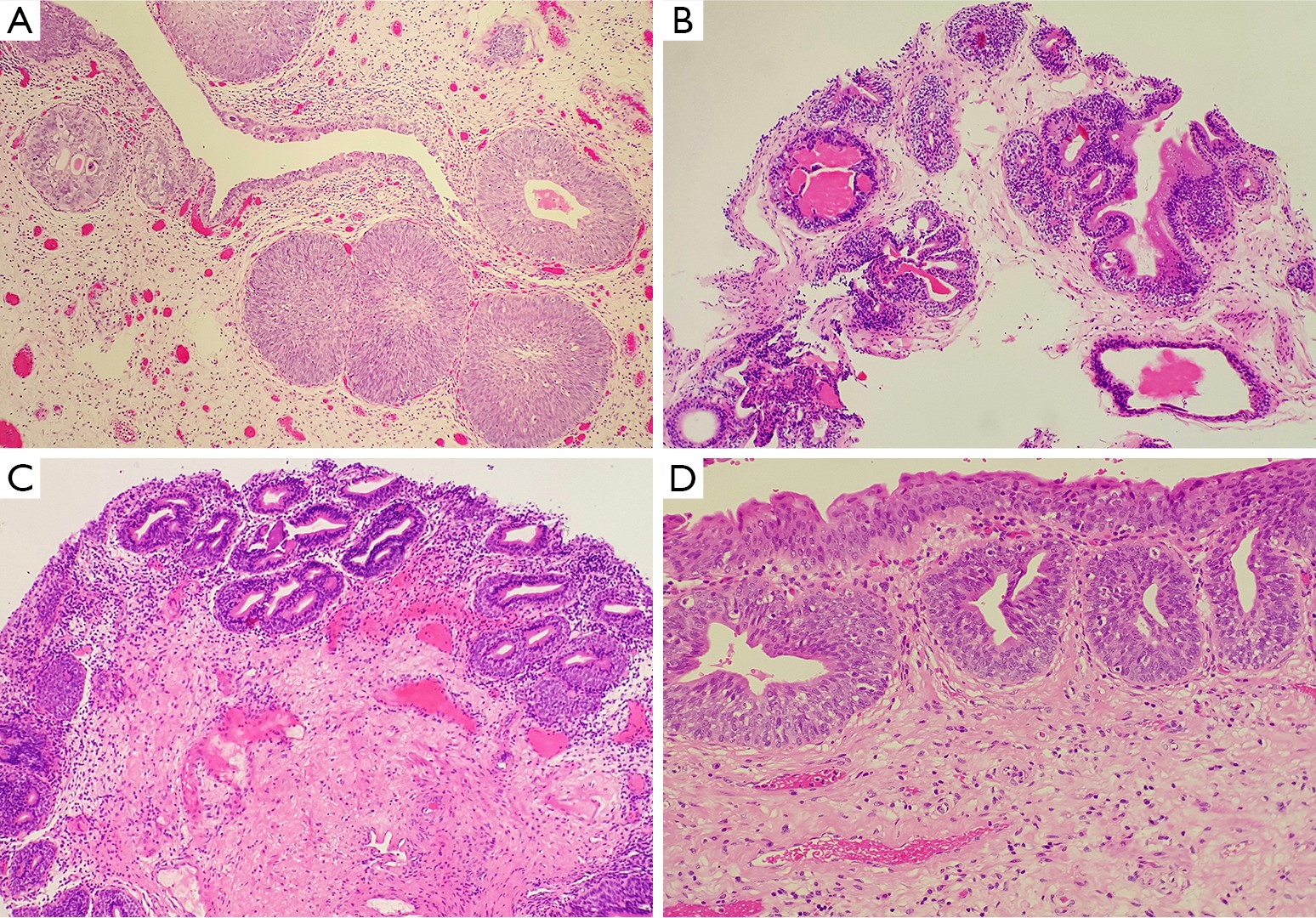
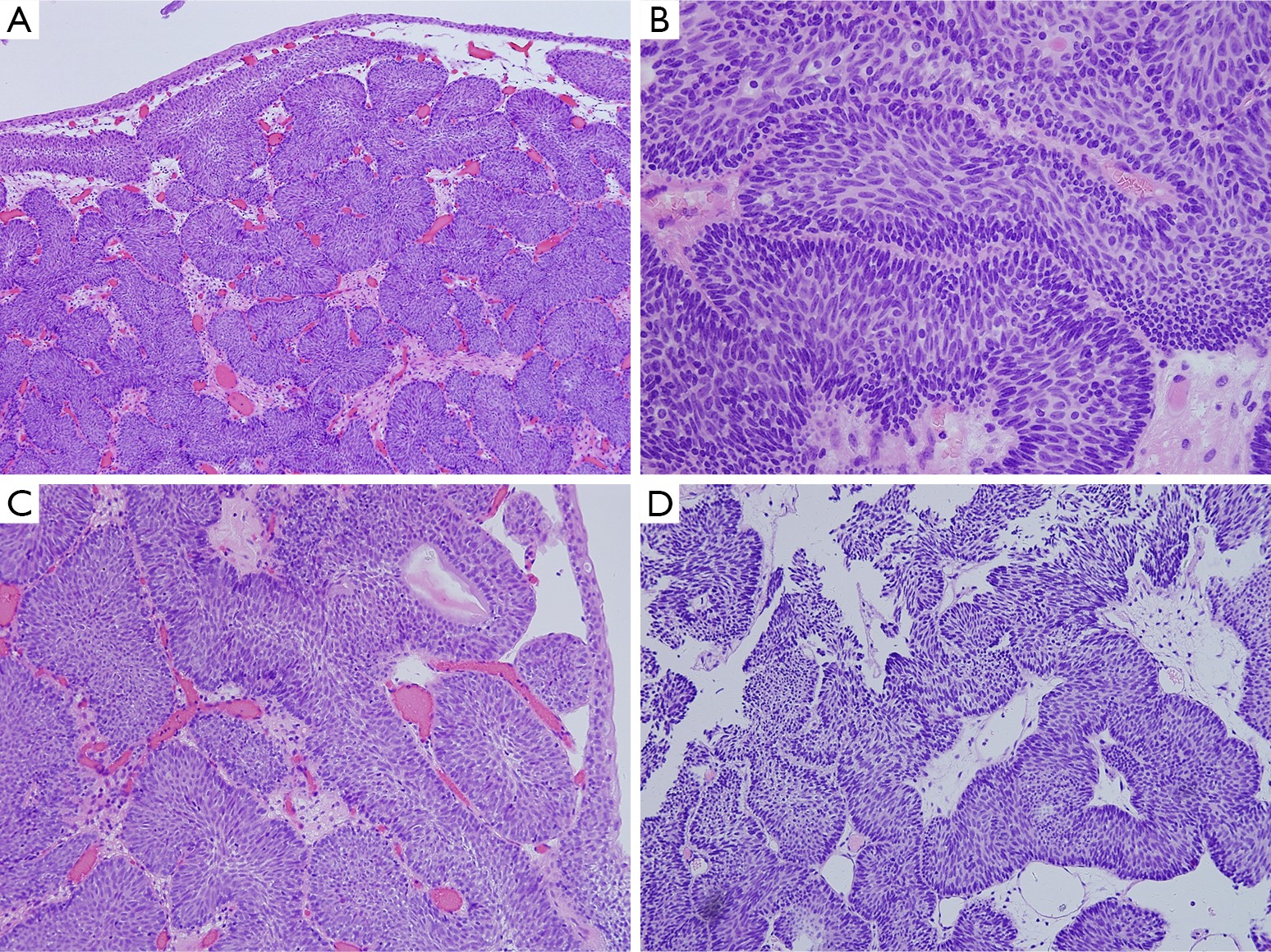
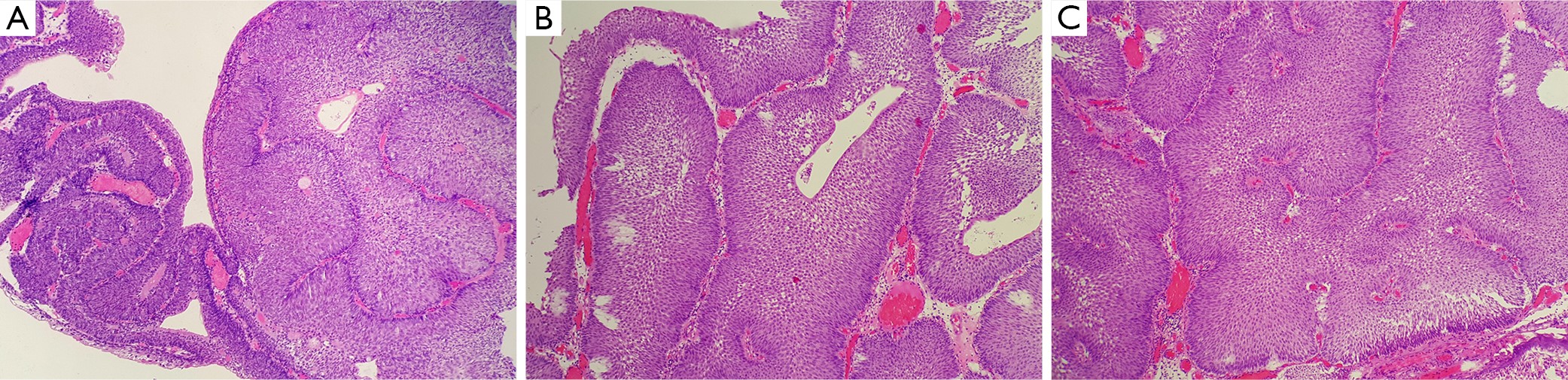
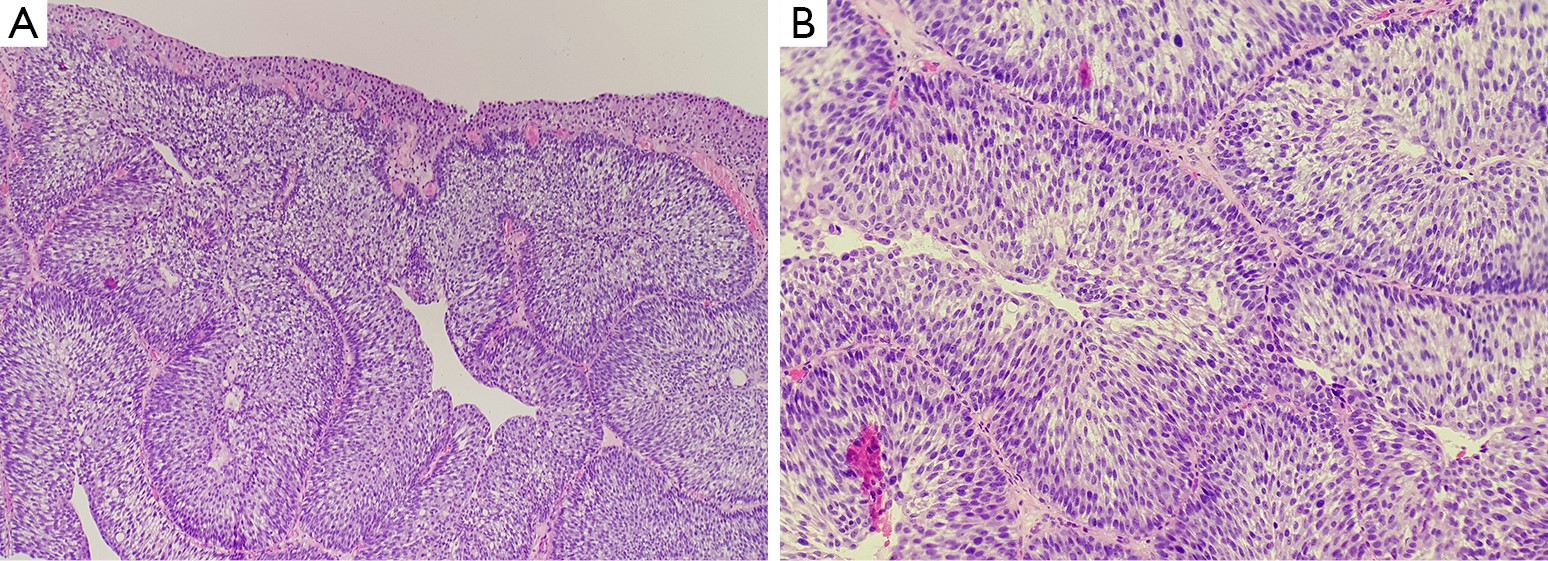
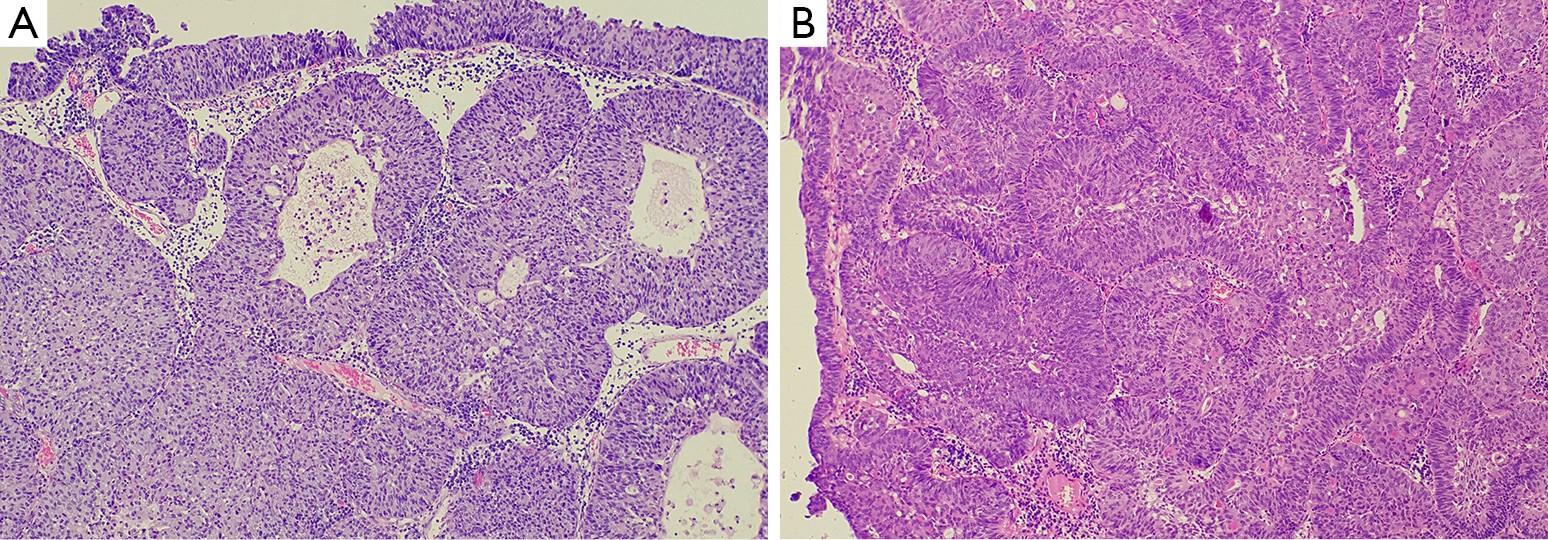
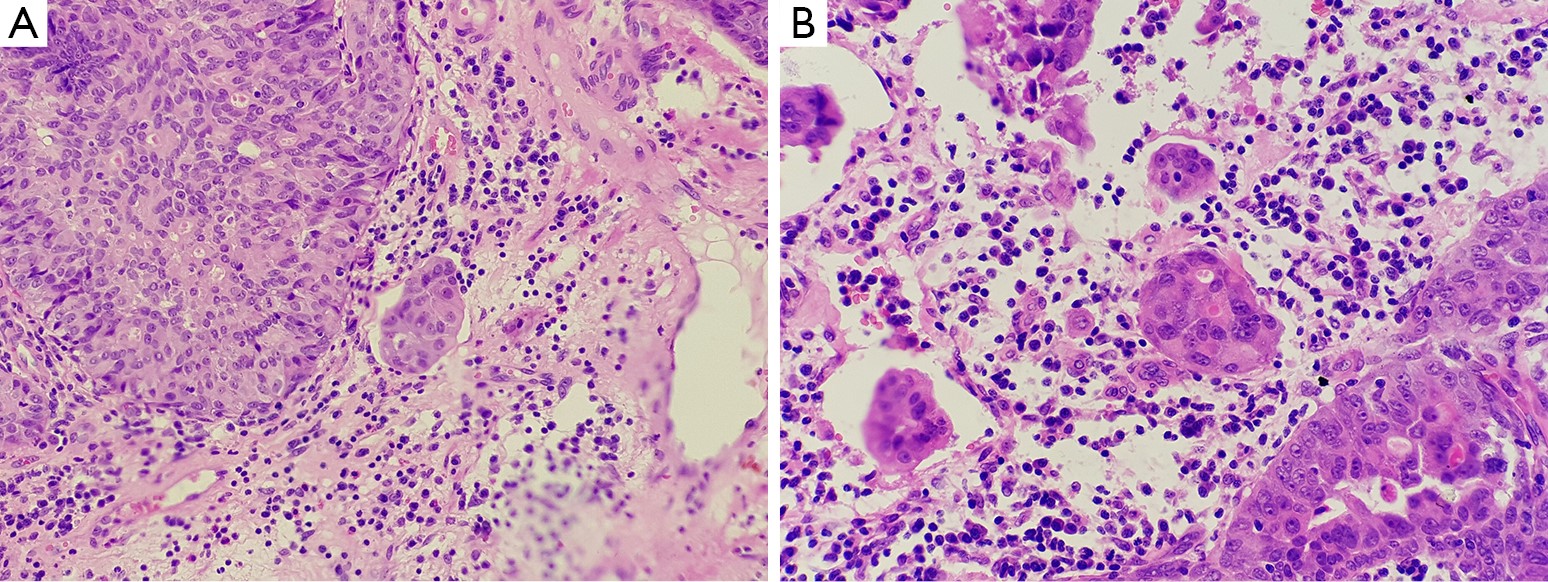
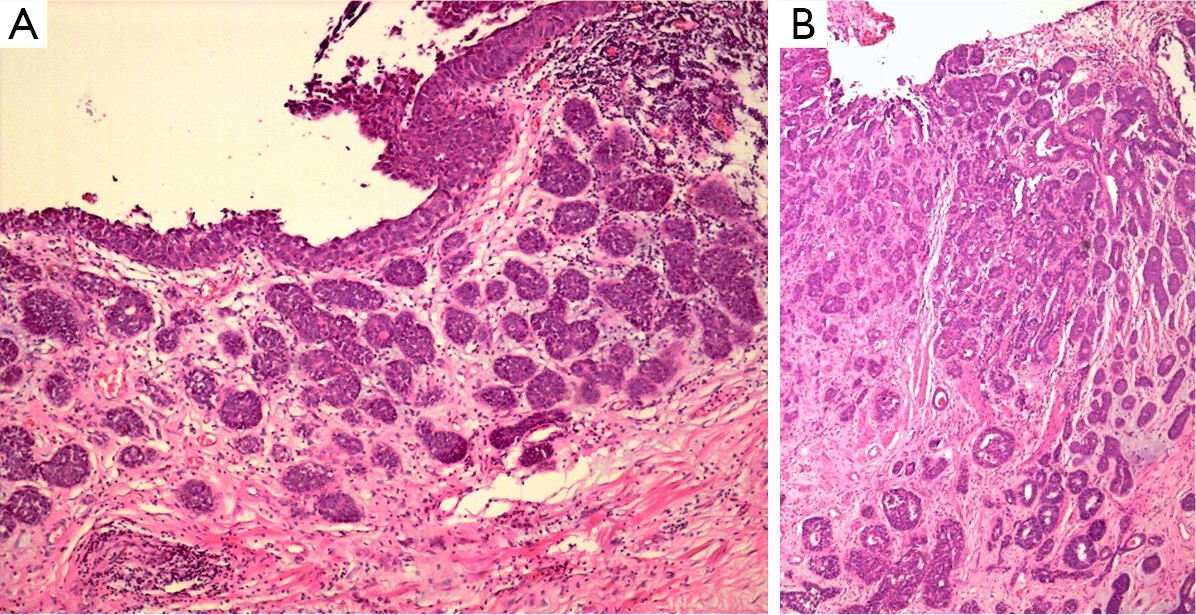
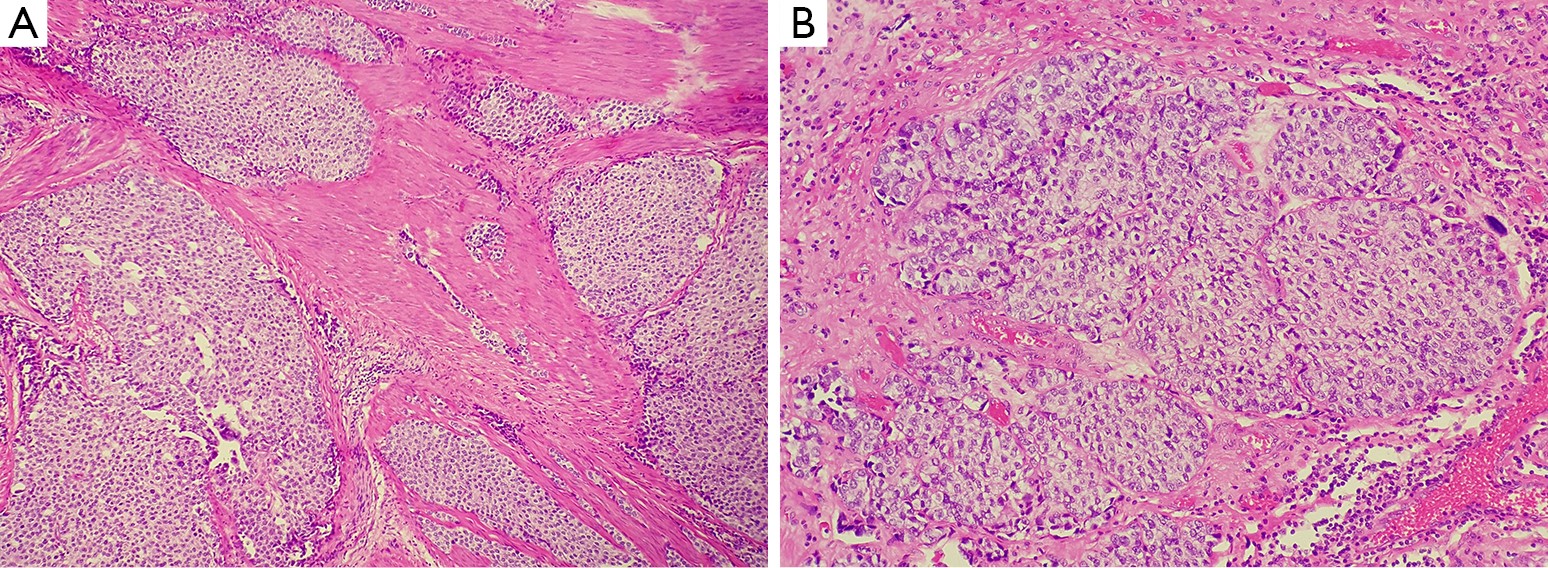
Inverted lesions in the urinary bladder have been the source of some difficulty in urological pathology. The two common ones are von Brunn’s nests and cystitis cystic/cystitis glandularis, which are considered normal variants of urothelium. Apart from them, a number of other rare urothelial lesions with inverted growth pattern occur in the urinary bladder. Some of them are only reactive conditions, just as pseudocarcinomatous hyperplasia. Some are benign tumors, namely inverted papilloma. Whereas others are malignant neoplasms, including inverted papillary urothelial neoplasm of low malignant potential (PUNLMP), non-invasive inverted papillary urothelial carcinoma (low-grade and high-grade), and invasive urothelial carcinoma (inverted, nested and big nested variants). Because of the overlapping morphological features of all the inverted lesions mentioned above, even between high-grade invasive carcinoma and pseudocarcinomatous hyperplasia which are only a kind of reactive conditions, it is very important for the surgical pathologist to recognize and be familiar with these inverted lesions in urinary bladder. In this article, we review these spectrums of inverted lesions of the urinary bladder. Emphasis is placed on histogenesis, morphology, differential diagnosis of these lesions, and the pathologic grading of the non-invasive inverted neoplasms, such as inverted papilloma, inverted PUNLMP, non-invasive inverted papillary urothelial carcinoma with low-grade, and non-invasive inverted papillary urothelial carcinoma with high-grade.
Inverted lesions in the urinary bladder have been the source of some difficulty in urological pathology. The two common ones are von Brunn’s nests and cystitis cystic/cystitis glandularis, which are considered normal variants of urothelium. Apart from them, a number of other rare urothelial lesions with inverted growth pattern occur in the urinary bladder. Some of them are only reactive conditions, just as pseudocarcinomatous hyperplasia. Some are benign tumors, namely inverted papilloma. Whereas others are malignant neoplasms, including inverted papillary urothelial neoplasm of low malignant potential (PUNLMP), non-invasive inverted papillary urothelial carcinoma (low-grade and high-grade), and invasive urothelial carcinoma (inverted, nested and big nested variants). Because of the overlapping morphological features of all the inverted lesions mentioned above, even between high-grade invasive carcinoma and pseudocarcinomatous hyperplasia which are only a kind of reactive conditions, it is very important for the surgical pathologist to recognize and be familiar with these inverted lesions in urinary bladder. In this article, we review these spectrums of inverted lesions of the urinary bladder. Emphasis is placed on histogenesis, morphology, differential diagnosis of these lesions, and the pathologic grading of the non-invasive inverted neoplasms, such as inverted papilloma, inverted PUNLMP, non-invasive inverted papillary urothelial carcinoma with low-grade, and non-invasive inverted papillary urothelial carcinoma with high-grade.
2016, 28(1): 122-129.
doi: 10.3978/j.issn.1000-9604.2016.01.02
Abstract:
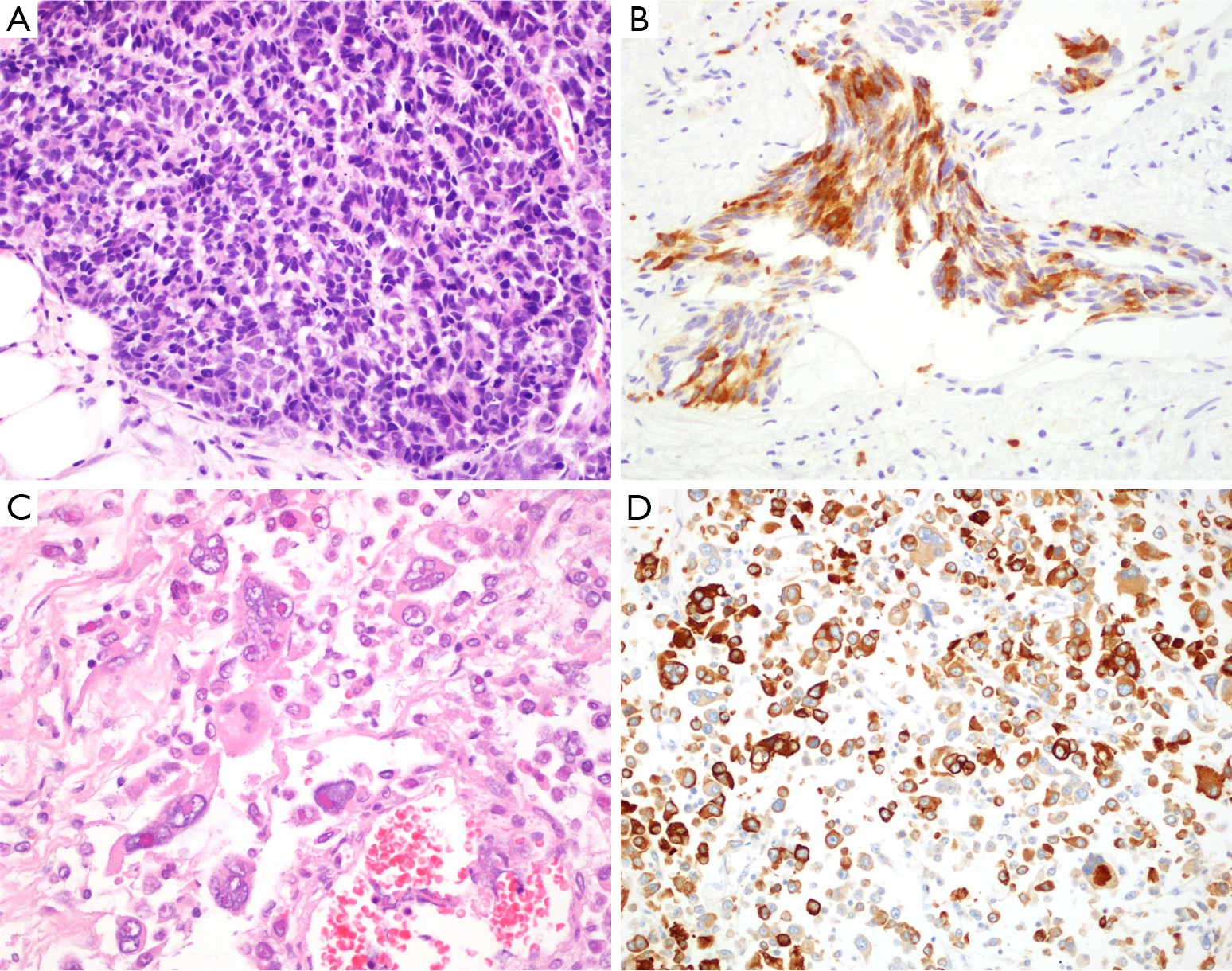
Neuroendocrine differentiation (NED), which is not uncommon in prostate cancer, is increases in prostate cancer after androgen-deprivation therapy (ADT) and generally appears in castration-resistant prostate cancer (CRPC). Neuroendocrine cells, which are found in normal prostate tissue, are a small subset of cells and have unique function in regulating the growth of prostate cells. Prostate cancer with NED includes different types of tumor, including focal NED, pure neuroendocrine tumor or mixed neuroendocrine-adenocarcinoma. Although more and more studies are carried out on NED in prostate cancer, the molecular components that are involved in NED are still poorly elucidated. We review neuroendocrine cells in normal prostate tissue, NED in prostate cancer, terminology of NED and biomarkers used for detecting NED in routine pathological practice. Some recently reported molecular components which drive NED in prostate cancer are listed in the review.
Neuroendocrine differentiation (NED), which is not uncommon in prostate cancer, is increases in prostate cancer after androgen-deprivation therapy (ADT) and generally appears in castration-resistant prostate cancer (CRPC). Neuroendocrine cells, which are found in normal prostate tissue, are a small subset of cells and have unique function in regulating the growth of prostate cells. Prostate cancer with NED includes different types of tumor, including focal NED, pure neuroendocrine tumor or mixed neuroendocrine-adenocarcinoma. Although more and more studies are carried out on NED in prostate cancer, the molecular components that are involved in NED are still poorly elucidated. We review neuroendocrine cells in normal prostate tissue, NED in prostate cancer, terminology of NED and biomarkers used for detecting NED in routine pathological practice. Some recently reported molecular components which drive NED in prostate cancer are listed in the review.
2016, 28(1): 130-143.
doi: 10.3978/j.issn.1000-9604.2016.01.06
Abstract:
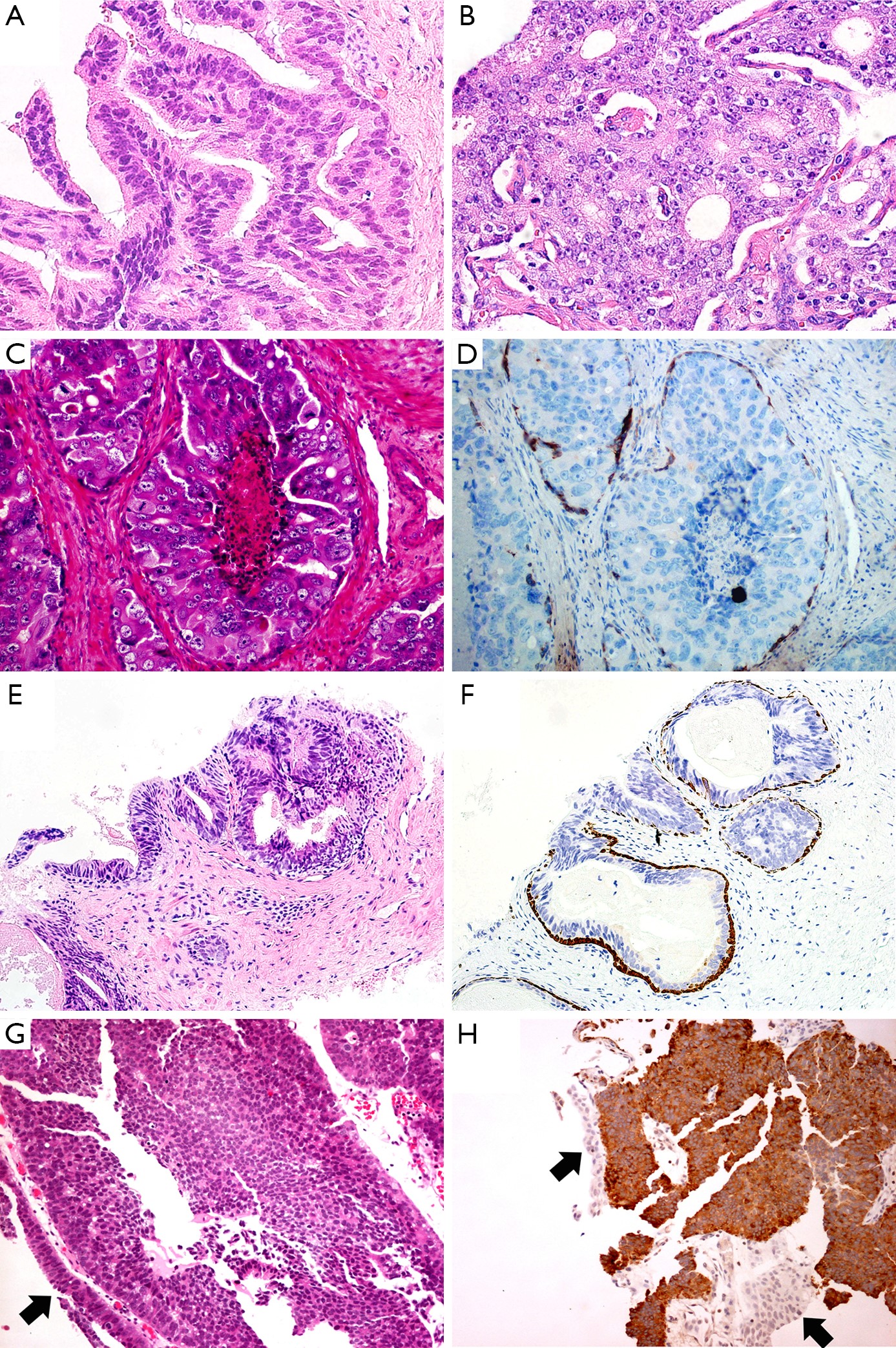
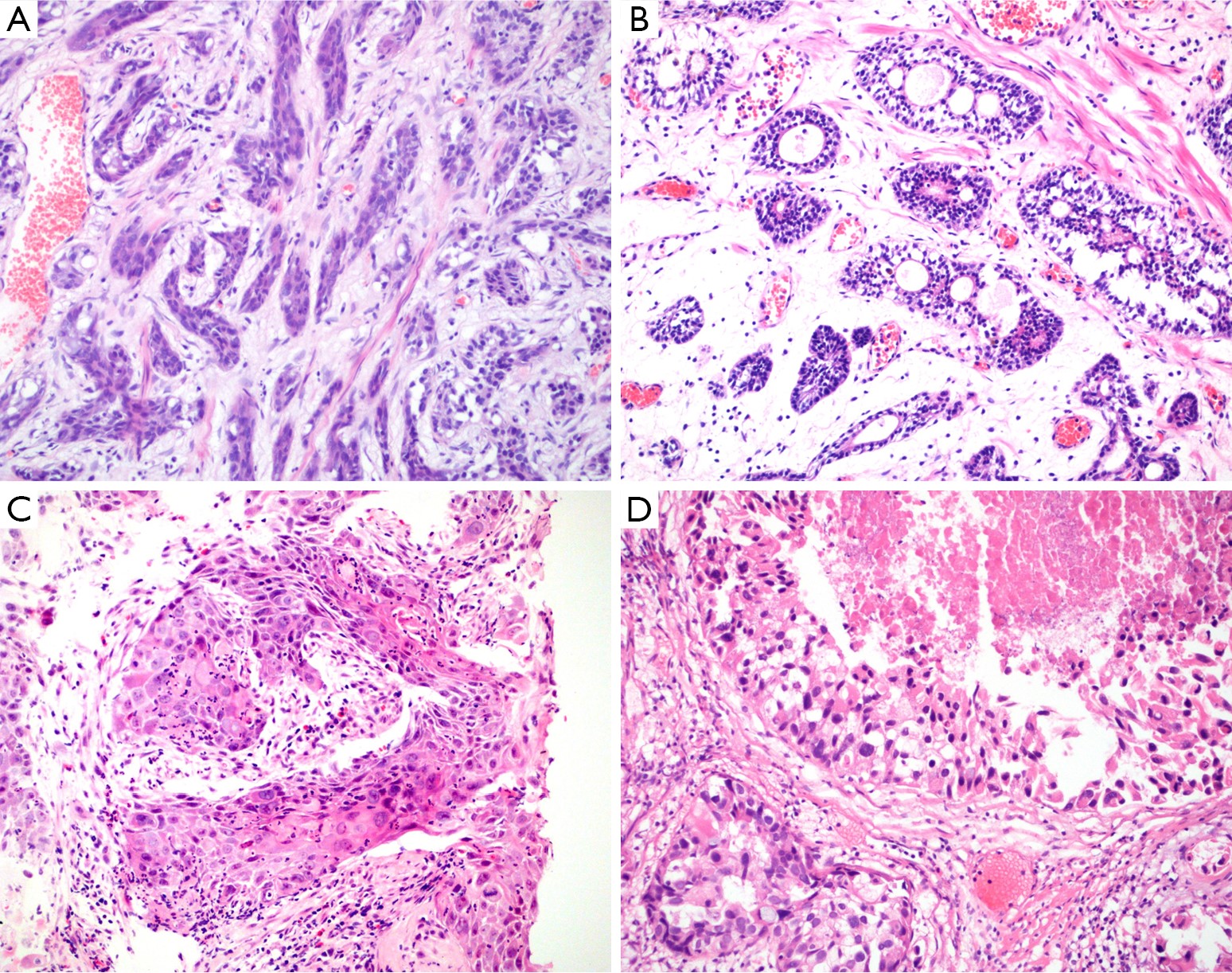
There are some current literatures describing the morphologic change of prostate carcinoma variants. Some subtypes do not respond to hormone deprivation therapy, for example adenosquamous and squamous cell carcinoma (SQCC), basaloid and adenoid cystic carcinoma (ACC), small cell carcinoma (SmCC), sarcomatoid carcinoma, urothelial carcinoma; some are defined in special Gleason grade, some develop different prognosis. So, it is very important to identify these rare subtypes to avoid misdiagnosis. In this review, we aim to describe the typical clinicopathological features of the rare variants of prostate cancer, including prostate acinar adenocarcinoma morphologic variants.
There are some current literatures describing the morphologic change of prostate carcinoma variants. Some subtypes do not respond to hormone deprivation therapy, for example adenosquamous and squamous cell carcinoma (SQCC), basaloid and adenoid cystic carcinoma (ACC), small cell carcinoma (SmCC), sarcomatoid carcinoma, urothelial carcinoma; some are defined in special Gleason grade, some develop different prognosis. So, it is very important to identify these rare subtypes to avoid misdiagnosis. In this review, we aim to describe the typical clinicopathological features of the rare variants of prostate cancer, including prostate acinar adenocarcinoma morphologic variants.
2016, 28(1): 144-145.
doi: 10.3978/j.issn.1000-9604.2016.02.10
Abstract:




