
2016 Vol.28(2)
Display Mode: |
2016, 28(2): 146-149.
doi: 10.21147/j.issn.1000-9604.2016.02.01
 Abstract
Abstract FullText HTML
FullText HTML PDF 130KB
PDF 130KB
Abstract:
After the results obtained in the two randomized clinical trial, the ELIOT trial and the TARGIT-A trial, a heated debate is going on concerning the question of applying intraoperative radiotherapy (IORT) instead of postoperative whole breast irradiation (WBI) after breast conservative treatment. Currently, many centers are applying the IORT following the strict selection criteria dictated by the working groups American Society for Radiation Oncology (ASTRO) and Groupe Européen de Curiethérapie-European Society for Therapeutic Radiology and Oncology (GEC-ESTRO) and monitoring the oncological outcome together with radiation toxicity on breast tissue. The clinical experience of the Geneva University Hospital regarding the use of the Intrabeam system is evaluated and compared with current evidences.
After the results obtained in the two randomized clinical trial, the ELIOT trial and the TARGIT-A trial, a heated debate is going on concerning the question of applying intraoperative radiotherapy (IORT) instead of postoperative whole breast irradiation (WBI) after breast conservative treatment. Currently, many centers are applying the IORT following the strict selection criteria dictated by the working groups American Society for Radiation Oncology (ASTRO) and Groupe Européen de Curiethérapie-European Society for Therapeutic Radiology and Oncology (GEC-ESTRO) and monitoring the oncological outcome together with radiation toxicity on breast tissue. The clinical experience of the Geneva University Hospital regarding the use of the Intrabeam system is evaluated and compared with current evidences.
2016, 28(2): 150-160.
doi: 10.21147/j.issn.1000-9604.2016.02.02
Abstract:
Hepatocellular carcinoma (HCC) is a malignant disease with limited therapeutic options due to its aggressive progression. It places heavy burden on most low and middle income countries to treat HCC patients. Nowadays accurate HCC risk predictions can help making decisions on the need for HCC surveillance and antiviral therapy. HCC risk prediction models based on major risk factors of HCC are useful and helpful in providing adequate surveillance strategies to individuals who have different risk levels. Several risk prediction models among cohorts of different populations for estimating HCC incidence have been presented recently by using simple, efficient, and ready-to-use parameters. Moreover, using predictive scoring systems to assess HCC development can provide suggestions to improve clinical and public health approaches, making them more cost-effective and effort-effective, for inducing personalized surveillance programs according to risk stratification. In this review, the features of risk prediction models of HCC across different populations were summarized, and the perspectives of HCC risk prediction models were discussed as well.
Hepatocellular carcinoma (HCC) is a malignant disease with limited therapeutic options due to its aggressive progression. It places heavy burden on most low and middle income countries to treat HCC patients. Nowadays accurate HCC risk predictions can help making decisions on the need for HCC surveillance and antiviral therapy. HCC risk prediction models based on major risk factors of HCC are useful and helpful in providing adequate surveillance strategies to individuals who have different risk levels. Several risk prediction models among cohorts of different populations for estimating HCC incidence have been presented recently by using simple, efficient, and ready-to-use parameters. Moreover, using predictive scoring systems to assess HCC development can provide suggestions to improve clinical and public health approaches, making them more cost-effective and effort-effective, for inducing personalized surveillance programs according to risk stratification. In this review, the features of risk prediction models of HCC across different populations were summarized, and the perspectives of HCC risk prediction models were discussed as well.
2016, 28(2): 161-167.
doi: 10.21147/j.issn.1000-9604.2016.02.03
Abstract:
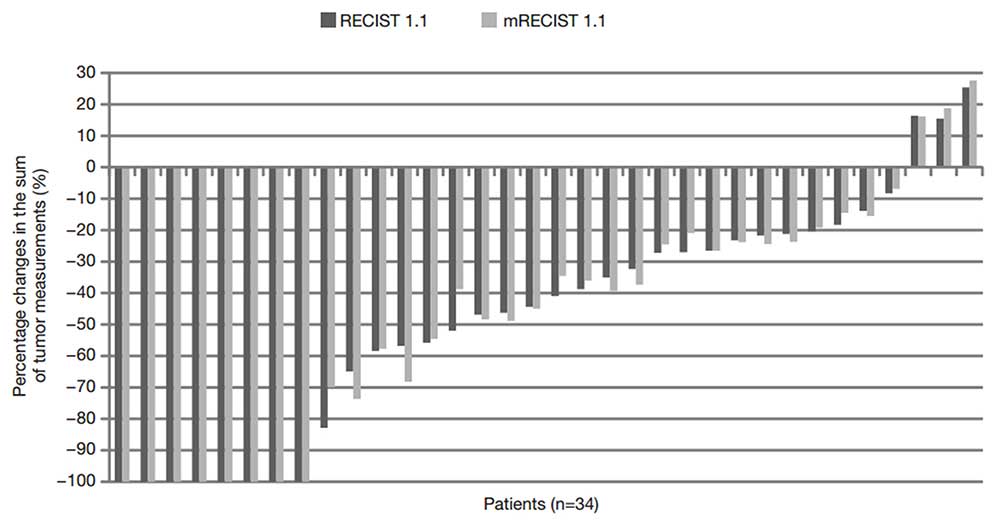
Background: The criterion of two target lesions per organ in the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 is an arbitrary one, being supported by no objective evidence. The optimal number of target lesions per organ still needs to be investigated. We compared tumor responses using the RECIST 1.1 (measuring two target lesions per organ) and modified RECIST 1.1 (measuring the single largest lesion in each organ) in patients with small cell lung cancer (SCLC). Methods: We reviewed medical records of patients with SCLC who received first-line treatment between January 2004 and December 2014 and compared tumor responses according to the two criteria using computed tomography. Results: There were a total of 34 patients who had at least two target lesions in any organ according to the RECIST 1.1 during the study period. The differences in the percentage changes of the sum of tumor measurements between RECIST 1.1 and modified RECIST 1.1 were all within 13%. Seven patients showed complete response and fourteen showed partial response according to the RECIST 1.1. The overall response rate was 61.8%. When assessing with the modified RECIST 1.1 instead of the RECIST 1.1, tumor responses showed perfect concordance between the two criteria (k=1.0). Conclusions: The modified RECIST 1.1 showed perfect agreement with the original RECIST 1.1 in the assessment of tumor response of SCLC. Our result suggests that it may be enough to measure the single largest target lesion per organ for evaluating tumor response.
2016, 28(2): 168-179.
doi: 10.21147/j.issn.1000-9604.2016.02.04
Abstract:
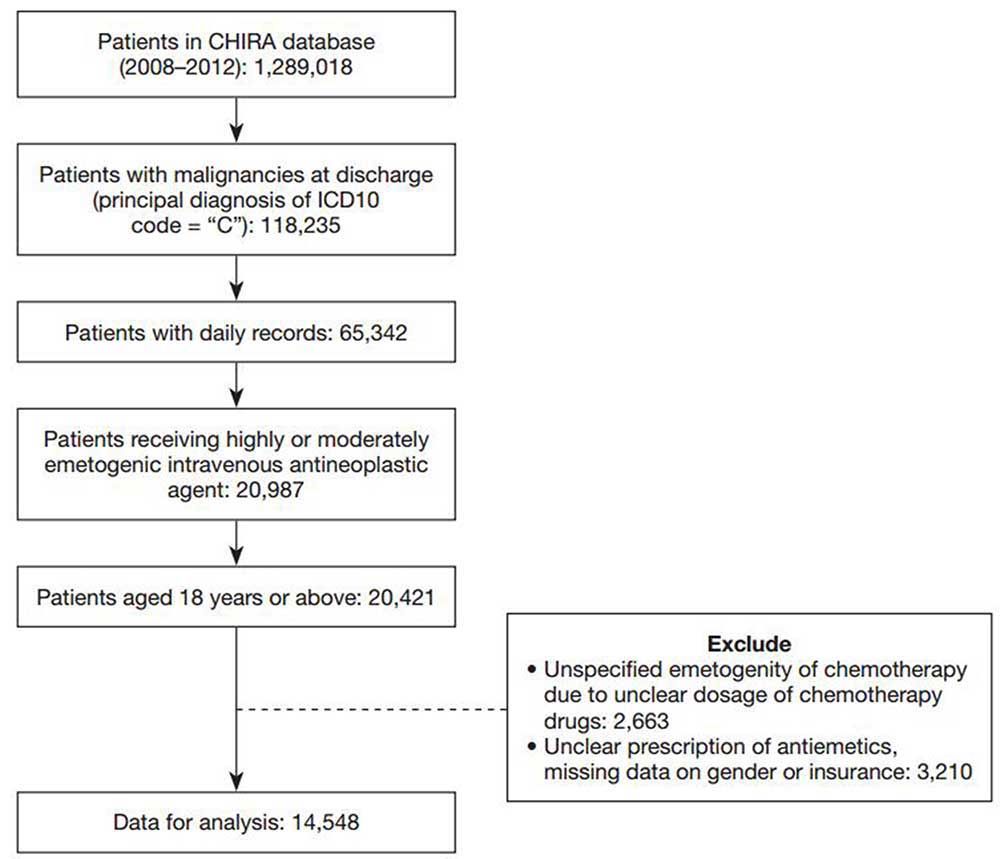
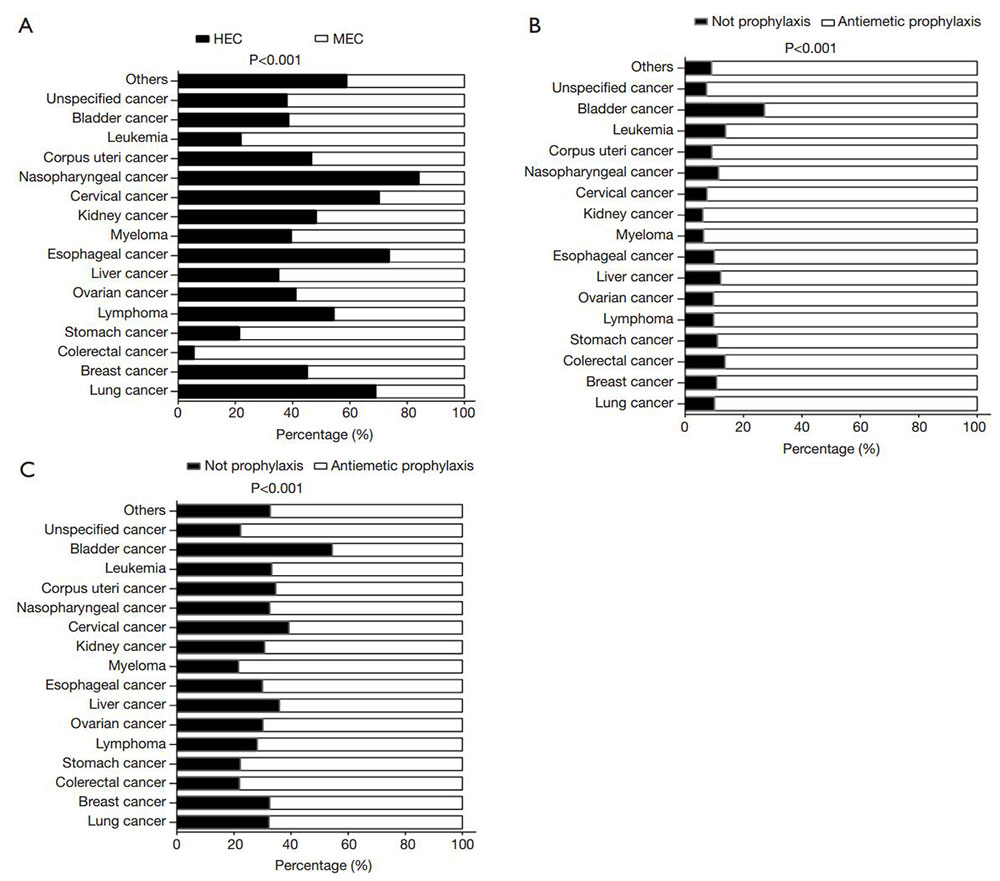
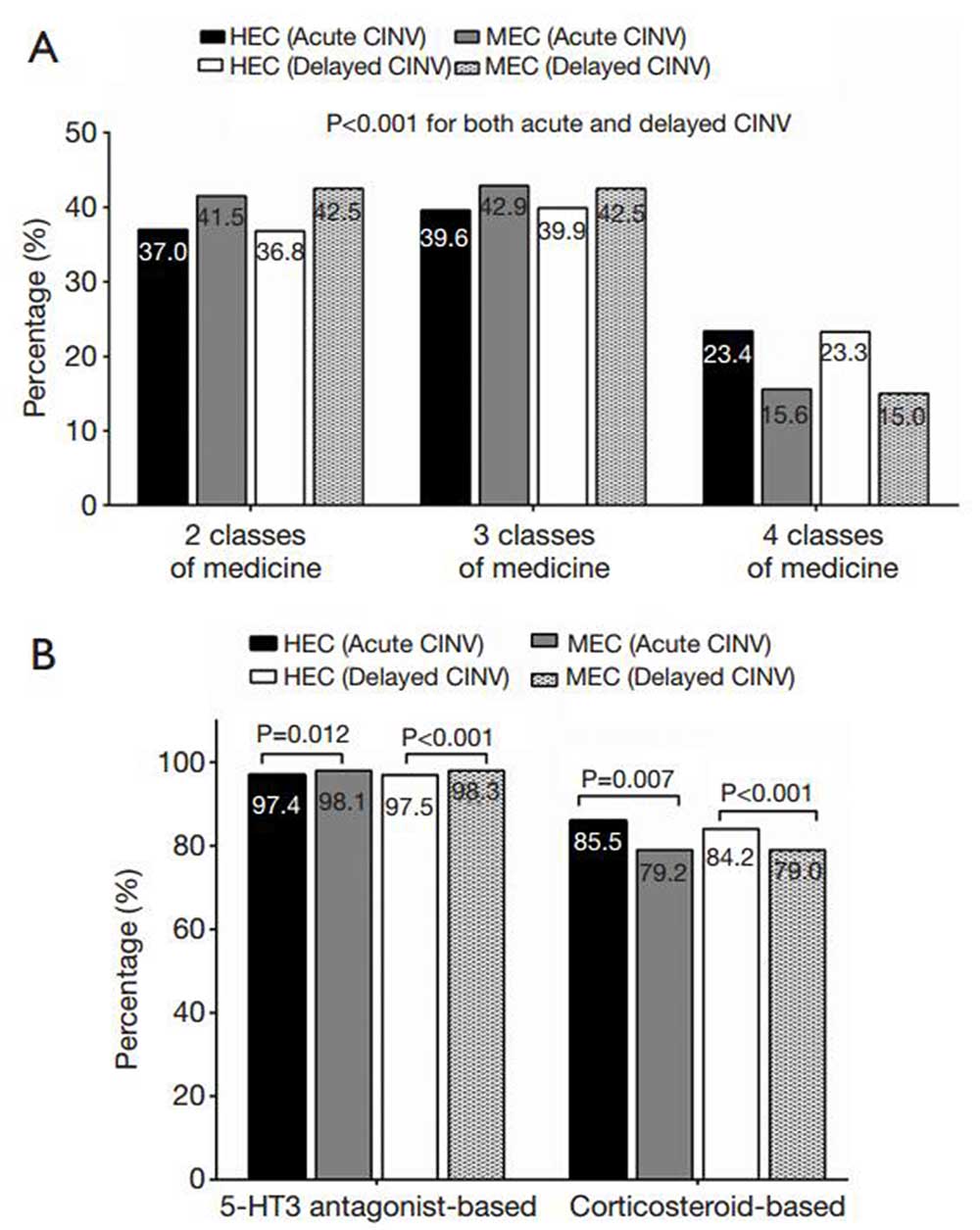
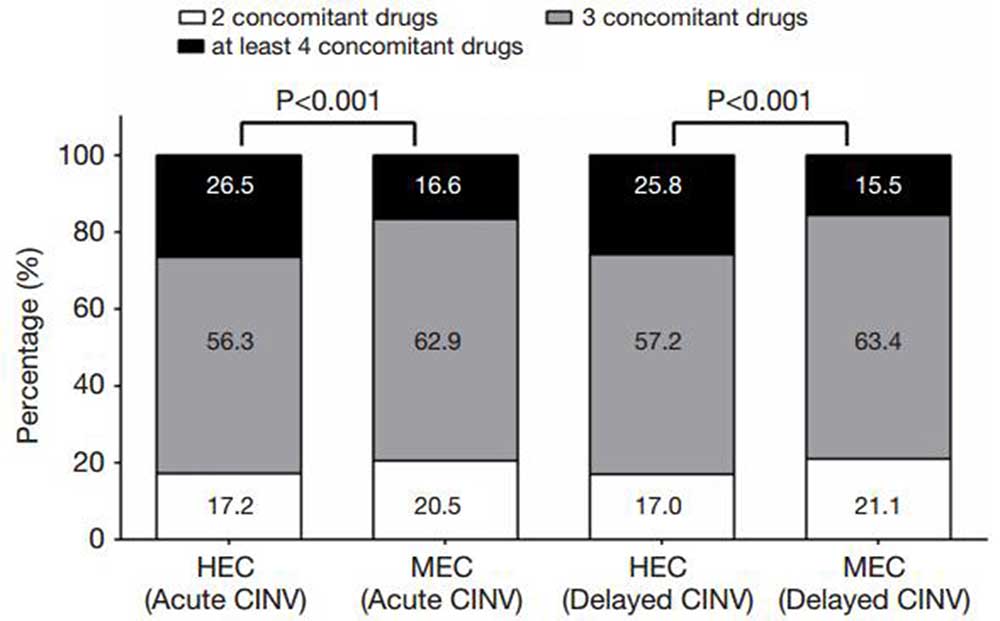
BackgroundFew studies have attempted to evaluate the use of antiemetic therapy for chemotherapy-induced nausea and vomiting (CINV) at a national level in China or to assess how treatment regimens adhere to current guidelines. MethodsWe searched the China Health Insurance Research Association (CHIRA) Database to identify patients with cancer who were ≥18 years old and received either moderately or highly emetogenic chemotherapy (MEC and HEC, respectively) between 2008 and 2012. Patients’ characteristics as well as usage of specific antiemetic regimens were analyzed using descriptive statistics. ResultsOf the 14,548 patients included in the study, 6,477 received HEC while 8,071 were treated with MEC. Approximately 89.9% used antiemetics prophylactically to prevent acute CINV and 71.5% for delayed CINV while 9.0% were prescribed antiemetics as rescue therapy. A significantly lower proportion of patients treated with HEC received prophylactic antiemetic therapy for delayed CINV as compared to those treated with MEC (59.4% vs. 81.3%; P<0.001). The HEC group had a slightly lower proportion of patients using a mixed regimen containing a 5-HT3 antagonist to prevent both acute and delayed CINV than the MEC group (P≤0.012); however, a higher proportion received a mixed regimen containing corticosteroids (P≤0.007). Although more than half of the patients in the HEC group took three antiemetics to prevent acute and delayed CINV, these rates were significantly lower than those of the MEC group (both P<0.001). Finally, analysis of the regimens used revealed that there is over-utilization of drugs within the same class of antiemetic. ConclusionsThese findings indicate that more attention is needed for treatment of delayed CINV, in terms of both overall use and the components of a typical treatment regimen.

2016, 28(2): 180-186.
doi: 10.21147/j.issn.1000-9604.2016.02.05
Abstract:
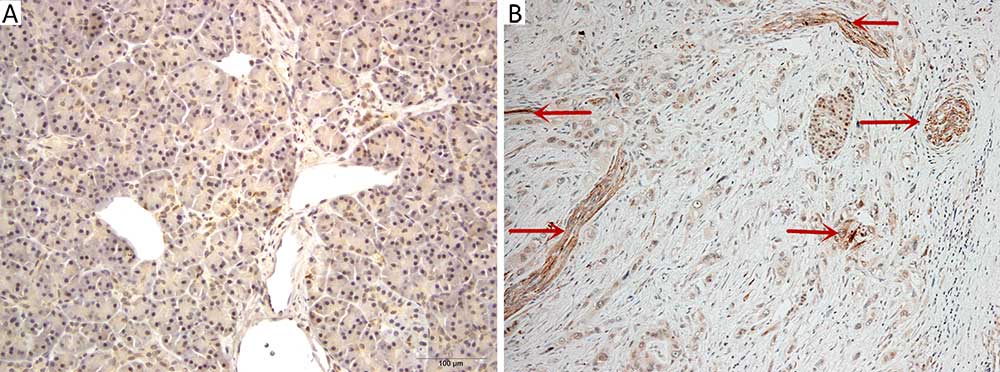
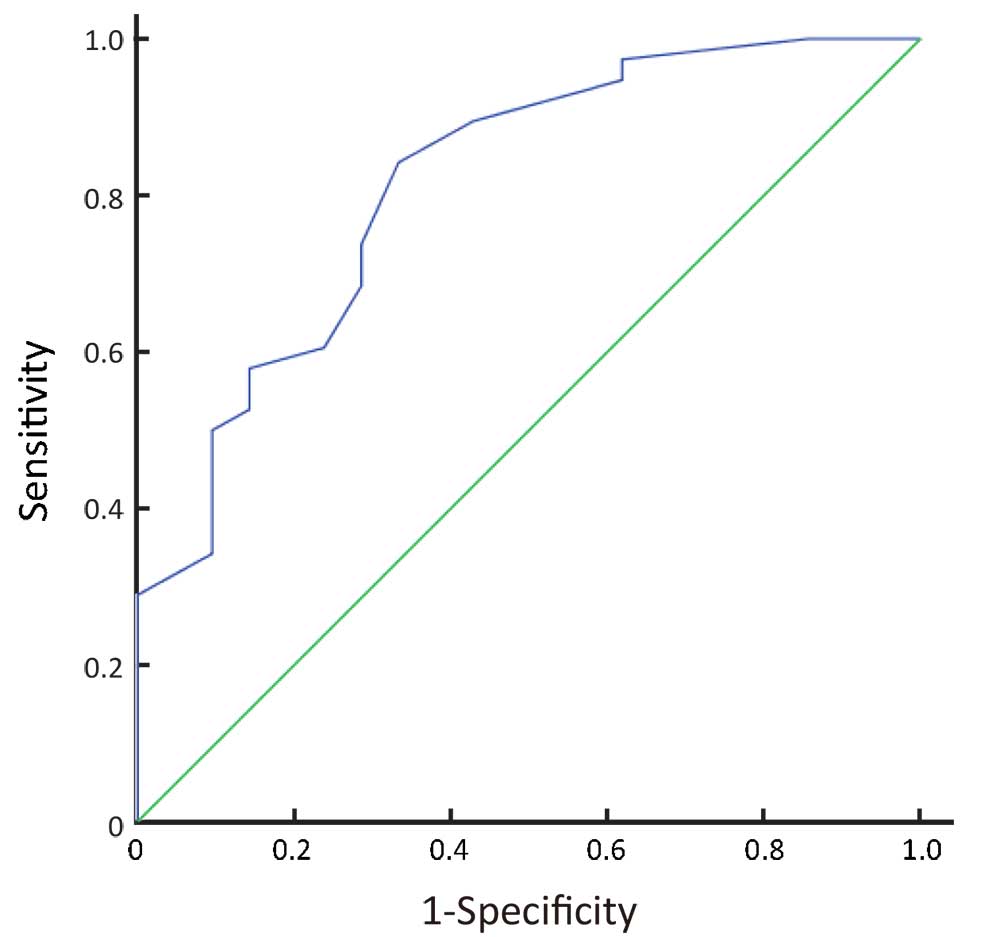
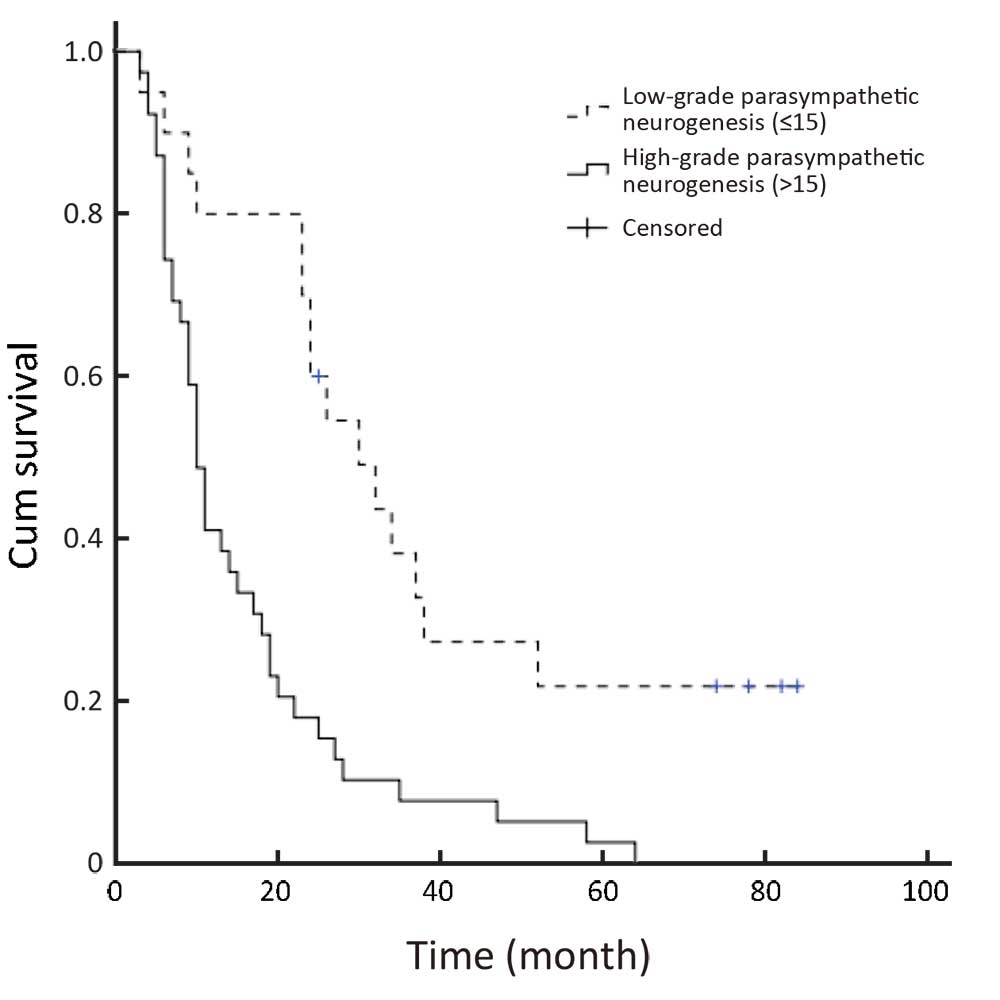
Objective: To investigate the frequency of parasympathetic neurogenesis and determine its association with tumor budding and prognosis in pancreatic ductal adenocarcinoma (PDAC). Methods: Parasympathetic neurogenesis was defined as the distribution of abnormal parasympathetic nerves in the stroma tissue. Staining of vesicular acetylcholine transporter (VAChT), as a marker for parasympathetic neurogenesis, was performed on a representative specimen of the tumor for 59 PDAC patients with available clinical, pathologic, and follow-up information. Three specimens containing normal pancreatic tissues were stained in parallel. The number of parasympathetic nerve fibers was counted in five high-power microscopic fields (5×0.785 mm2). Cut-off values were calculated by receiver operating characteristic curve analysis. Results: VAChT-positive parasympathetic nerve fibers were not seen in the stroma of 3 cases of normal pancreatic tissues. In 59 PDAC cases, the range of parasympathetic neurogenesis was 4-38 fibers/(5×0.785) mm2, with a median of 18 fibers/(5×0.785) mm2. Patients with parasympathetic neurogenesis >15 fibers/(5×0.785) mm2 were defined as the high-density group (39 patients, 66.1%), and those with parasympathetic neurogenesis 15 fibers/(5×0.785) mm2 as the low-density group (20 patients, 33.9%). The high-density group had a higher occurrence of tumor budding (P=0.001) and a higher rate of early recurrence (P=0.035). Parasympathetic neurogenesis appeared to be an independent adverse prognostic factor [hazard ratio (HR)=2.45, 95% confidence interval (95% CI): 1.25-4.81, P=0.009], in addition to American Joint Committee on Cancer (AJCC) stage (P=0.010) and tumor budding (P=0.009). Conclusions: Parasympathetic neurogenesis is strongly associated with tumor budding and correlates with an adverse prognosis in PDAC.
2016, 28(2): 187-196.
doi: 10.21147/j.issn.1000-9604.2016.02.06
Abstract:
Background: To evaluate the short-term and long-term outcomes after laparoscopic hysterectomy (LH) compared with abdominal hysterectomy (AH) in case of benign gynecological disease. Methods: A multi-center cohort retrospective comparative study of population among 4,895 hysterectomies (3,539 LH vs.1,356 AH) between 2007 and 2013 was involved. Operative time (OT), estimated blood loss (EBL), intra-operative and post-operative complications, passing flatus; days with indwelling catheter, questionnaires covering pelvic floor functions and sexual functions were assessed. Results: The EBL (174.1±157.4 vs. 263.1±183.2 cc, LH and AH groups, respectively), passing flatus (38.7±14.1 vs. 48.1±13.2 hours), days with indwelling catheter (1.5±0.6 vs. 2.2±0.8 days), use of analgesics (6.5% vs. 73.1%), intra-operative complication rate (2.4% vs. 4.1%), post-operative complication rate (2.3% vs. 5.7%), post-operative constipation (12.1% vs. 24.6%), mild and serious stress urinary incontinence (SUI) post-operative (P<0.001; P=0.014), and proportion of Female Sexual Functioning Index (FSFI) total score <26.55 post-operative (P<0.001) of the LH group were significantly less than those of AH group. There were no significant differences in OT (106.5±34.5 vs. 106.2±40.3 min) between the two groups. Conclusions: LH is a safe and efficient operation for improving patients?long-term quality of life (QoL), and LH is a cost-effectiveness procedure for treating benign gynecological disease. LH is superior to AH due to reduced EBL, reduced post-operative pain and earlier passing flatus.
2016, 28(2): 197-208.
doi: 10.21147/j.issn.1000-9604.2016.02.07
Abstract:
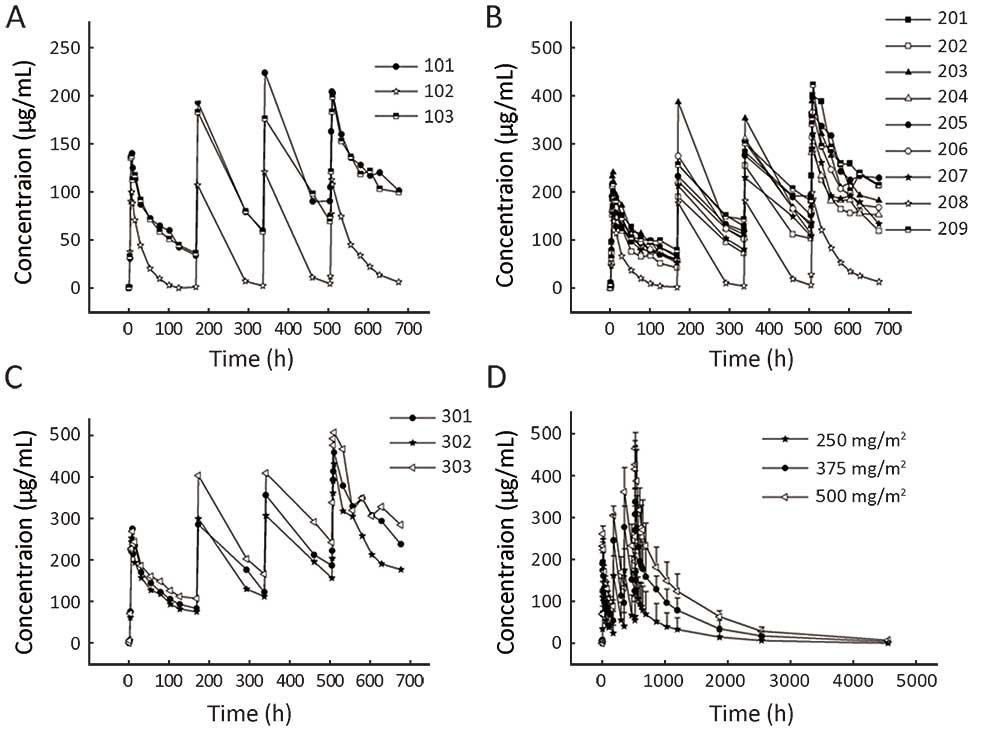
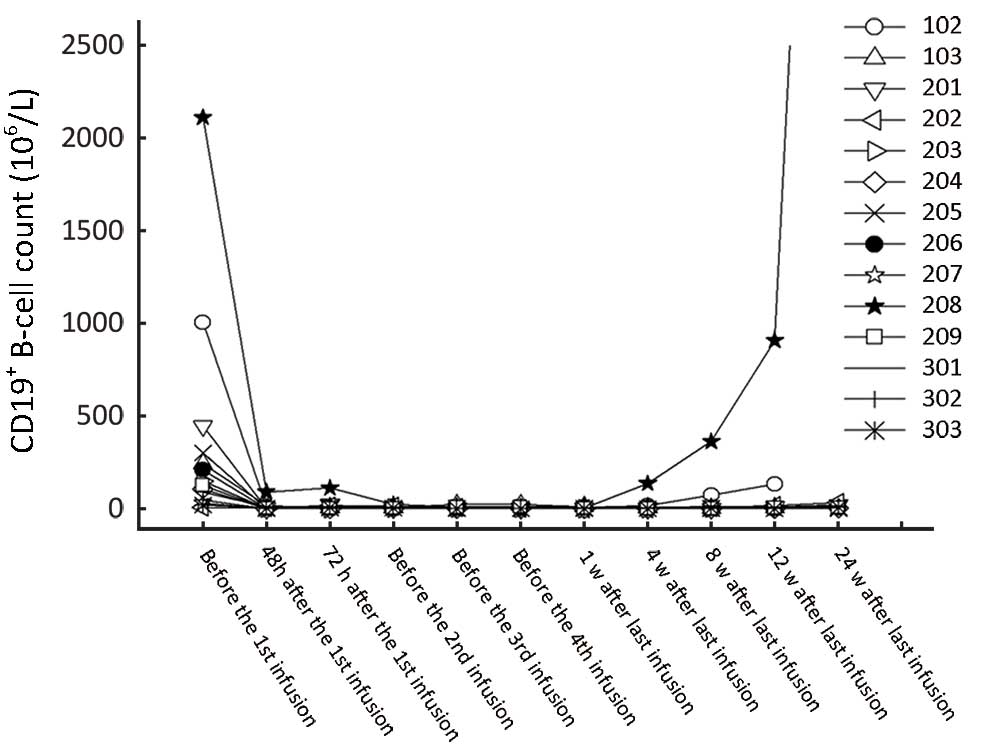
Objective: This study was designed to determine the safety, pharmacokinetics and biologic effects of a human-mouse chimeric anti-CD20 monoclonal antibody (SCT400) in Chinese patients with CD20-positive B-cell non-Hodgkin's lymphoma (CD20+ B-cell NHL). SCT400 has an identical amino acid sequence as rituximab, with the exception of one amino acid in the CH1 domain of the heavy chain, which is common in Asians. Methods: Fifteen patients with CD20+ B-cell NHL received dose-escalating SCT400 infusions (250 mg/m2: n=3; 375 mg/m2: n=9; 500 mg/m2: n=3) once weekly for 4 consecutive weeks with a 24-week follow-up period. The data of all patients were collected for pharmacokinetics and pharmacodynamics analyses. Results: No dose-limiting toxicities were observed. Most drug-related adverse events were grade 1 or 2. Two patients had grade 3 or 4 neutropenia. Under premedication, the drug-related infusion reaction was mild. A rapid, profound and durable depletion of circulating B cells was observed in all dose groups without significant effects on T cell count, natural killer (NK) cell count or immunoglobulin levels. No patient developed anti-SCT400 antibodies during the course of the study. SCT400 serum half-life (T1/2), maximum concentration (Cmax) and area under the curve (AUC) generally increased between the first and fourth infusions (P<0.05). At the 375 mg/m2 dose, the T1/2 was 122.5±46.7 h vs. 197.0±75.0 h, respectively, and the Cmax was 200.6±20.2 g/mL vs. 339.1±71.0 g/mL, respectively. From 250 mg/m2 to 500 mg/m2, the Cmax and AUC increased significantly in a dose-dependent manner (P<0.05). Patients with a high tumor burden had markedly lower serum SCT400 concentrations compared with those without or with a low tumor burden. Of the 9 assessable patients, 1 achieved complete response and 2 achieved partial responses. Conclusions: SCT400 is well-tolerated and has encouraging preliminary efficacy in Chinese patients with CD20+ B-cell NHL.

2016, 28(2): 209-214.
doi: 10.21147/j.issn.1000-9604.2016.02.08
Abstract:
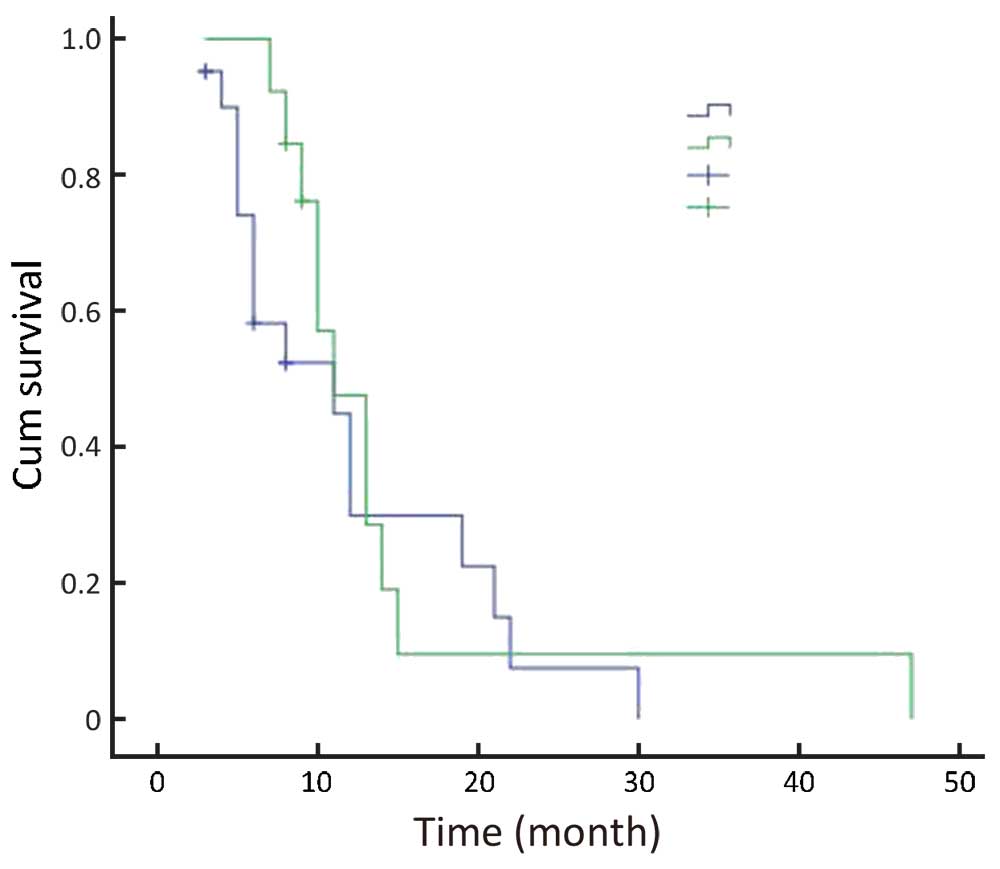
Objective: To evaluate the clinical and functional outcomes of modular endoprosthetic replacement (EPR) compared to proximal femur intramedullary nailing (IMN) for the treatment of proximal femur metastases. Methods: We retrospectively studied the records of patients with proximal femur metastatic lesions treated with surgical stabilization between January 2007 and December 2014 in terms of operation time, blood loss, postoperative score, soreness, Karnofsky performance score (KPS) and survival time. Results: There were 34 patients treated with surgical stabilization. The mean follow-up period was 12.1?.6 months (range: 10-47 months). Thirteen were treated with EPR and 21 were stabilized with IMN (20 males, 14 females; mean age: 68.7 years). The median survival time was 11.0 months for both groups (P=0.147). The operation time, blood loss and Harris score of IMN group were lower than those of EPR group (P=0.001, P=0.001, P=0.002, respectively). Conclusions: Both EPR and IMN for treating proximal femur metastasis achieved effective clinical outcomes. Therefore, the suitable surgical methods depended on the general conditions and medical requirements of patients, as well as the technical advantages of the doctor.


2016, 28(2): 215-220.
doi: 10.21147/j.issn.1000-9604.2016.02.09
Abstract:
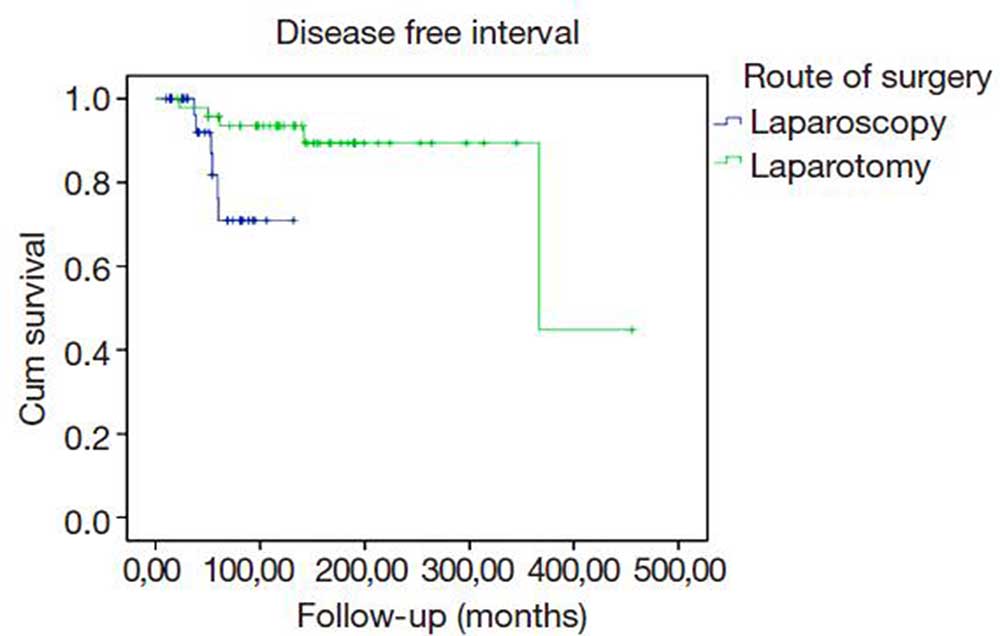
Background: The radical hysterectomy (RH) surgical technique has improved along the years. It is used for the treatment of cervical cancer, endometrial cancer when affecting the cervix, and upper vaginal carcinomas. Our aim was to describe the historical evolution of the technique after the introduction of laparoscopy at our institution. Methods: We performed a retrospective review of medical records of patients who underwent RH, grouped in three periods according to the year of surgery: 1990-1999, 2000-2009 and 2010-2013. Patients?characteristics, pathologic details, intraoperative and postoperative complications were analyzed and compared throughout the time periods. Results: A total of 102 cases of RH were performed at our center during the study period. Among all data collected, the presence of necrosis, age, number of lymph nodes, surgery route, operating time, hospital stay, blood loss and transfusion requirement were statistically significant different among groups. Conversion to laparotomy rate was 19% for the second period compared to the absence of cases in the last one. No significant differences (P=0.124) were observed in the adjuvant treatment received among the three different groups. At the time of the last contact the patients free of disease were 12 (85.7%), 53 (91.3%) and 26 (86.6%) respectively (P=0.406). Regarding the disease-free interval, we found significant better outcomes in the group of laparotomy compared to laparoscopy (P=0.015). Conclusions: Laparoscopic RH is an acceptable surgery with advantages like magnified vision of the operation抯 field, lower surgical complications, shorter hospital stay and earlier resumption to daily activities.
2016, 28(2): 221-227.
doi: 10.21147/j.issn.1000-9604.2016.02.10
Abstract:
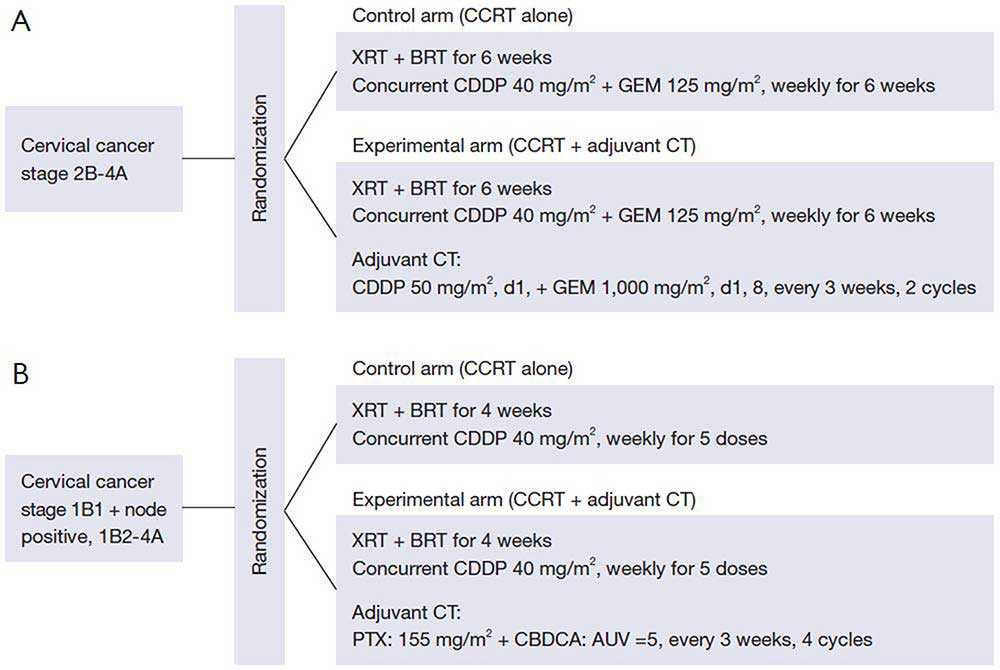
Concurrent chemoradiotherapy (CCRT) is regarded as the standard treatment for locally advanced uterine cervical cancer (LACC), including stage Ib2-IVa disease [International Federation of Gynecology and Obstetrics (FIGO) staging]. However, approximately a third of eligible patients in previous studies died of LACC despite receiving CCRT. The therapeutic significance of CCRT alone in stage III-IVa disease has not yet been confirmed. Effective treatment of some LACC is beyond the scope of CCRT. The objective of the present review is to highlight some challenging work aimed at overcoming this seemingly intractable disease. CCRT with increased peak concentrations of cisplatin (CDDP), surgery following CCRT, adjuvant chemotherapy (CT) following CCRT, and neoadjuvant CT followed by CCRT are strategies expected to enhance the therapeutic efficacy of CCRT. If patients with LACC were divided into those with low-risk or high-risk systemic disease or prognoses, novel strategies should be assessed in the group with high-risk disease.
Concurrent chemoradiotherapy (CCRT) is regarded as the standard treatment for locally advanced uterine cervical cancer (LACC), including stage Ib2-IVa disease [International Federation of Gynecology and Obstetrics (FIGO) staging]. However, approximately a third of eligible patients in previous studies died of LACC despite receiving CCRT. The therapeutic significance of CCRT alone in stage III-IVa disease has not yet been confirmed. Effective treatment of some LACC is beyond the scope of CCRT. The objective of the present review is to highlight some challenging work aimed at overcoming this seemingly intractable disease. CCRT with increased peak concentrations of cisplatin (CDDP), surgery following CCRT, adjuvant chemotherapy (CT) following CCRT, and neoadjuvant CT followed by CCRT are strategies expected to enhance the therapeutic efficacy of CCRT. If patients with LACC were divided into those with low-risk or high-risk systemic disease or prognoses, novel strategies should be assessed in the group with high-risk disease.
2016, 28(2): 228-234.
doi: 10.21147/j.issn.1000-9604.2016.02.12
Abstract:
The aim of this review is to address the current status of adjuvant chemotherapy alone in early-stage cervical cancer treatments in the literature. At present, the therapeutic effect of adjuvant chemotherapy alone after radical surgery (RS) has not yet been established, and radiation therapy (RT) or concurrent chemoradiotherapy (CCRT) is recommended as the standard adjuvant therapy after RS for early-stage cervical cancer in various guidelines. The main purpose of adjuvant therapy after RS, however, should be to reduce extrapelvic recurrence rather than local recurrence, although adjuvant RT or CCRT has survival benefits for patients with intermediate- or high-risk factors for recurrence. Moreover, several studies reported that adjuvant therapies including RT were associated with a higher incidence of complications, such as lymphedema, bowel obstruction and urinary disturbance, and a lower grade of long-term quality of life (QOL) or sexual functioning than adjuvant chemotherapy alone. The effect of adjuvant chemotherapy alone for early-stage cervical cancer with intermediate- or high-risk factors for recurrence were not fully investigated in prospective studies, but several retrospective studies suggest that the adjuvant effects of chemotherapy alone are at least similar to that of RT or CCRT in terms of recurrence rate, disease-free survival, or overall survival (OS) with lower incidence of complications. Whereas cisplatin based combination regimens were used in these studies, paclitaxel/cisplatin (TP) regimen, which is currently recognized as a standard chemotherapy regimen for patients with metastatic, recurrent or persistent cervical cancer by Gynecologic Oncology Group (GOG), had also survival benefit as an adjuvant therapy. Therefore, it may be worth considering a prospective randomized controlled trial (RCT) of adjuvant chemotherapy alone using TP regimen versus adjuvant RT as an alternative adjuvant therapy. Because early-stage cervical cancer is a curable condition, it is necessary that the therapeutic strategies should be improved with considering adverse events and QOL for long-term survivors.
The aim of this review is to address the current status of adjuvant chemotherapy alone in early-stage cervical cancer treatments in the literature. At present, the therapeutic effect of adjuvant chemotherapy alone after radical surgery (RS) has not yet been established, and radiation therapy (RT) or concurrent chemoradiotherapy (CCRT) is recommended as the standard adjuvant therapy after RS for early-stage cervical cancer in various guidelines. The main purpose of adjuvant therapy after RS, however, should be to reduce extrapelvic recurrence rather than local recurrence, although adjuvant RT or CCRT has survival benefits for patients with intermediate- or high-risk factors for recurrence. Moreover, several studies reported that adjuvant therapies including RT were associated with a higher incidence of complications, such as lymphedema, bowel obstruction and urinary disturbance, and a lower grade of long-term quality of life (QOL) or sexual functioning than adjuvant chemotherapy alone. The effect of adjuvant chemotherapy alone for early-stage cervical cancer with intermediate- or high-risk factors for recurrence were not fully investigated in prospective studies, but several retrospective studies suggest that the adjuvant effects of chemotherapy alone are at least similar to that of RT or CCRT in terms of recurrence rate, disease-free survival, or overall survival (OS) with lower incidence of complications. Whereas cisplatin based combination regimens were used in these studies, paclitaxel/cisplatin (TP) regimen, which is currently recognized as a standard chemotherapy regimen for patients with metastatic, recurrent or persistent cervical cancer by Gynecologic Oncology Group (GOG), had also survival benefit as an adjuvant therapy. Therefore, it may be worth considering a prospective randomized controlled trial (RCT) of adjuvant chemotherapy alone using TP regimen versus adjuvant RT as an alternative adjuvant therapy. Because early-stage cervical cancer is a curable condition, it is necessary that the therapeutic strategies should be improved with considering adverse events and QOL for long-term survivors.
2016, 28(2): 235-240.
doi: 10.21147/j.issn.1000-9604.2016.02.13
Abstract:
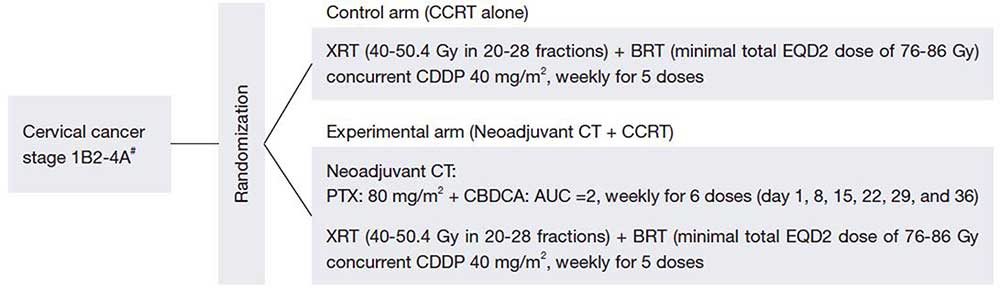
Neoadjuvant chemotherapy followed by surgery (NCS) has not been fully evaluated clinically. Currently, the main regimen of neoadjuvant chemotherapy (NAC) used in NCS includes cisplatin. The antitumor effects of NAC reduce lymph node metastasis and the tumor diameter in patients prior to surgery, and this can reduce the number of high risk patients who require postoperative radiation therapy. Many randomized controlled trials (RCTs) have examined the long-term prognosis of NCS compared to primary surgery, but the utility of NCS remains uncertain. The advent of concurrent chemoradiotherapy (CCRT) has markedly improved the outcome of radiotherapy (RT), and CCRT is now used as a standard method in many cases of advanced bulky cervical cancer. NCS gives a better treatment outcome than radiation therapy alone, but it is important to verify that NCS gives a similar or better outcome compared to CCRT.
Neoadjuvant chemotherapy followed by surgery (NCS) has not been fully evaluated clinically. Currently, the main regimen of neoadjuvant chemotherapy (NAC) used in NCS includes cisplatin. The antitumor effects of NAC reduce lymph node metastasis and the tumor diameter in patients prior to surgery, and this can reduce the number of high risk patients who require postoperative radiation therapy. Many randomized controlled trials (RCTs) have examined the long-term prognosis of NCS compared to primary surgery, but the utility of NCS remains uncertain. The advent of concurrent chemoradiotherapy (CCRT) has markedly improved the outcome of radiotherapy (RT), and CCRT is now used as a standard method in many cases of advanced bulky cervical cancer. NCS gives a better treatment outcome than radiation therapy alone, but it is important to verify that NCS gives a similar or better outcome compared to CCRT.
2016, 28(2): 241-253.
doi: 10.21147/j.issn.1000-9604.2016.02.14
Abstract:
For patients with primary stage ⅣB, persistent, or recurrent cervical cancer, chemotherapy remains the standard treatment, although it is neither curative nor associated with long-term disease control. In this review, we summarized the history of treatment of recurrent cervical cancer, and the current recommendation for chemotherapy and molecular targeted therapy. Eligible articles were identified by a search of the MEDLINE bibliographical database for the period up to November 30, 2014. The search strategy included the following any or all of the keywords: “uterine cervical cancer”, “chemotherapy”, and “targeted therapies”. Since cisplatin every 21 days was considered as the historical standard treatment for recurrent cervical cancer, subsequent trials have evaluated and demonstrated activity for other agents including paclitaxel, gemcitabine, topotecan and vinorelbine among others. Accordingly, promising agents were incorporated into phase Ⅲ trials. To examine the best agent to combine with cisplatin, several landmark phase Ⅲ clinical trials were conducted by Gynecologic Oncology Group (GOG) and Japan Clinical Oncology Group (JCOG). Through, GOG204 and JCOG0505, paclitaxel/cisplatin (TP) and paclitaxel/carboplatin (TC) are now considered to be the recommended therapies for recurrent cervical cancer patients. However, the prognosis of patients who are already resistant to chemotherapy, are very poor. Therefore new therapeutic strategies are urgently required. Molecular targeted therapy will be the most hopeful candidate of these strategies. From the results of GOG240, bevacizumab combined with TP reached its primary endpoint of improving overall survival (OS). Although, the prognosis for recurrent cervical cancer patients is still poor, the results of GOG240 shed light on the usefulness of molecular target agents to chemotherapy in cancer patients. Recurrent cervical cancer is generally considered incurable and current chemotherapy regiments offer only modest gains in OS, particularly for patients with multiple poor prognostic factors. Therefore, it is crucial to consider not only the survival benefit, but also the minimization of treatment toxicity, and maximization of quality of life (QOL).
For patients with primary stage ⅣB, persistent, or recurrent cervical cancer, chemotherapy remains the standard treatment, although it is neither curative nor associated with long-term disease control. In this review, we summarized the history of treatment of recurrent cervical cancer, and the current recommendation for chemotherapy and molecular targeted therapy. Eligible articles were identified by a search of the MEDLINE bibliographical database for the period up to November 30, 2014. The search strategy included the following any or all of the keywords: “uterine cervical cancer”, “chemotherapy”, and “targeted therapies”. Since cisplatin every 21 days was considered as the historical standard treatment for recurrent cervical cancer, subsequent trials have evaluated and demonstrated activity for other agents including paclitaxel, gemcitabine, topotecan and vinorelbine among others. Accordingly, promising agents were incorporated into phase Ⅲ trials. To examine the best agent to combine with cisplatin, several landmark phase Ⅲ clinical trials were conducted by Gynecologic Oncology Group (GOG) and Japan Clinical Oncology Group (JCOG). Through, GOG204 and JCOG0505, paclitaxel/cisplatin (TP) and paclitaxel/carboplatin (TC) are now considered to be the recommended therapies for recurrent cervical cancer patients. However, the prognosis of patients who are already resistant to chemotherapy, are very poor. Therefore new therapeutic strategies are urgently required. Molecular targeted therapy will be the most hopeful candidate of these strategies. From the results of GOG240, bevacizumab combined with TP reached its primary endpoint of improving overall survival (OS). Although, the prognosis for recurrent cervical cancer patients is still poor, the results of GOG240 shed light on the usefulness of molecular target agents to chemotherapy in cancer patients. Recurrent cervical cancer is generally considered incurable and current chemotherapy regiments offer only modest gains in OS, particularly for patients with multiple poor prognostic factors. Therefore, it is crucial to consider not only the survival benefit, but also the minimization of treatment toxicity, and maximization of quality of life (QOL).
2016, 28(2): 254-262.
doi: 10.21147/j.issn.1000-9604.2016.02.11
Abstract:
Uterine cervical adenocarcinoma (ADC) has been increasing in its prevalence world widely despite the decrease of squamous cell carcinoma (SCC). It comprises nearly 20-25% of the all cervical malignancy in developed countries. The worse biological behavior had been reported in patients with intermediate- and high risk factors after surgery, and in advanced stage over Ⅲ, radiotherapy (RT) alone and concurrent chemo-radiotherapy (CCRT) with cisplatin was not always effective. As for chemotherapy (CT), the induction CT has not established, as well. Further molecular targeted therapy (MTT) has been studied. The targets of oncogenic driver mutations were vascular endothelial growth factor (VEGF) in SCC, or tyrosine kinase (TK) of endothelial growth factor receptor 2 (EGFR2, Her2/neu)-Ras-MAPK-ERK pathway. Bevacizumab (Bev, anti-VEGF monoclonal antibody) is considered as one of key agent with paclitaxel and carboplatin in SCC, but not for ADC. This article focuses on up-to-date knowledge of biology and possible specific therapeutic directions to explore in the management of cervical ADC.
Uterine cervical adenocarcinoma (ADC) has been increasing in its prevalence world widely despite the decrease of squamous cell carcinoma (SCC). It comprises nearly 20-25% of the all cervical malignancy in developed countries. The worse biological behavior had been reported in patients with intermediate- and high risk factors after surgery, and in advanced stage over Ⅲ, radiotherapy (RT) alone and concurrent chemo-radiotherapy (CCRT) with cisplatin was not always effective. As for chemotherapy (CT), the induction CT has not established, as well. Further molecular targeted therapy (MTT) has been studied. The targets of oncogenic driver mutations were vascular endothelial growth factor (VEGF) in SCC, or tyrosine kinase (TK) of endothelial growth factor receptor 2 (EGFR2, Her2/neu)-Ras-MAPK-ERK pathway. Bevacizumab (Bev, anti-VEGF monoclonal antibody) is considered as one of key agent with paclitaxel and carboplatin in SCC, but not for ADC. This article focuses on up-to-date knowledge of biology and possible specific therapeutic directions to explore in the management of cervical ADC.


