
2017 Vol.29(3)
Display Mode: |
2017, 29(3): 171-171.
doi: 10.21147/j.issn.1000-9604.2017.03.01
 Abstract
Abstract FullText HTML
FullText HTML PDF 327KB
PDF 327KB
Abstract:
2017, 29(3): 172-178.
doi: 10.21147/j.issn.1000-9604.2017.03.02
Abstract:
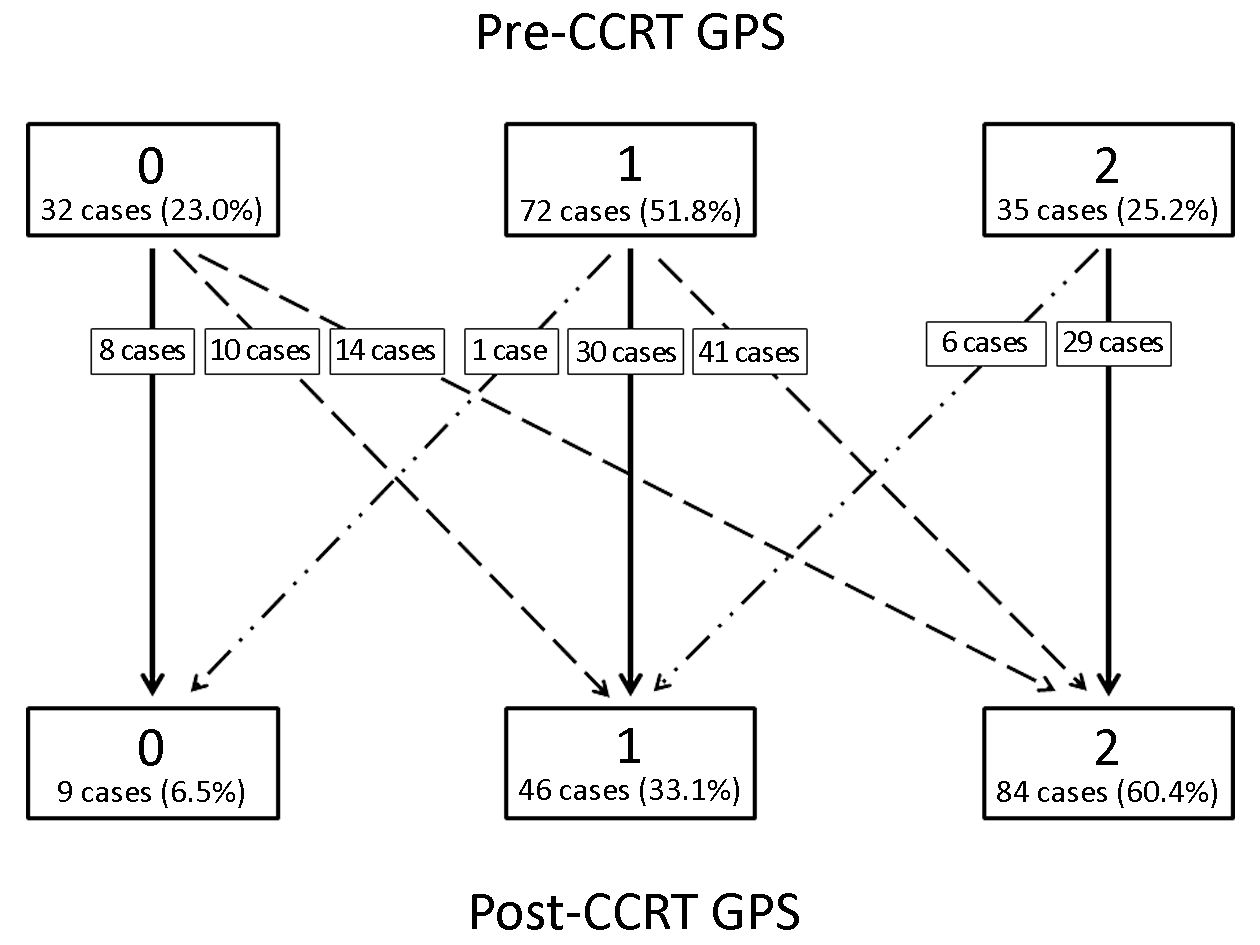
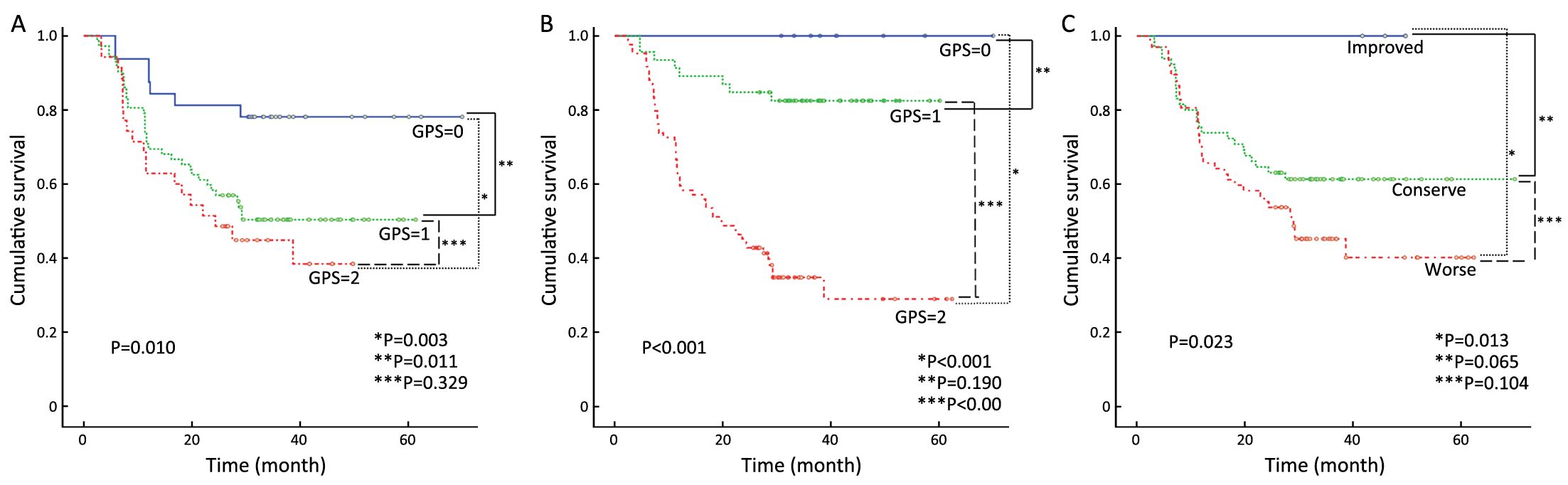
Objective This study aims to evaluate the impact and potential prognostic roles of the pre- and post-treatment Glasgow prognostic score (GPS) and the change thereof in patients with advanced head and neck cancer undergoing concurrent chemoradiotherapy (CCRT). Methods We collected GPS and clinicopathological data of 139 stage III, IVA, and IVB head and neck cancer patients who underwent CCRT between 2008 and 2011. Their GPSs pre- and post-CCRT and the change thereof were analyzed for correlations with recurrence and survival. Results The GPS changed in 72 (51.8%) patients, with worse scores observed post-CCRT in 65 (90.3%) of the GPS changed patients. Patients in the improved GPS group showed a tendency toward better survival. From the multivariate analysis, the post-CCRT GPS level was an independent prognostic factor in addition to tumor stage. Conclusions After CCRT, a high GPS was revealed to be an important predictor of survival for advanced head and neck cancer.

2017, 29(3): 179-188.
doi: 10.21147/j.issn.1000-9604.2017.03.03
Abstract:
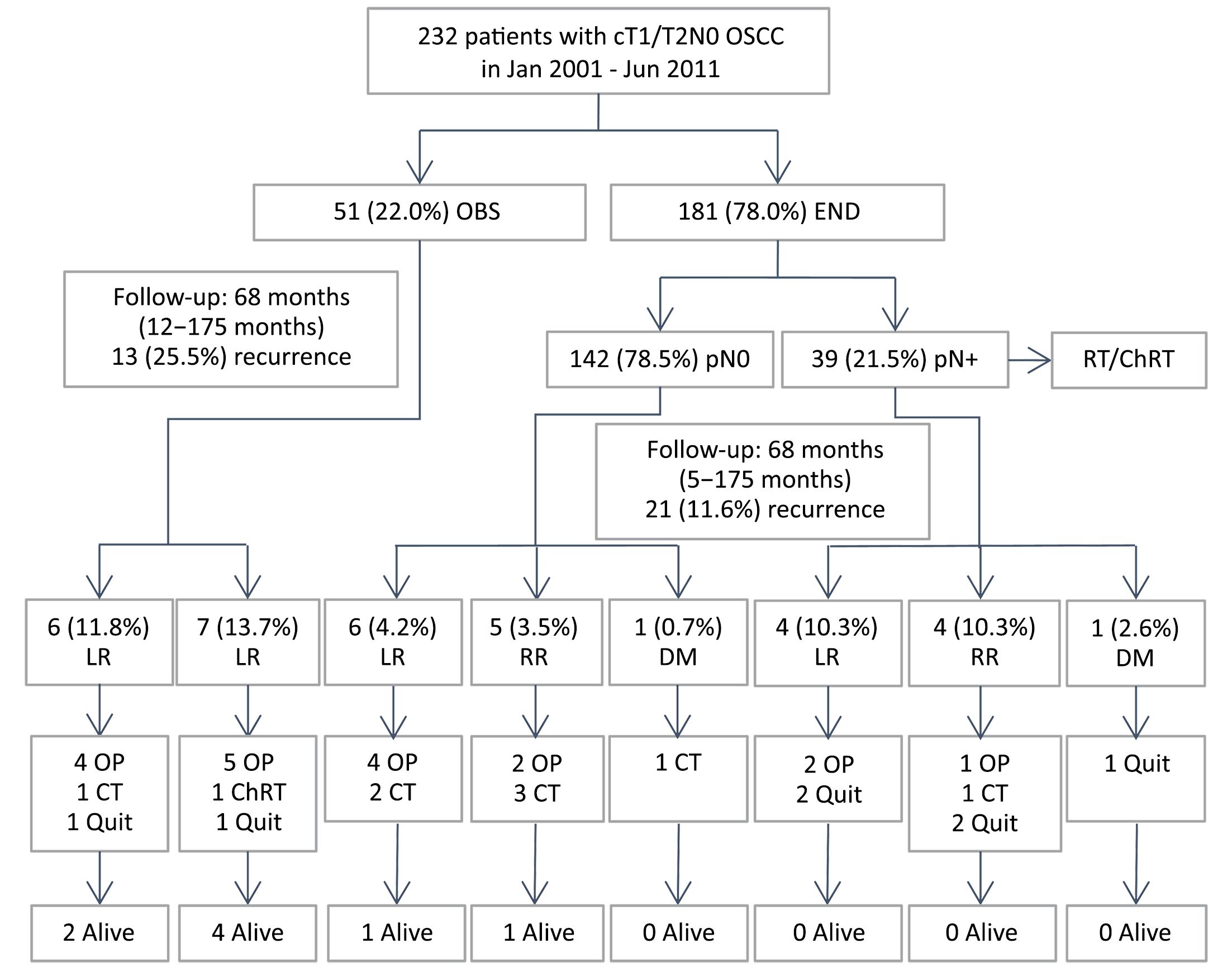
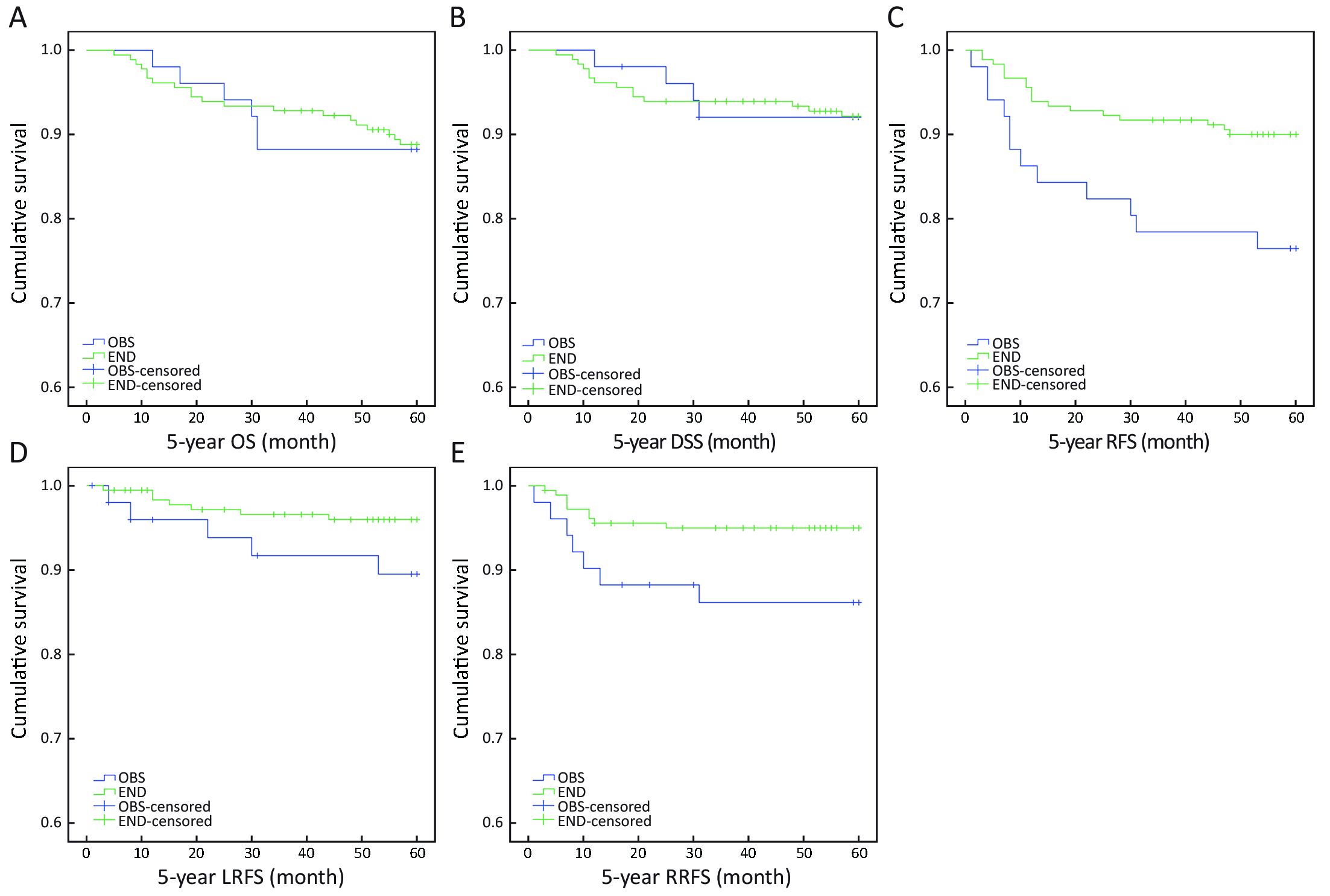
Objective The management of early-stage (cT1/2N0) oral squamous cell carcinoma (OSCC) remains a controversial issue. The aim of this study was to compare the clinical outcomes of neck observation (OBS) and elective neck dissection (END) in treating patients with cT1/2N0 OSCC. Methods A total of 232 patients with cT1/2N0 OSCC were included in this retrospective study. Of these patients, 181 were treated with END and 51 with OBS. The survival curves of 5-year overall survival (OS), disease-specific survival (DSS), and recurrence-free survival (RFS) rates were plotted using the Kaplan-Meier method for each group, and compared using the Log-rank test. Results There was no significant difference in 5-year OS and DSS rates between END and OBS groups (OS: 89.0% vs. 88.2%, P=0.906; DSS: 92.3% vs. 92.2%, P=0.998). However, the END group had a higher 5-year RFS rate than the OBS group (90.1% vs. 76.5%, P=0.009). Patients with occult metastases in OBS group (7/51) had similar 5-year OS rate (57.1% vs. 64.1%, P=0.839) and DSS rate (71.4% vs. 74.4%, P=0.982) to those in END group (39/181). In the regional recurrence patients, the 5-year OS rate (57.1% vs. 11.1%, P=0.011) and DSS rate (71.4% vs. 22.2%, P=0.022) in OBS group (7/51) were higher than those in END group (9/181). Conclusions The results indicated that OBS policy could obtain the same 5-year OS and DSS as END. Under close follow-up, OBS policy may be an available treatment option for patients with clinical T1/2N0 OSCC.
2017, 29(3): 189-195.
doi: 10.21147/j.issn.1000-9604.2017.03.04
Abstract:
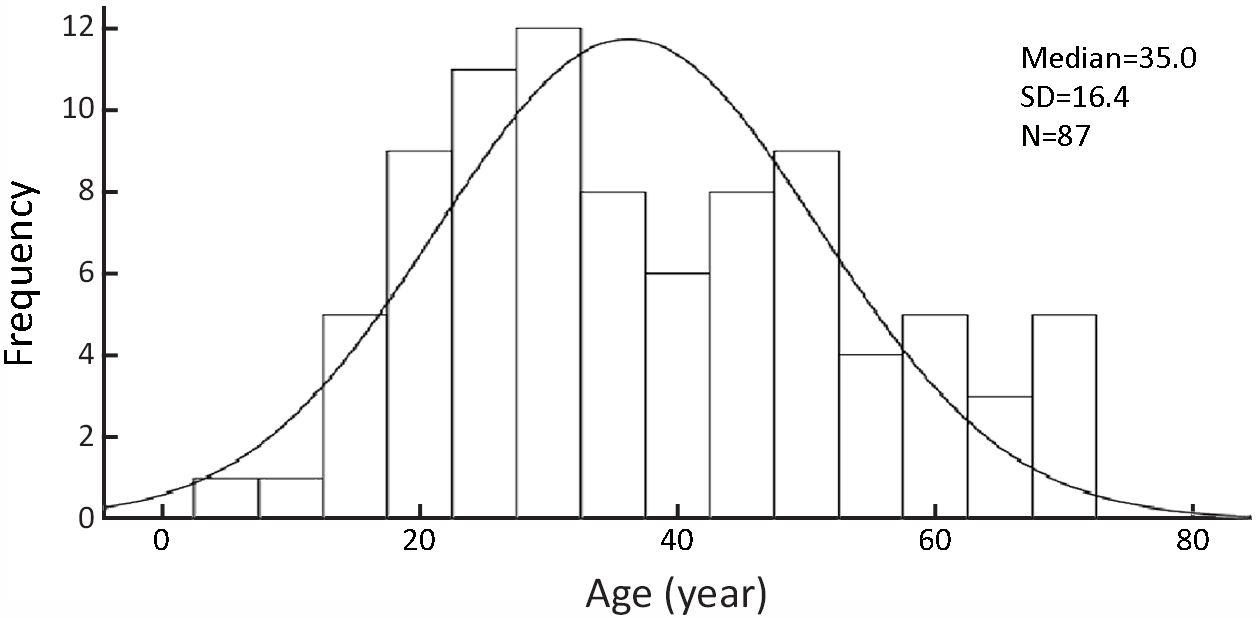
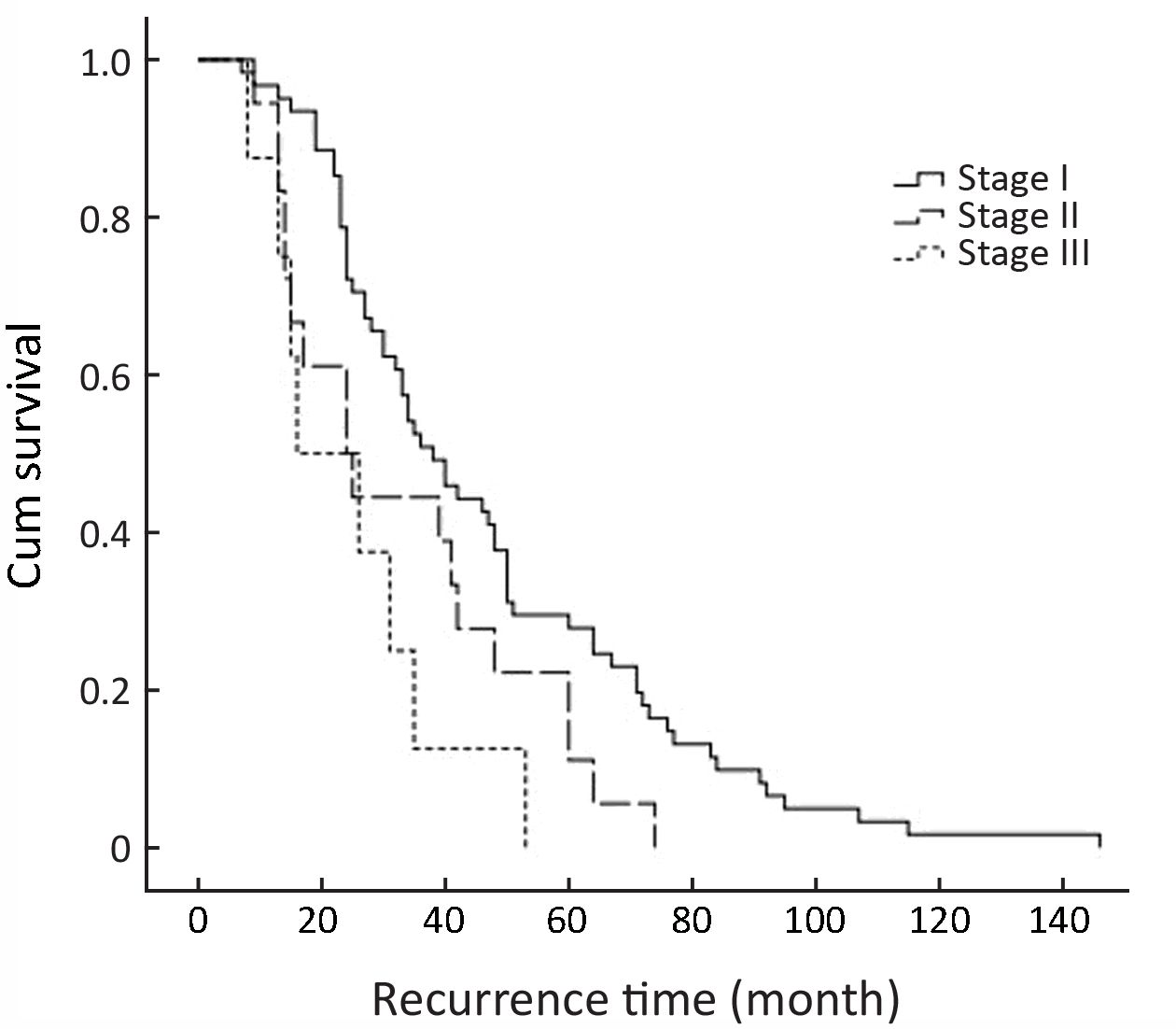
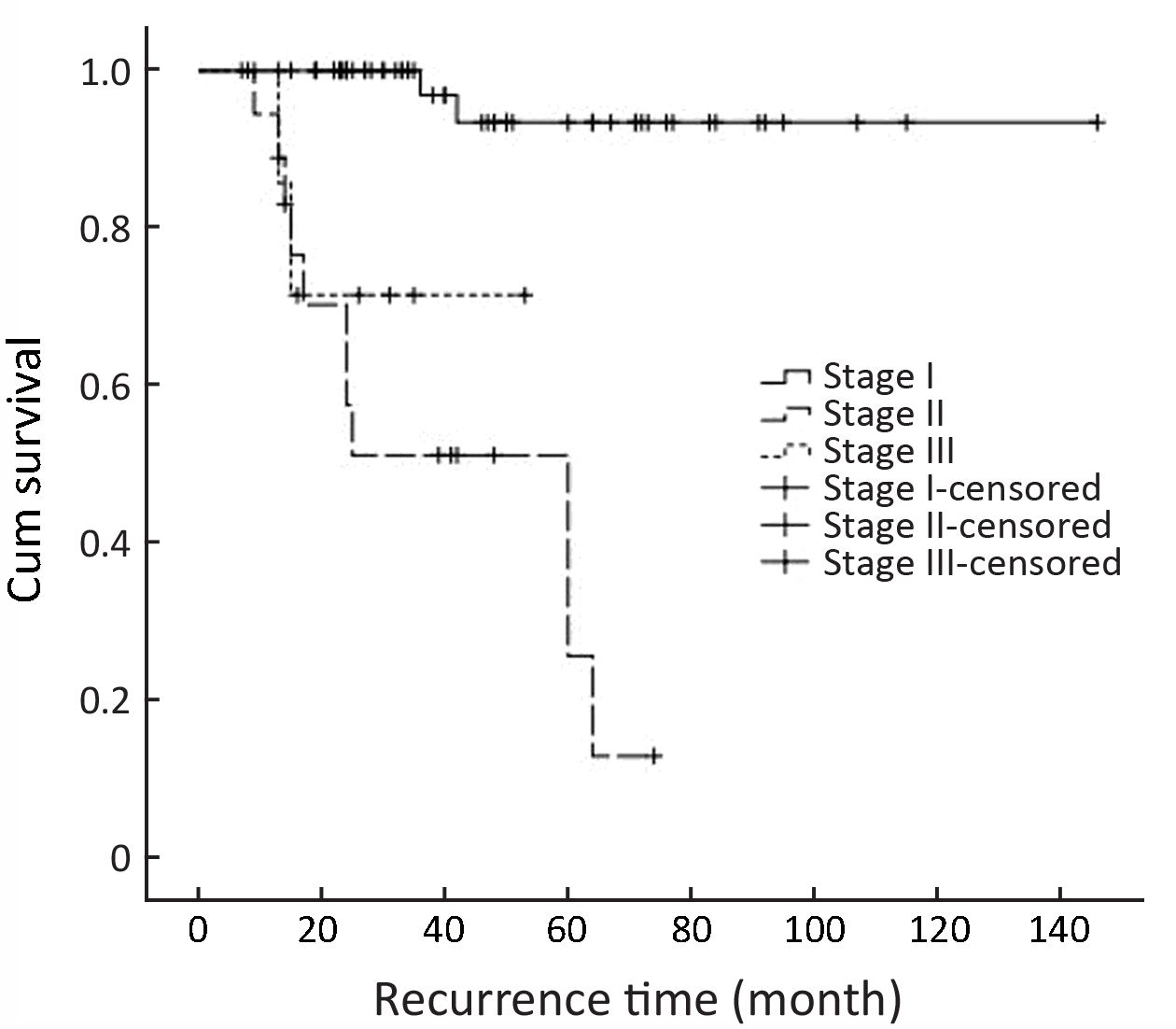
Objective The recurrence and progression of ameloblastoma are unpredictable. Therefore, we examined the influence of clinical factors on recurrence time and analyzed the clinical factors associated with early recurrence and cancerization. We then developed a staging system to predict early recurrence and cancerization. Methods All of the primary craniofacial ameloblastoma patients treated in Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine were recorded. There were 87 recurrent cases used to create a staging system and tested in a Cox regression analysis for risk factors associated with early recurrence or cancerization following surgery. Results There were 890 craniofacial ameloblastoma patients, and 72 cases had recurrence. There were also 15 cases with cancerous recurrence. The overall recurrence rate was 9.78%, and the cancer rate was 1.69%. The primary cases were classified into the following 3 stages based on clinicopathological features: stage I, the maximum tumor diameter ≤6 cm; stage II, the maximum diameter of tumor >6 cm or tumor invasion to the maxilla sinus/orbital floor/soft tissue; and stage III, tumor invasion of the skull base or metastasis into regional lymph nodes. When the method of surgery was controlled by partial correlation, the staging had significance with recurrence time (P=0.004). The Cox analysis showed the tumor stage was correlated with recurrence time (P=0.027) and cancerization time (P=0.002). However, the surgical method did not influence the recurrence time when adjusted for cofounding variables. Conclusions Tumor larger than 6 cm and invasion to soft tissues or adjacent anatomical structures are associated with early recurrence. This staging system can be used to predict the risk factors of early recurrence and cancerization in ameloblastoma patients.

2017, 29(3): 196-203.
doi: 10.21147/j.issn.1000-9604.2017.03.05
Abstract:
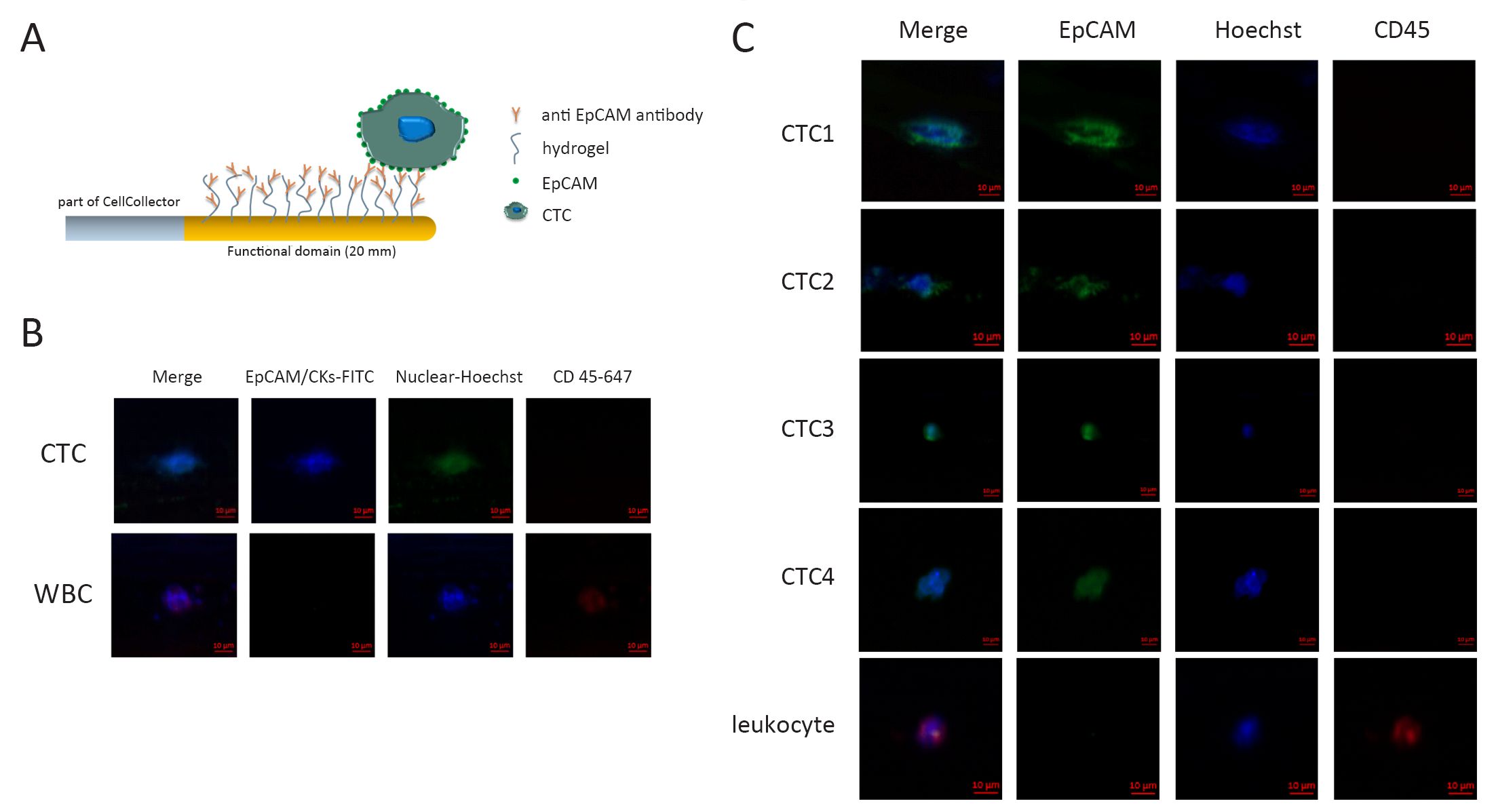
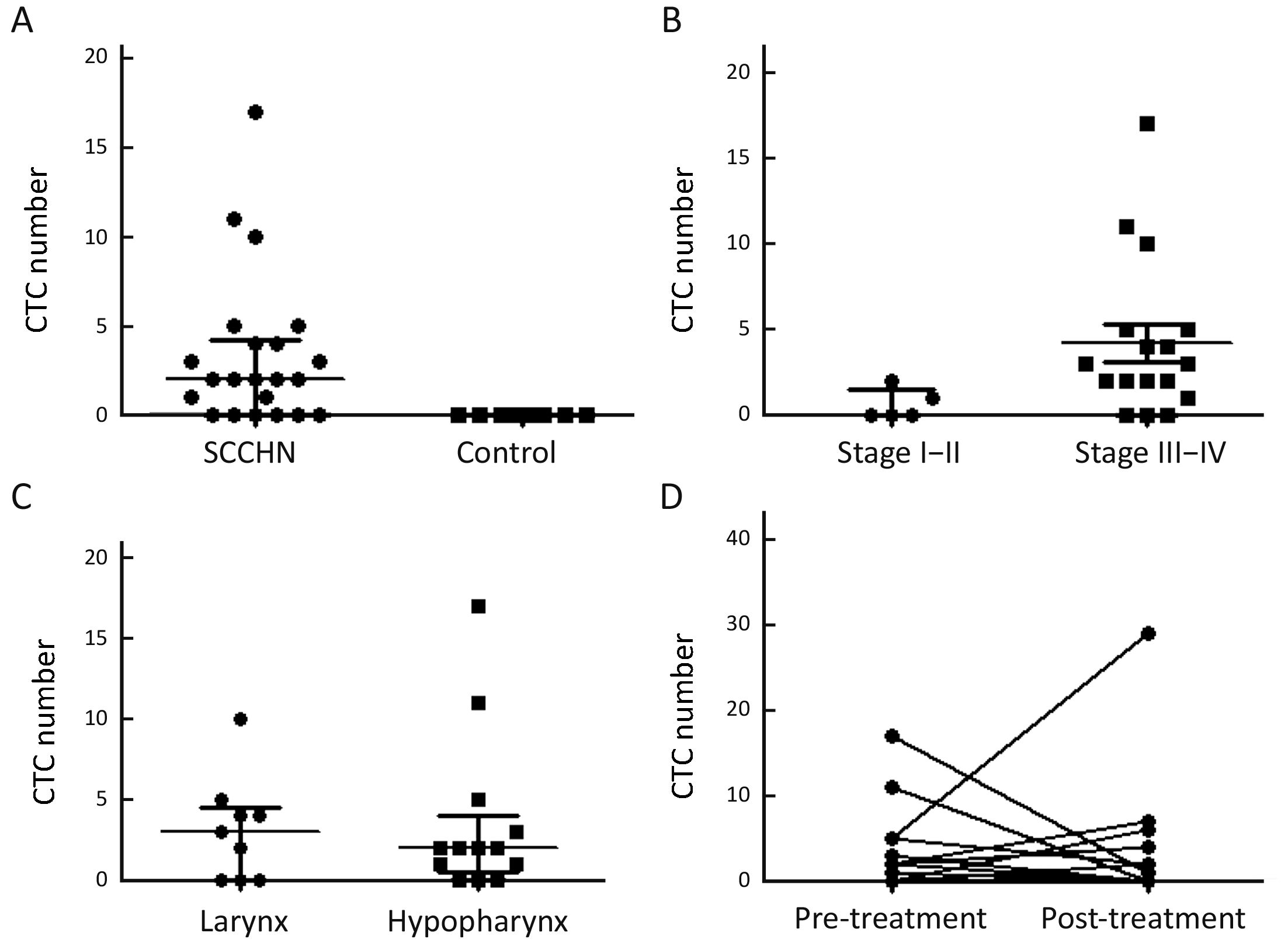
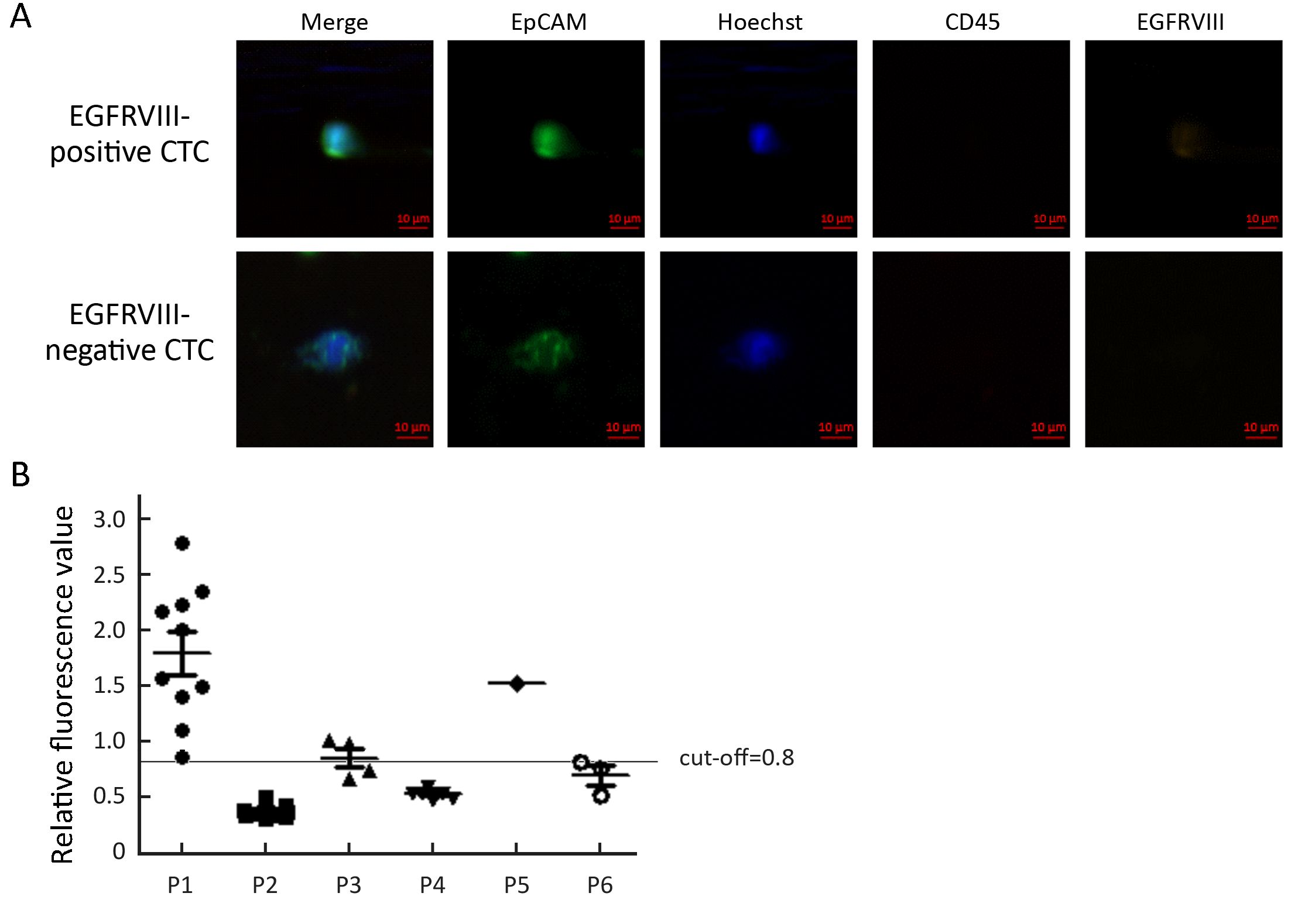
Objective Detection rate and isolation yield of circulating tumor cell (CTC) are low in squamous cell carcinoma of head and neck (SCCHN) with in vitro approaches due to limited sample volumes. In this study, we applied the CellCollector to capture CTC in vivo from peripheral blood. Methods In total, the study included 22 cases with 37 times of detection. All of the patients were newly diagnosed with locally advanced or metastatic SCCHN, including laryngocarcinoma (40.9%, 9/22) and hypopharyngeal carcinoma (59.1%, 13/22). All patients received CTC analysis before treatment. Three patients received induction chemotherapy. Sixteen patients received surgical therapy, of which 13 patients received postoperative detection. Two patients received both induction chemotherapy and surgery treatment. Patients underwent two successive CellCollector applications 24 h before and 7 d after surgical therapy. Nine healthy volunteers were enrolled as the control group. Epidermal growth factor receptor variant type III (EGFRVIII) expression was analyzed with fluorescent dye labeled antibody. Results With CellCollector isolation, 72.7% (16/22) of the patients were positive for ≥1 CTC (CTC; range, 1–17 cells) before treatments and 46.7% (7/15) of patients were CTC positive for ≥1 CTC (CTC; range, 1–29 cells) after surgical therapy. Moreover, the detection rate of CellCollector (82.4%, 14/17; CTC count range, 0–17) in advanced SCCHN (stage III–IV) was much higher than that in early stages (stage I–II, 40.0%, 2/5; CTC count range, 0–2) (P<0.05). EGFRVIII expression of CTC was also analyzed with fluorescence staining. One CTCEGFRVIII-positive patient was detected from six CTC-positive patients, and the positive expression of EGFRVIII was also found in the tumor tissue of this patient. Conclusions In vivo detection of CTCs had high sensitivity in SCCHN, which might improve CTC application in clinic.
2017, 29(3): 204-212.
doi: 10.21147/j.issn.1000-9604.2017.03.06
Abstract:
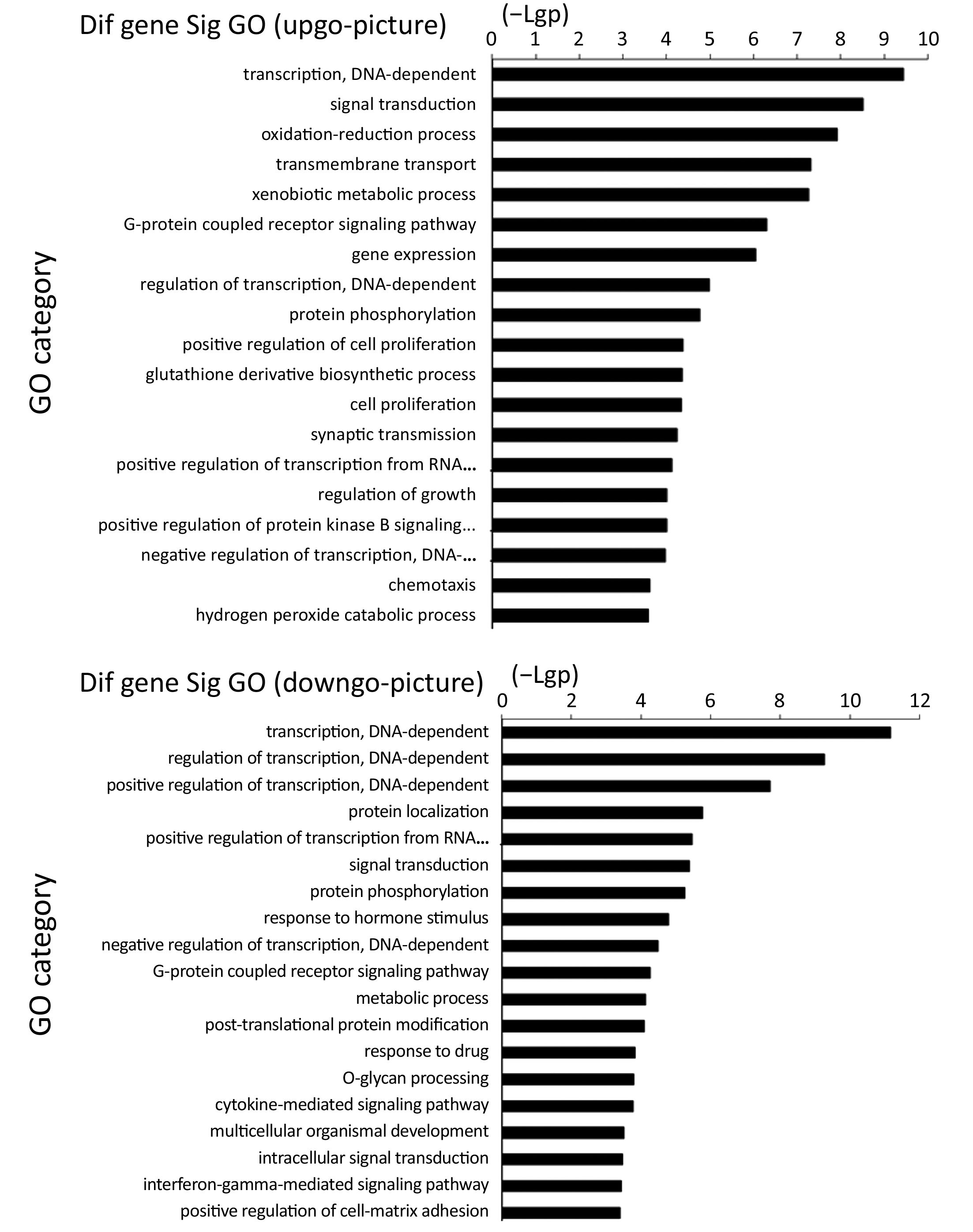
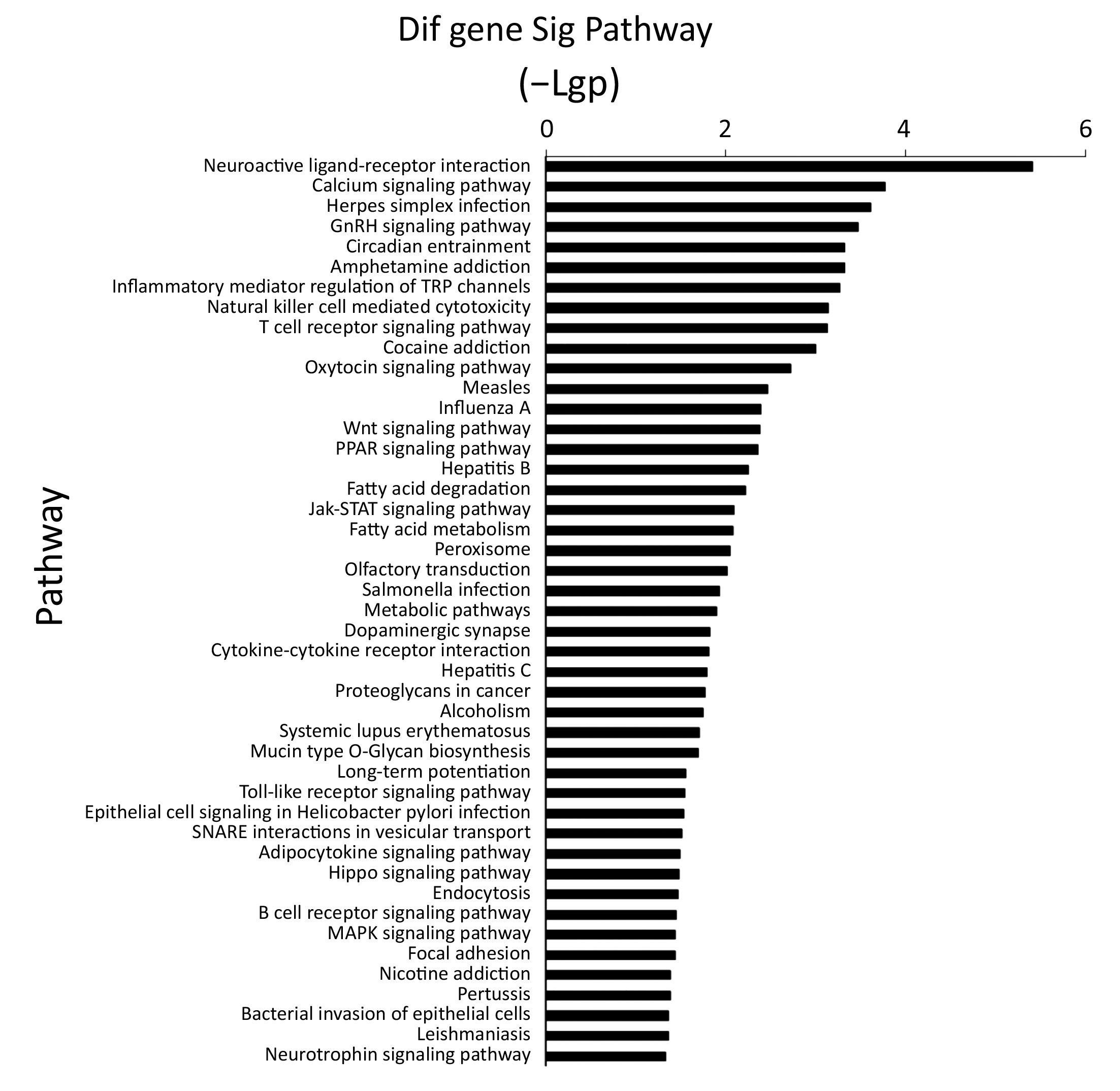
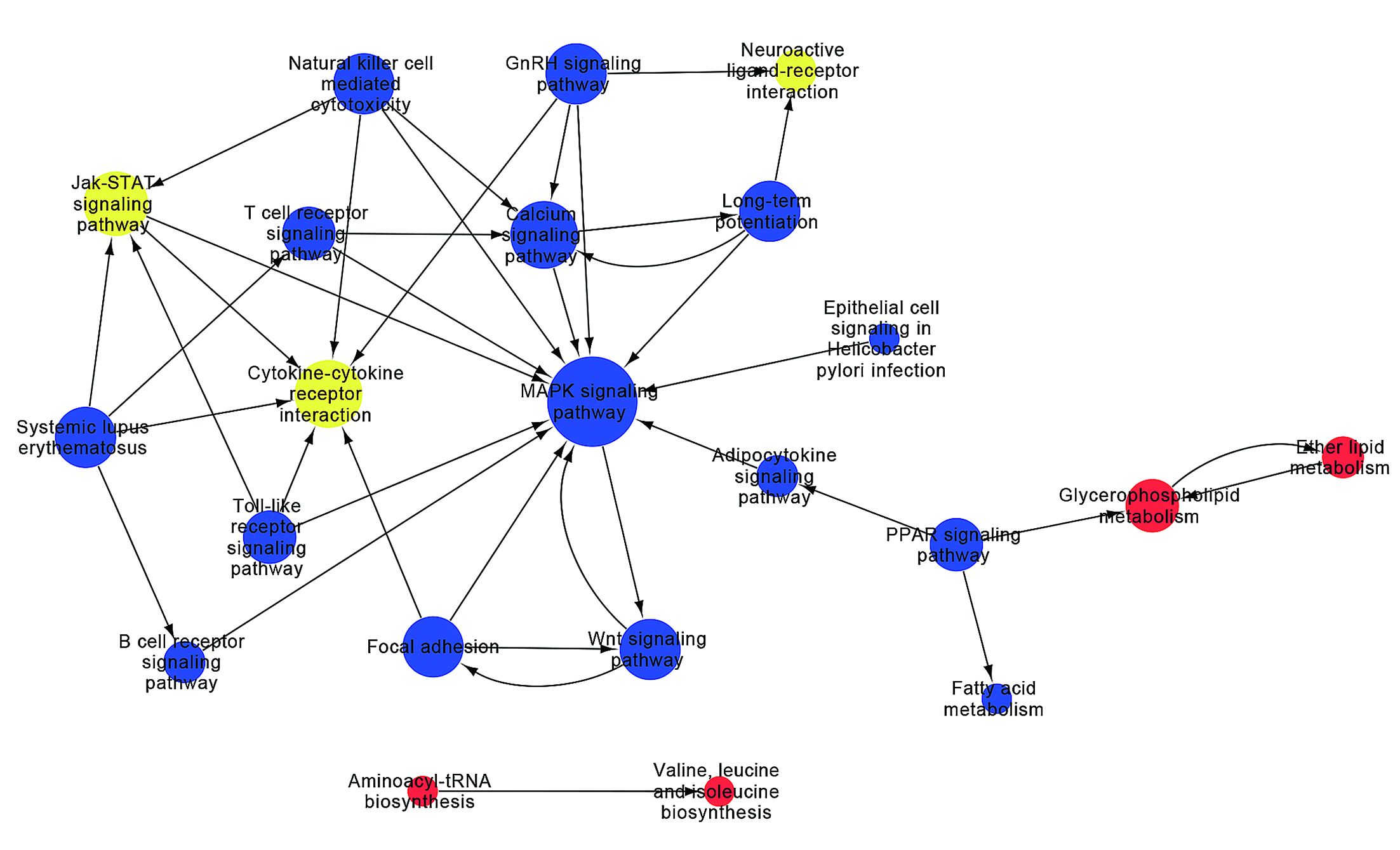
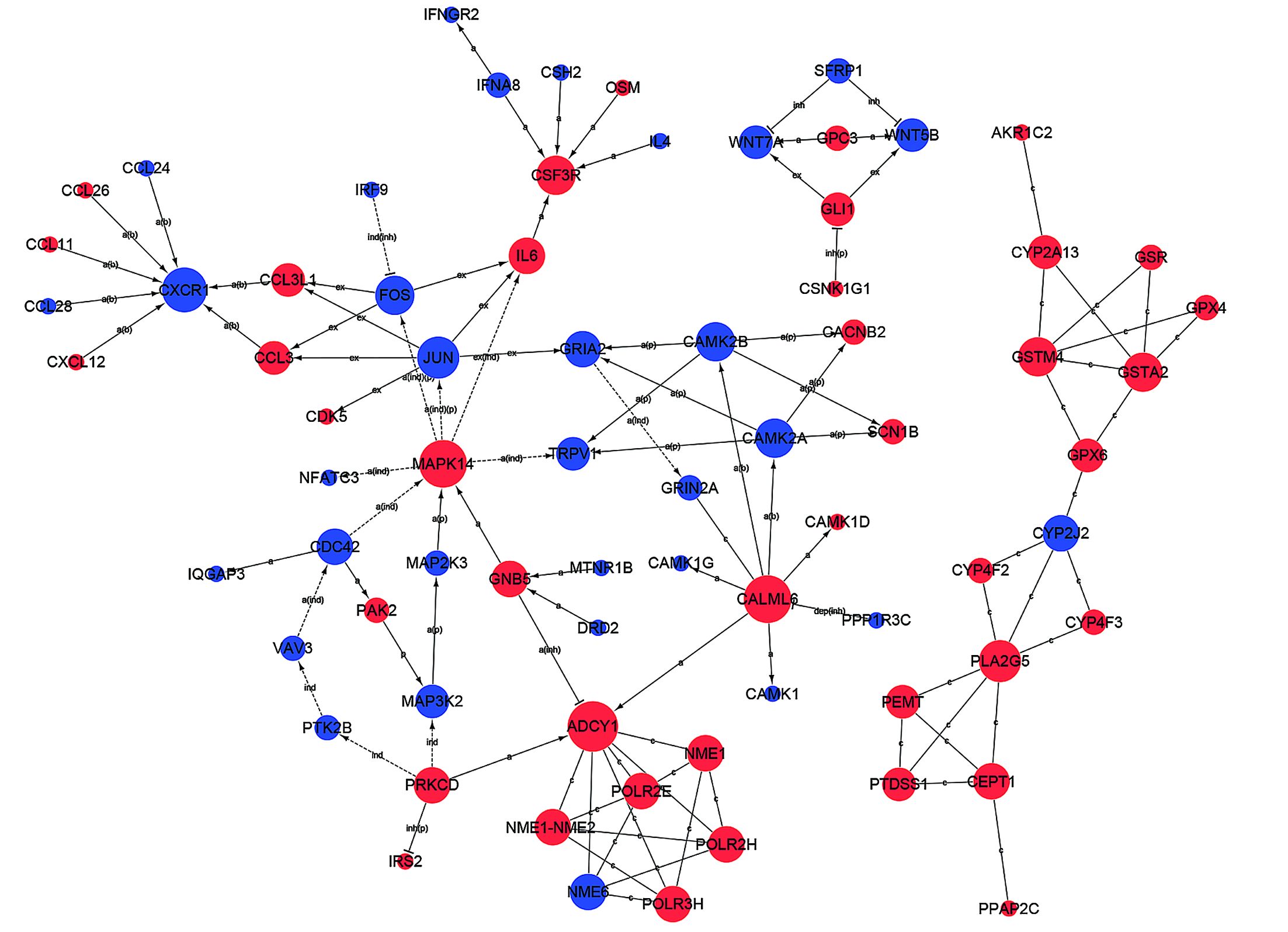
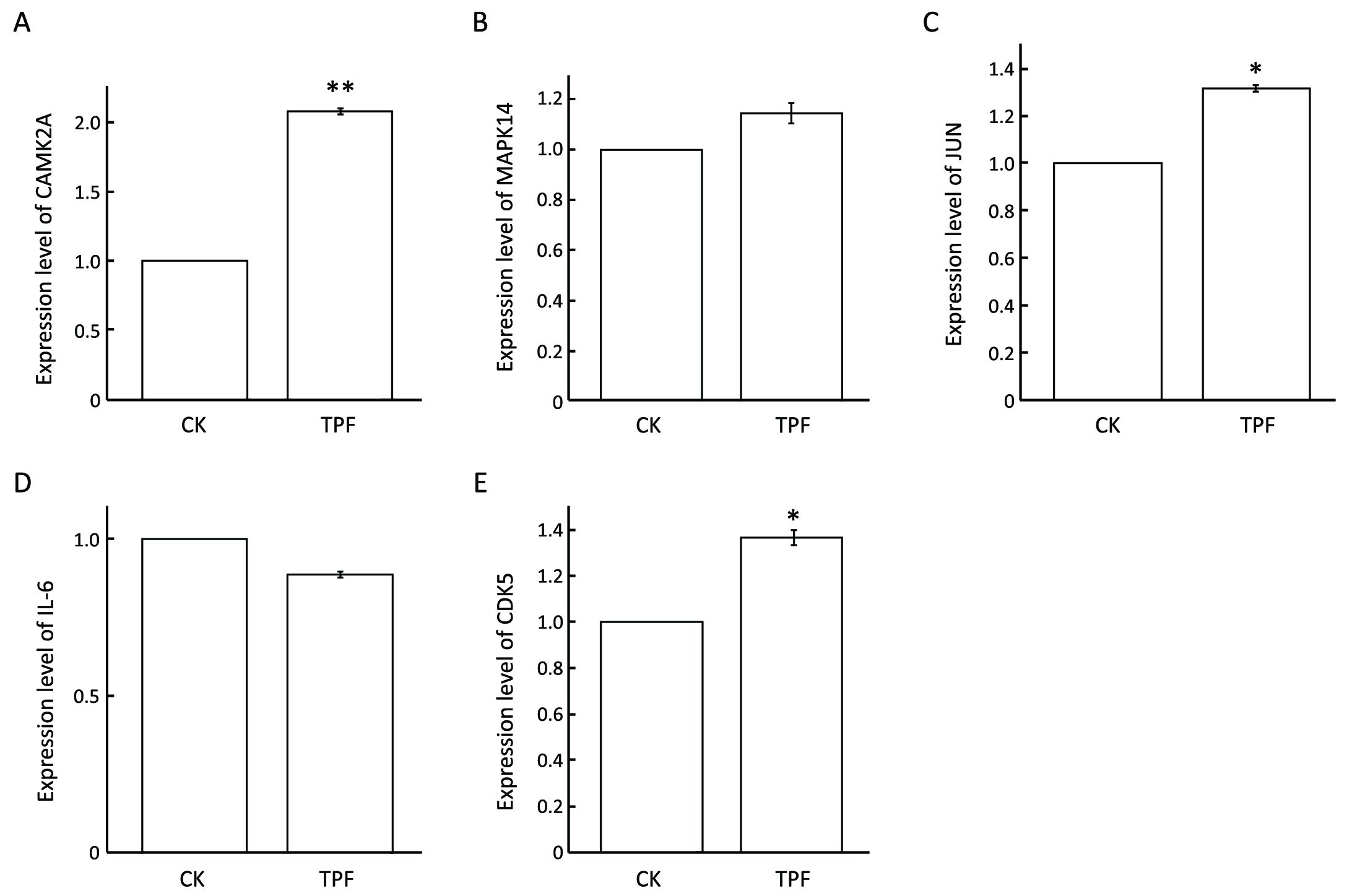
Objective To screen out a set of candidate genes which could help to determine whether patients with hypopharyngeal squamous cell carcinoma (HSCC) could benefit from docetaxel, cisplatin and 5-fluorouracil (TPF) induction chemotherapy. Methods Gene-expression profiles in 12 TPF-sensitive patients were compared to 9 resistant controls by microarray analysis. Subsequently, expression levels of potential biomarkers in chemosensitive cell line FaDu after TPF treatment were observed by quantitative real-time polymerase chain reaction (qRT-PCR). Results Through microarray analysis, 1,579 differentially expressed genes were identified, of which 815 were up-regulated in TPF chemotherapy-responsive tissues whereas 764 were down-regulated. Gene ontology (GO) analysis suggested these genes participating in physiological processes including transcription and its regulation, cellular signal transduction and metabolic process. Additionally, Kyoto Encyclopedia of Genes and Genomes (KEGG) database revealed that MAPK and Jat/STAT signaling pathways occupied important roles in TPF chemotherapeutic sensitivity. Moreover, in vitro cell culture experiments revealed the expression alternations of IL-6, MAPK14, JUN, CDK5 and CAMK2A exposed to TPF treatment by qRT-PCR, whilst providing an insight into the mechanism underlying TPF chemotherapeutic response in HSCC. Conclusions These results provided a battery of genes related to TPF chemotherapeutic sensitivity and might act as molecular targets in HSCC treatment. Moreover, these candidate biomarkers could contribute to HSCC individualized treatment.

2017, 29(3): 213-222.
doi: 10.21147/j.issn.1000-9604.2017.03.07
Abstract:
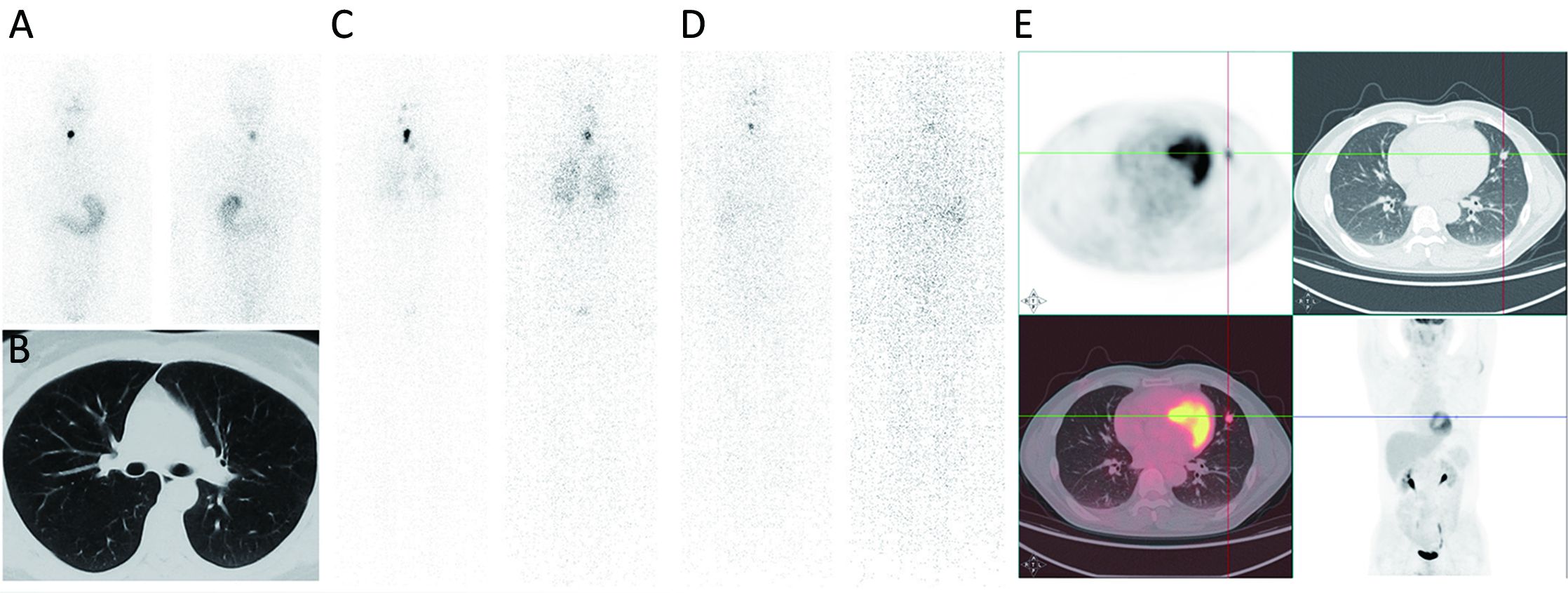
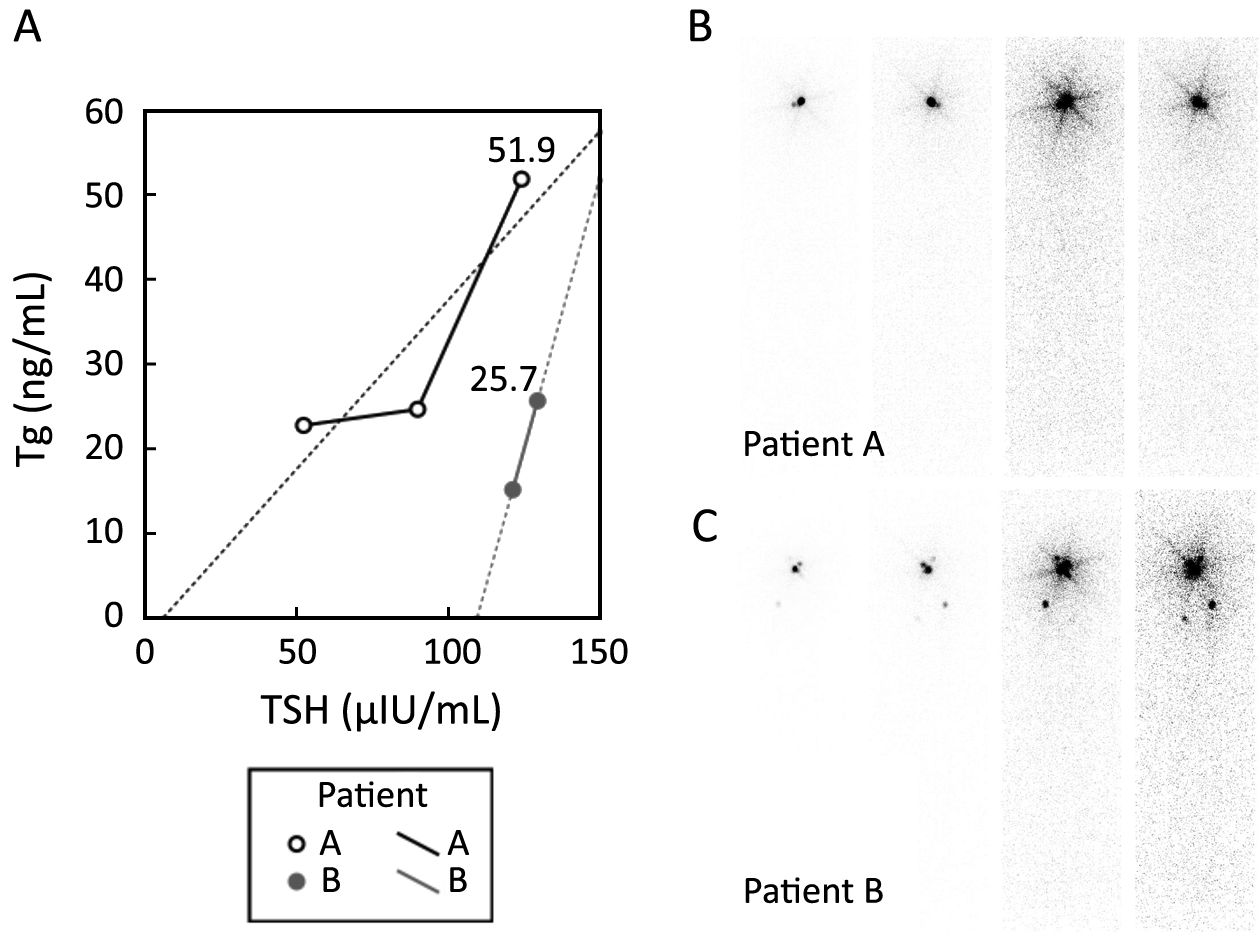
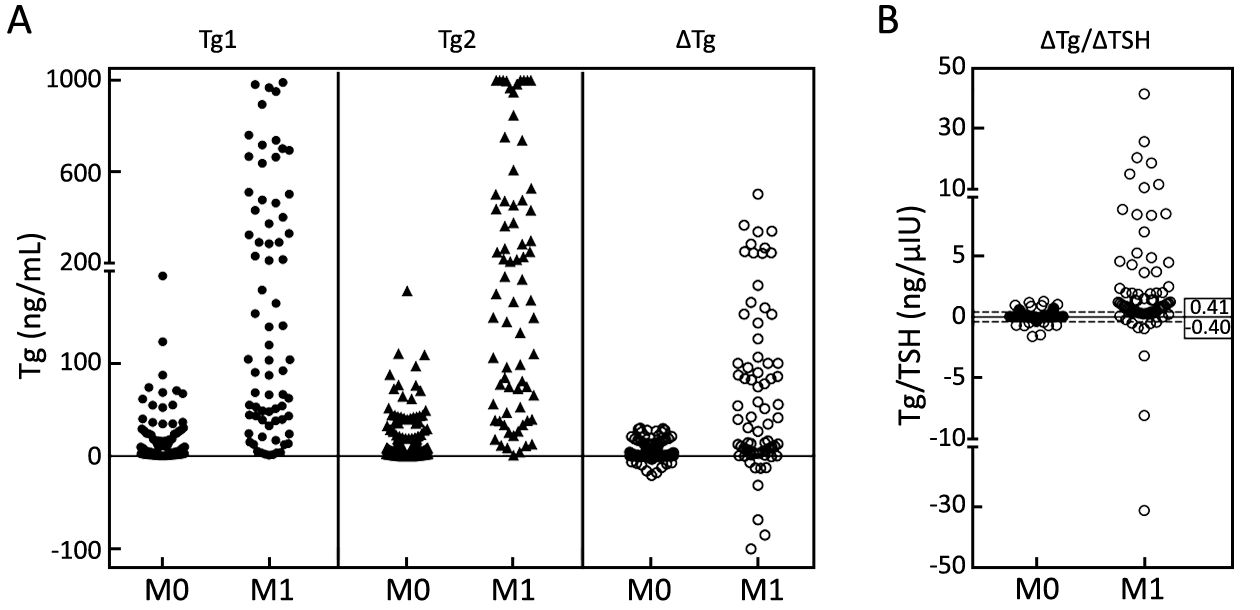
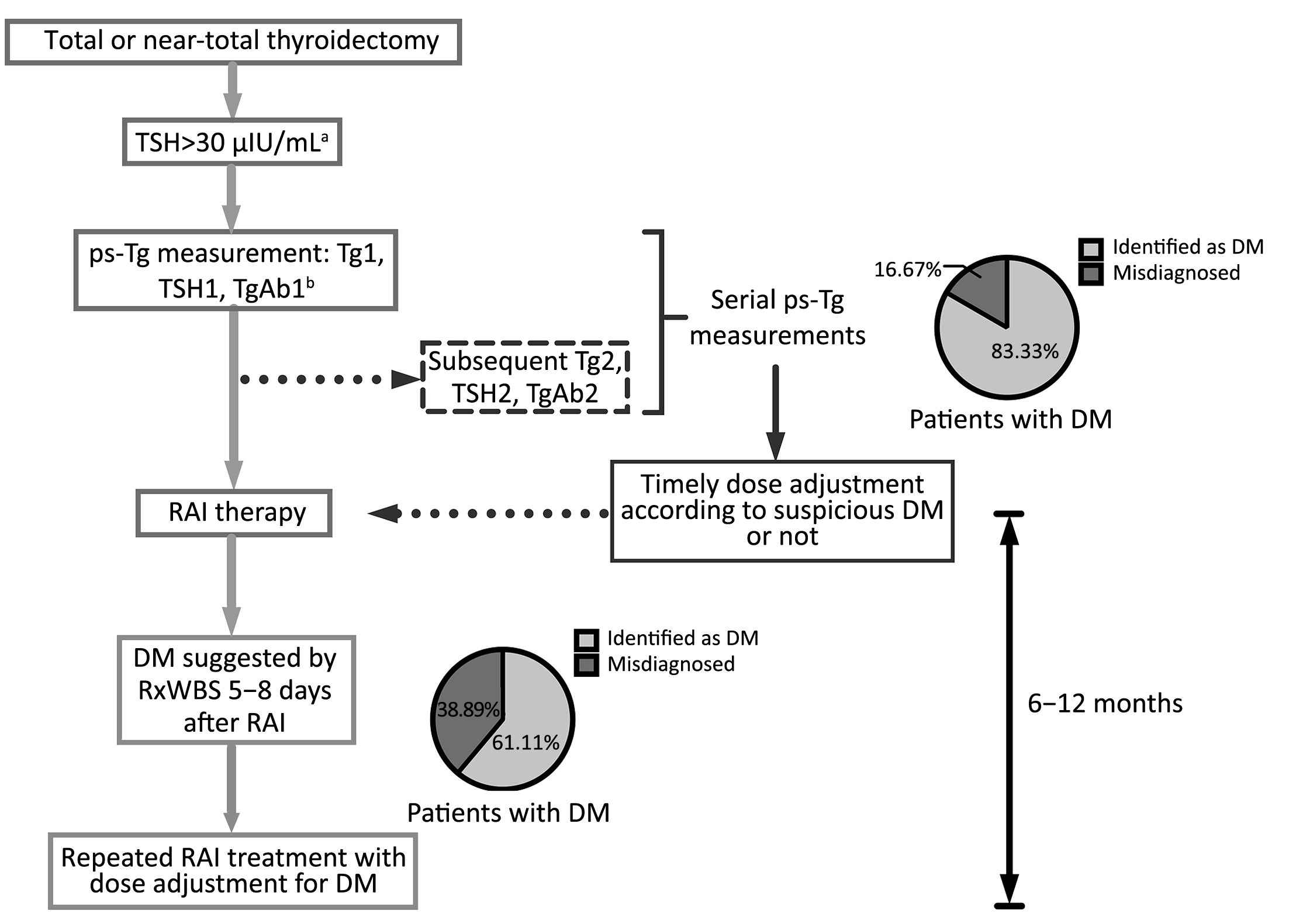
Objective Preablative stimulated thyroglobulin (ps-Tg) has the potential to be used in identifying distant metastatic differentiated thyroid carcinoma (DM-DTC), but its single level can be affected by remnant thyroid tissue and thyrotropin (TSH). The objective of this retrospective study was to evaluate the value of serial ps-Tg measurements in identifying DM-DTC specifically. Methods A total of 317 DTC patients with serial measurements of ps-Tg, TSH and anti-Tg antibody were divided into M1 (n=72) and M0 (n=245) according to the presence of distant metastasis (DM) or not. The initial ps-Tg measurement, with a corresponding TSH exceeding 30 μIU/mL, was marked as Tg1, and ps-Tg measured right before radioactive iodine (RAI) therapy was defined as Tg2, with a median interval of 8 days. ΔTg denotes Tg2–Tg1, and ΔTSH denotes TSH2–TSH1. Tg1, Tg2, ΔTg, and ΔTg/ΔTSH were tested for efficacy in identifying DM-DTC using receiver operating characteristic (ROC) curve analysis, and further compared with chest computed tomography (CT) and posttreatment whole-body RAI scan (RxWBS). Results Compared with single ps-Tg measurement (Tg1 or Tg2), both ΔTg and ΔTg/ΔTSH were more narrowly distributed around zero in the M0 group, which made their distribution in the M1 group more distinguished in a relatively dispersed way. ΔTg/ΔTSH manifested a higher accuracy (88.64%) and specificity (90.20%) in identifying DM-DTC than Tg1 or Tg2 measurements, with a much higher specificity than chest CT (90.20% vs. 66.00%) and a much higher sensitivity than RxWBS (83.33% vs. 61.11%). Conclusions Serial ps-Tg measurements even over as short an interval as 8 days hold incremental value in identifying DM-DTC. ΔTg/ΔTSH is a specific early biochemical marker for DM-DTC.
2017, 29(3): 223-230.
doi: 10.21147/j.issn.1000-9604.2017.03.08
Abstract:
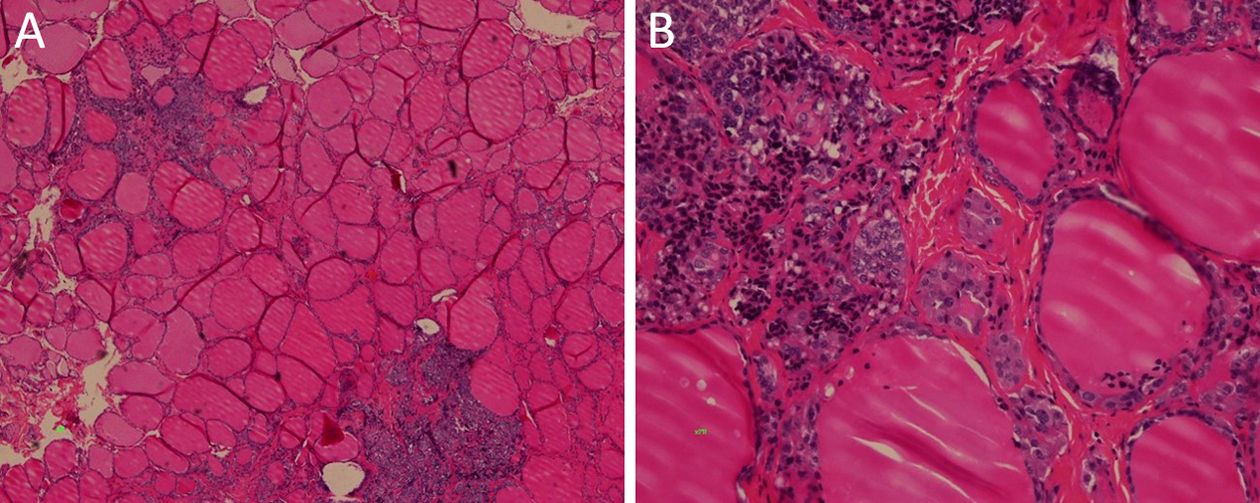
Objective The American Thyroid Association (ATA) proposed a new risk classification for hereditary medullary thyroid carcinoma (MTC) in 2015. This study aimed to assess whether the new guidelines are suitable for the Chinese population, and reported our experience on prophylactic thyroidectomy. Methods A total of 73 patients from 22 families were screened as rearranged during transfection (RET) mutation carriers from 2010 to 2016 in Cancer Hospital, Chinese Academy of Medical Science; the medical history for each patient was collected. Based on the initial treatment, we identified the risk factors for poor prognosis by univariate and multivariate logistic regression. Then, 4 RET mutation carriers were enrolled for prophylactic thyroidectomy, and their pathological data and follow-up outcomes were recorded. Results In univariate and multivariate logistic regression analyses, age at initial surgery and risk classification were significant risk factors for stage III/IV hereditary MTC at initial diagnosis. The likelihood was increased by 11.6% per year of age at initial surgery [95% confidence interval (95% CI), 1.040–1.198; P=0.002). It was 7.888 times more likely to have III/IV stage disease for ATA highest risk patients, compared to ATA moderate risk individuals (95% CI, 1.607–38.717; P=0.003). Postoperative pathological results showed all 4 multiple endocrine neoplasia type 2A (MEN2A) patients had C-cell hyperplasia (CCH); multifocal malignancies were detected in 3 of them. All 4 patients were cured biochemically, and none developed permanent hypoparathyroidism. Conclusions In Chinese individuals, hereditary MTC aggressiveness is in line with the new ATA risk classification. Germline RET gene mutation carriers should undergo prophylactic thyroidectomy according to basal serum calcitonin levels.
2017, 29(3): 253-262.
doi: 10.21147/j.issn.1000-9604.2017.03.11
Abstract:
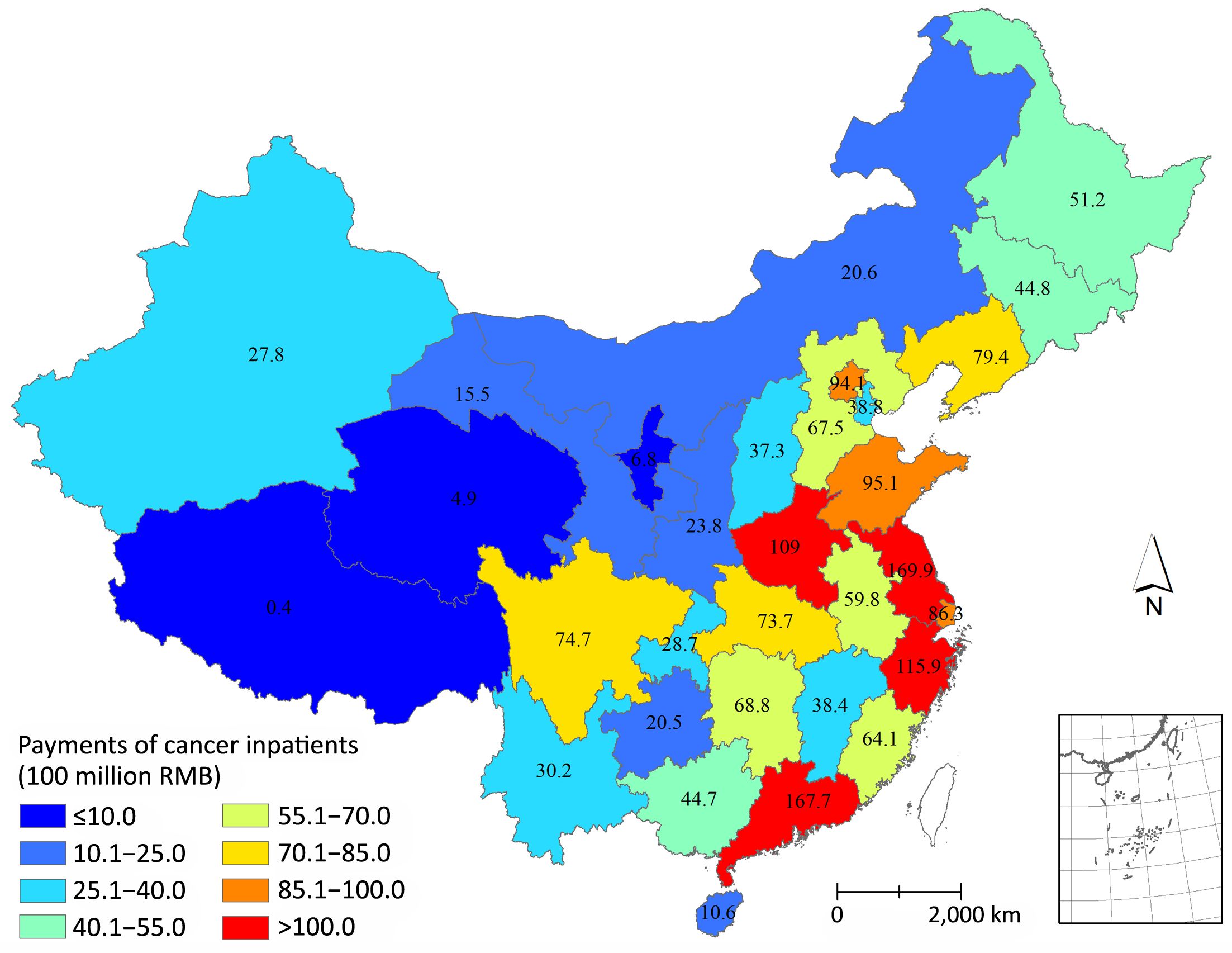
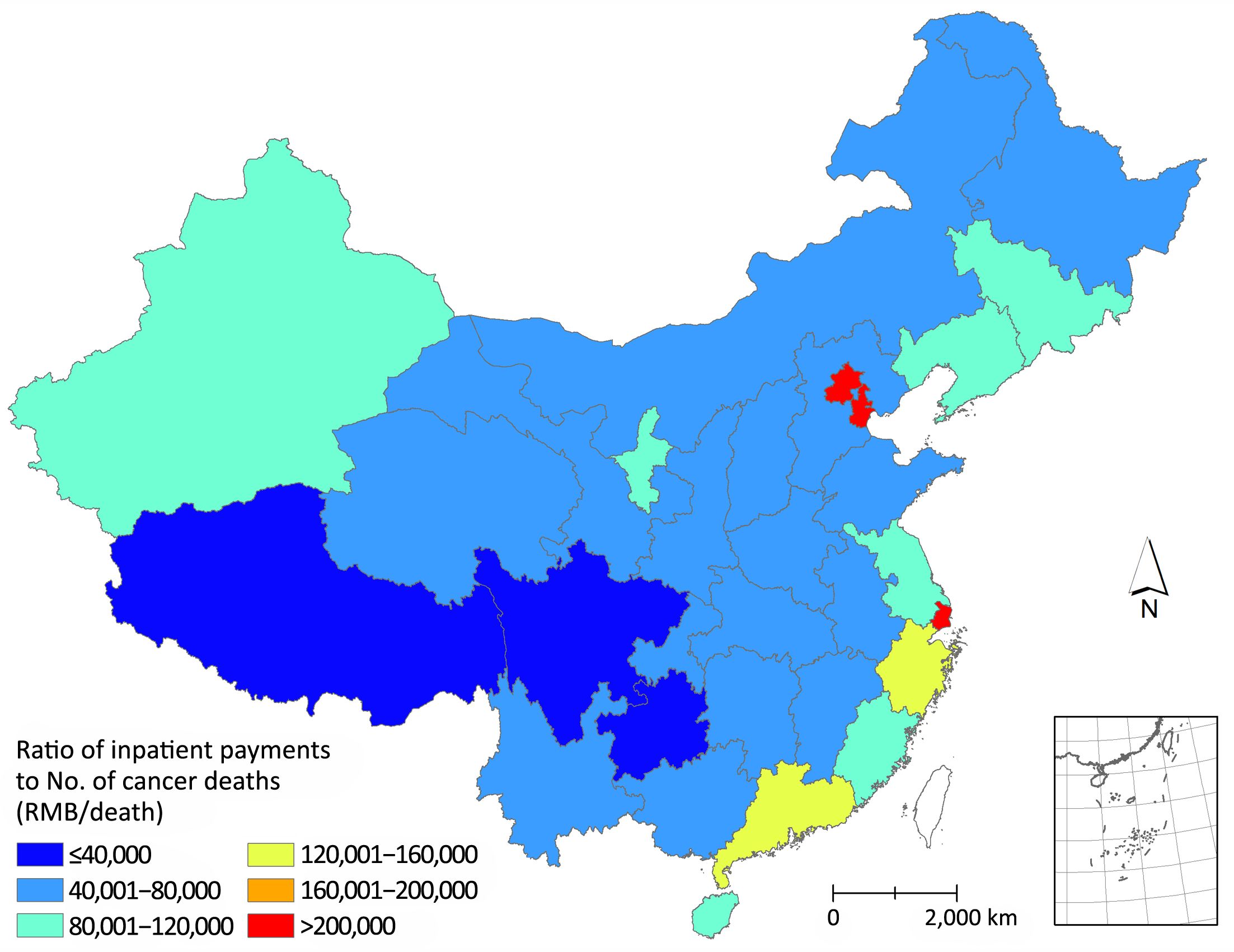
Objective A solid understanding of levels and trends of spending on cancer is important to evaluate whether our healthcare resources were wisely spent and to prioritize future resources for cancer treatment and prevention. However, studies on economic burden of cancers in China are scant and the results are inconsistent. Methods The Chinese hospital information database and nearly 350 million inpatient medical record data were used. As the ratios of cancer inpatient payments to total inpatient payments were mainly influenced by the grades and sites of hospitals, the estimates of payments of cancer inpatients in this study were stratified by hospital grades and provinces. Only the payments of cancer inpatients happened in grade 2, grade 3 and specialized cancer hospitals were included in the analyses. The total medical payments of cancers in China were estimated based on the ratios of outpatient payments to inpatient payments in specialized cancer hospitals. Results From 2011 to 2015, the payments of cancer inpatients in China have increased by 84.1% and the total inpatient payments reached 177.1 billion RMB in 2015, accounting for 4.3% of the total health expenditure in China. Based on the ratio of outpatient payments to inpatient payments, the total payments on cancer treatments in China were estimated to be 221.4 billion RMB in 2015. Among different cancer types, the highest payments were the treatment of trachea, bronchus and lung cancer. The major cancer inpatient payments (67.1% in 2015) spent in grade 3 general hospitals and this ratio increased continually from 2011 to 2015. The expenditure of cancer treatments also varies by region with the major expenditure in the eastern region of China. Conclusions This study estimated the total payments of cancer treatments in China and analyzed how the money was spent on cancer treatments in the recent 5 years, which would provide information for decision makings on the allocation of resources to service provisioning, prevention strategies, research funding, and assessing whether the economic burden of cancer is affordable to the governments.
2017, 29(3): 263-271.
doi: 10.21147/j.issn.1000-9604.2017.03.12
Abstract:
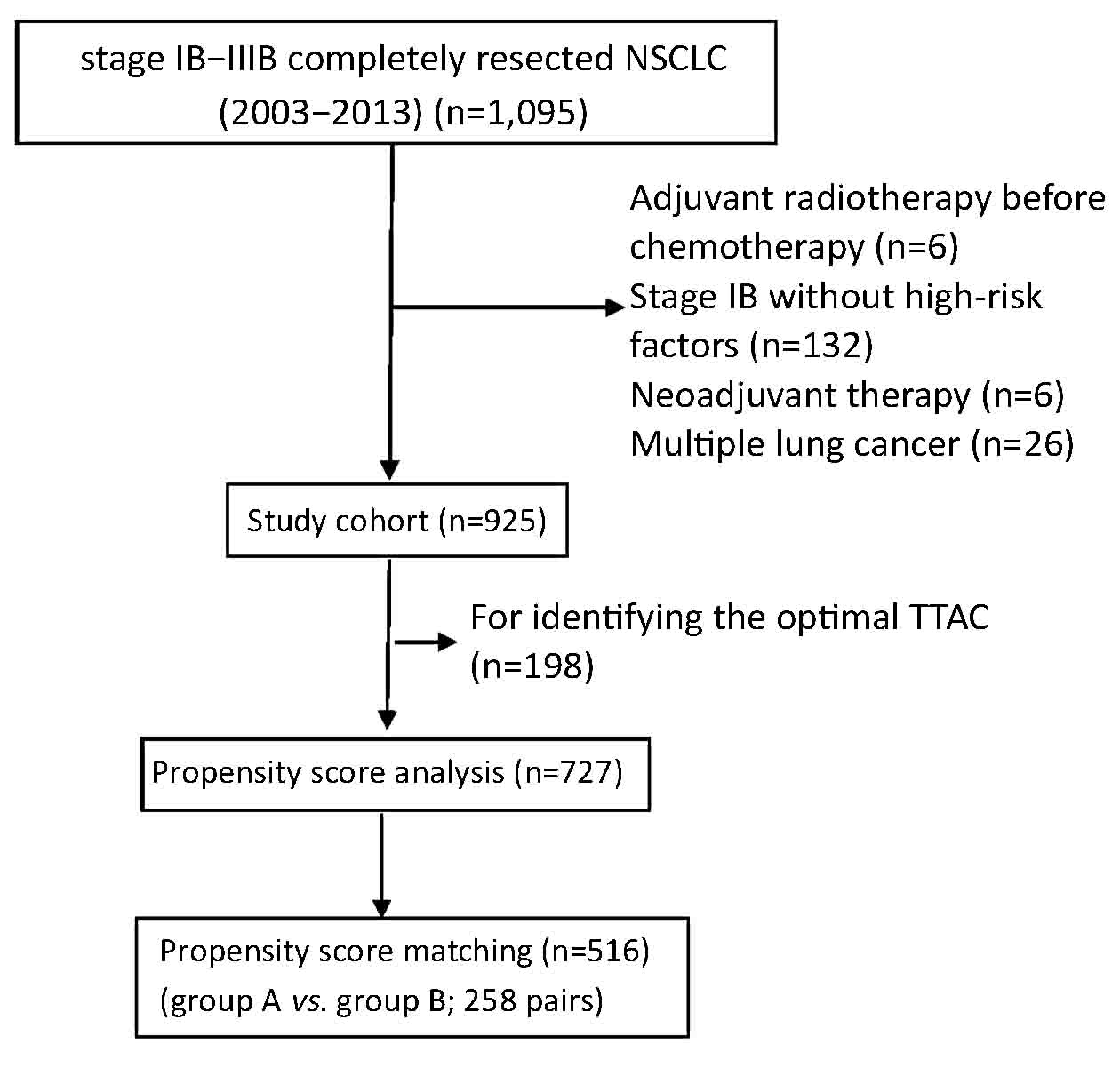
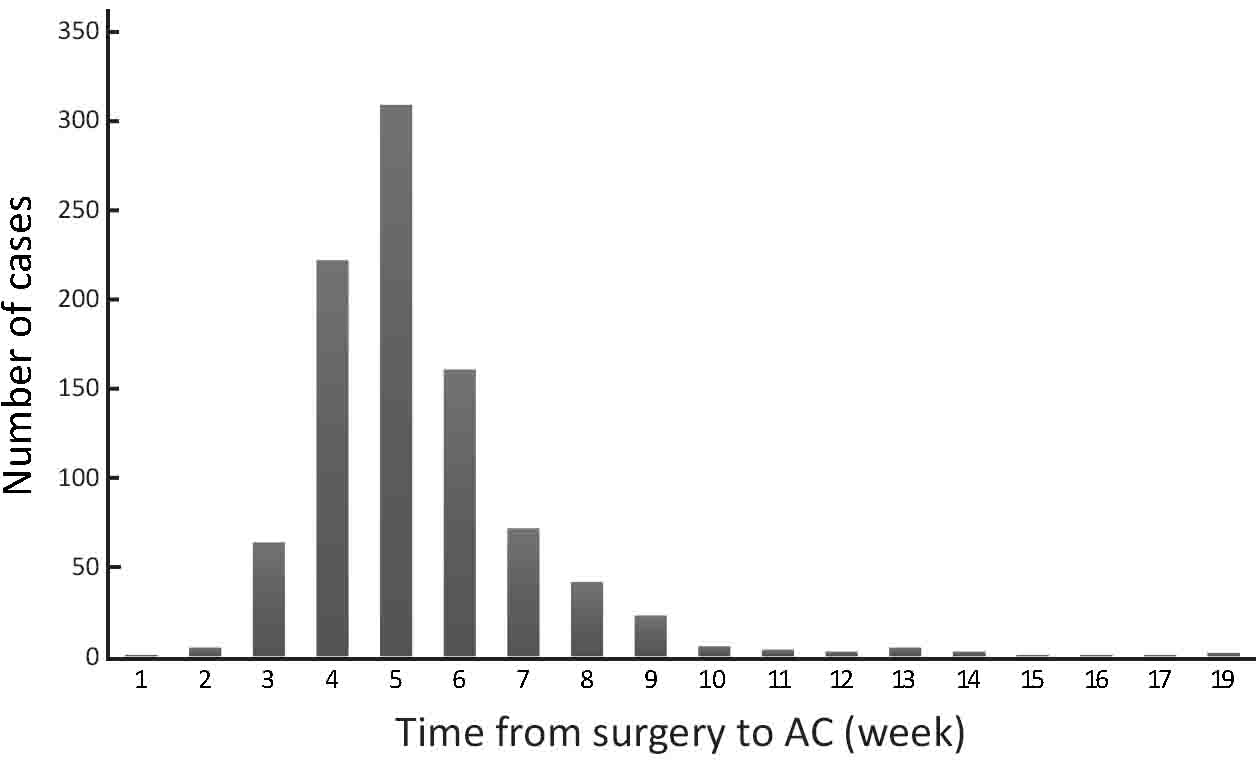
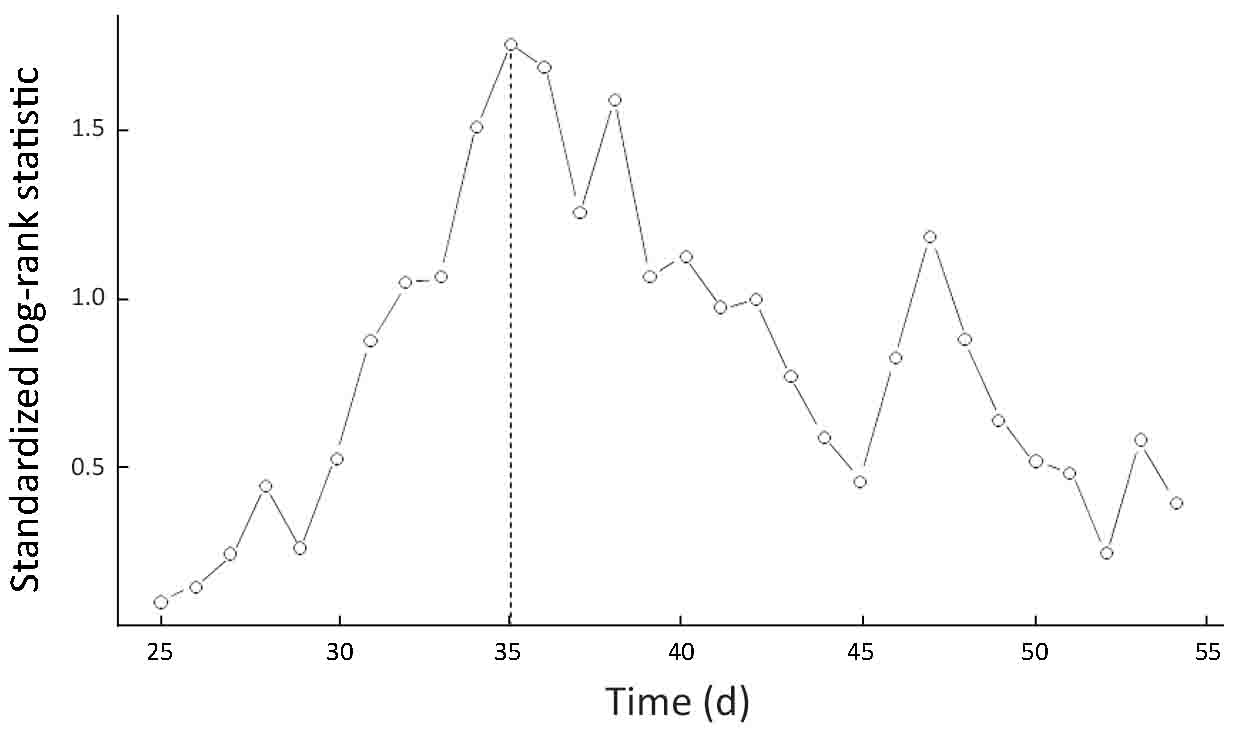
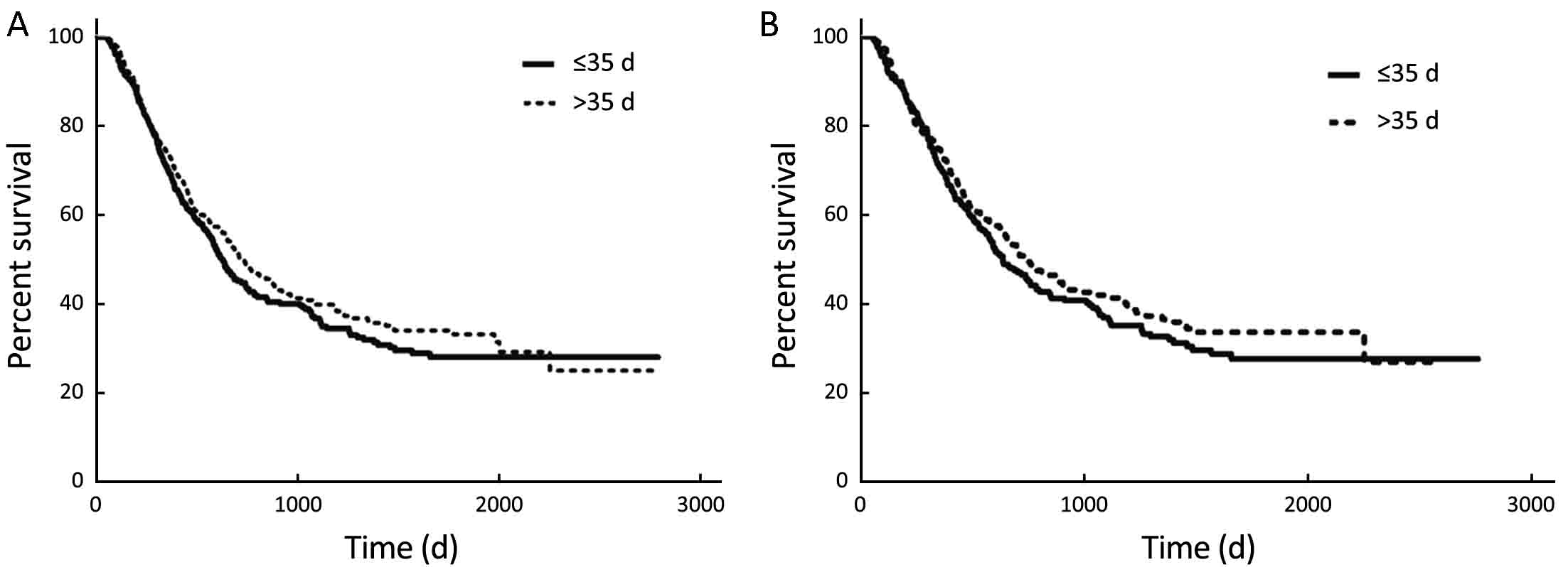
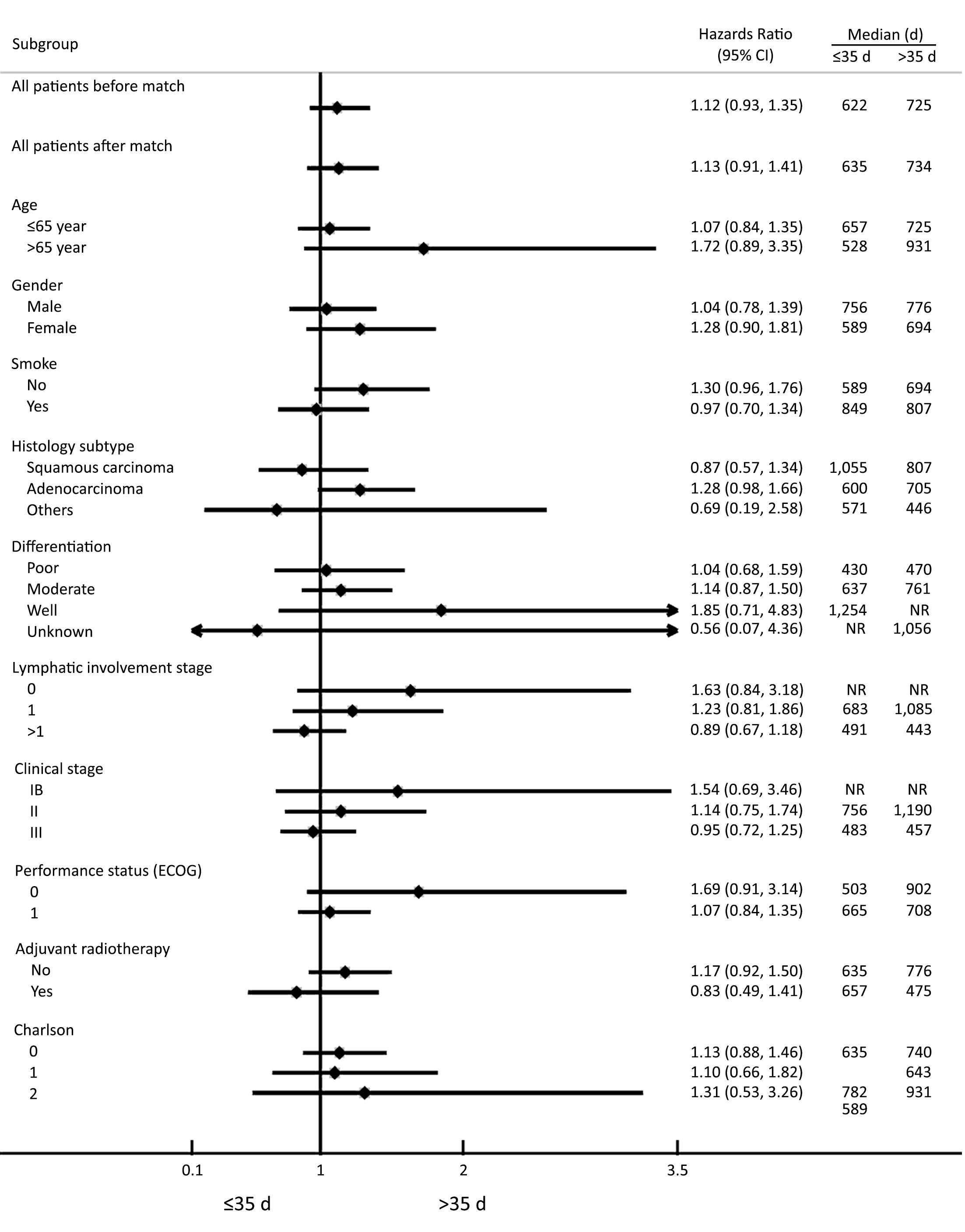
Objective Adjuvant chemotherapy (AC) after curative resection is known to improve the survival of patients with non-small cell lung cancer (NSCLC); however, few studies have reported the correlation between the time to initiation of AC (TTAC) and survival in NSCLC patients. Methods The clinical data of 925 NSCLC patients who received curative resection and post-operative AC at the Cancer Hospital of Chinese Academy of Medical Sciences between 2003 and 2013 were retrospectively analyzed. TTAC was measured from the date of surgery to the initiation of AC. Disease-free survival (DFS) was defined as the duration from surgery to the time of tumor recurrence or last follow-up evaluation. The optimal cut-off value of TTAC was determined by maximally selected log-rank statistics. The DFS curve was estimated using the Kaplan-Meier method, and the Cox proportional hazards regression model was used to identify risk factors independently associated with DFS. Propensity score matching (PSM) was performed for survival analysis using the match data. Results The optimal discriminating cut-off value of TTAC was set at d 35 after curative resection based on which the patients were assigned into two groups: group A (≤35 d) and group B (>35 d). There was no significant difference in the DFS between the two groups (P=0.246), indicating that the TTAC is not an independent prognostic factor for DFS. A further comparison continued to show no significant difference in the DFS among 258 PSM pairs (P=0.283). Conclusions There was no significant correlation between the TTAC and DFS in NSCLC patients. Studies with larger samples are needed to further verify this conclusion.
2017, 29(3): 272-280.
doi: 10.21147/j.issn.1000-9604.2017.03.13
Abstract:
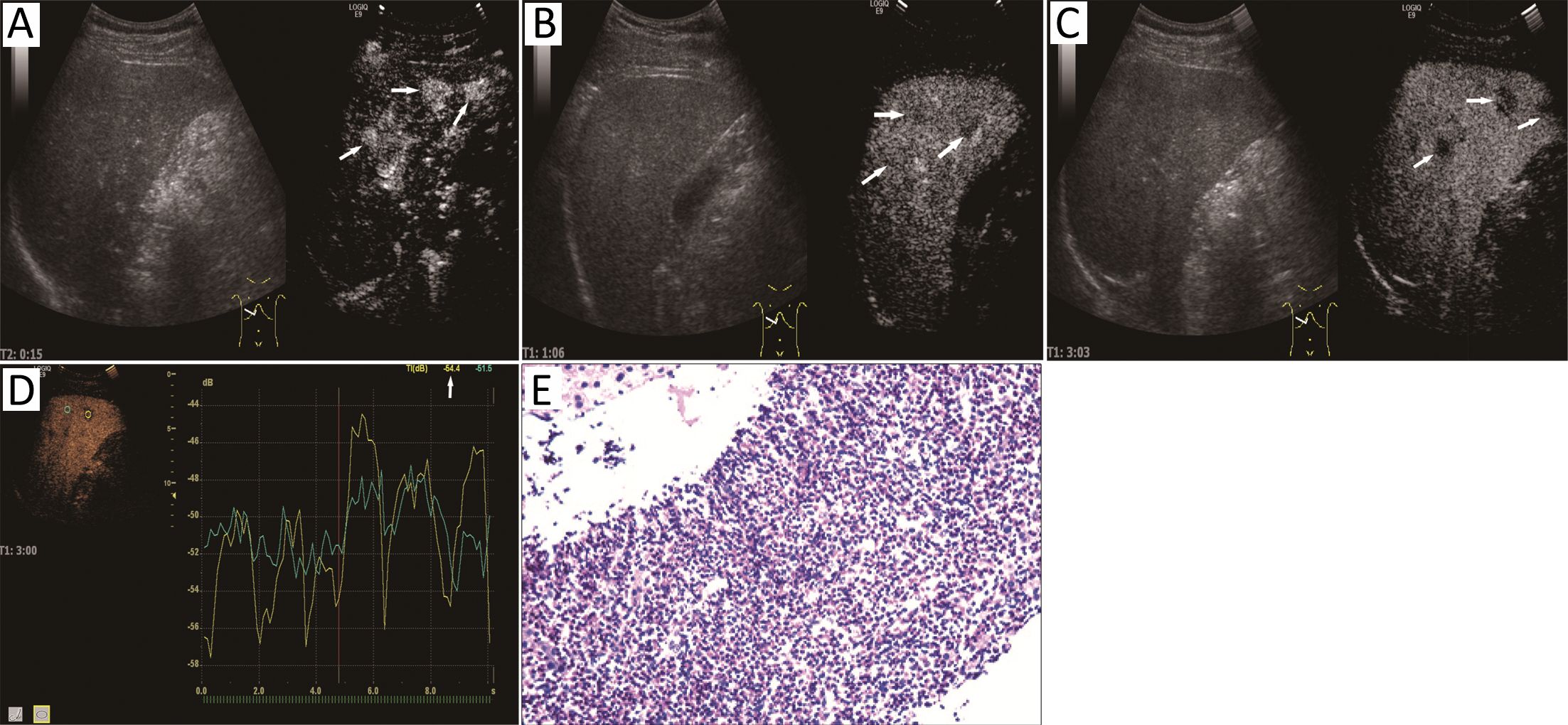
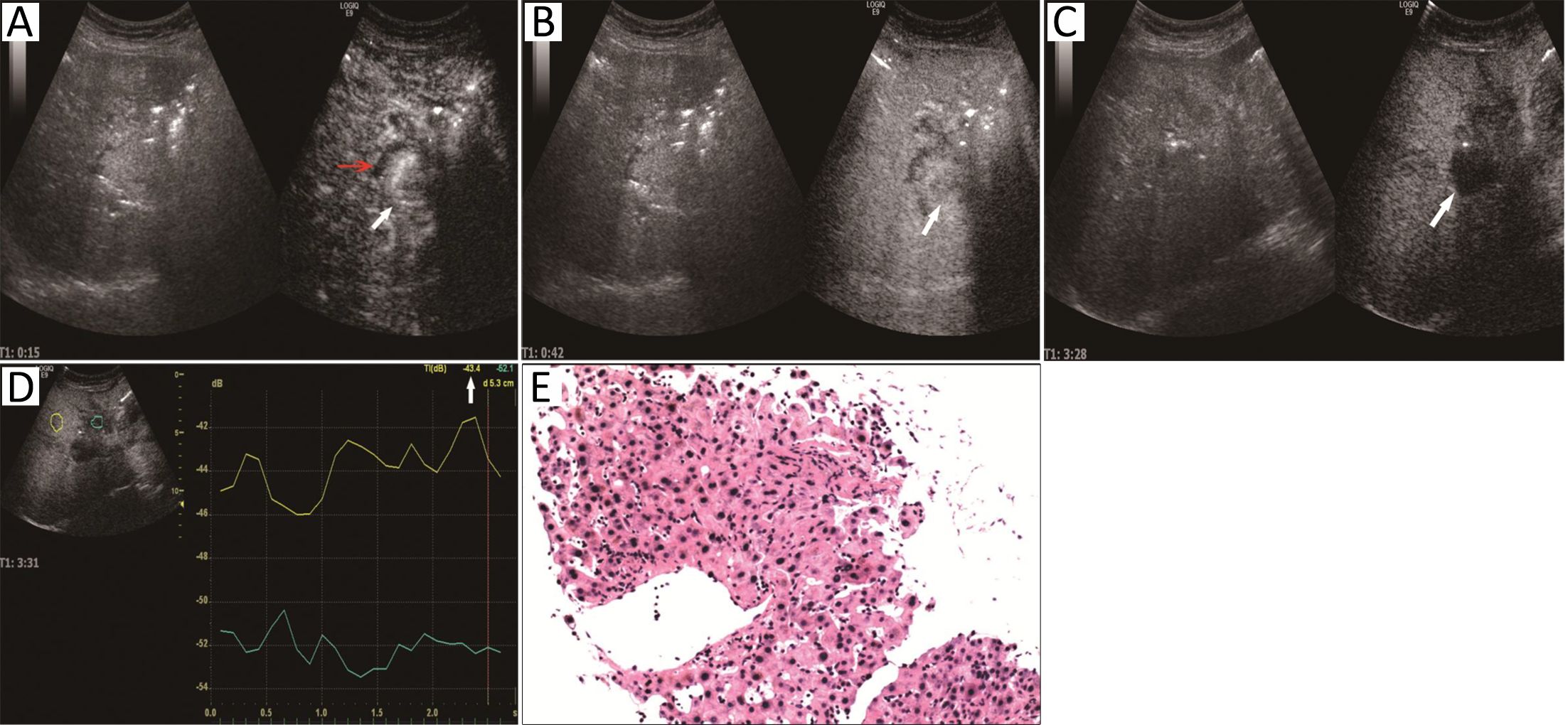
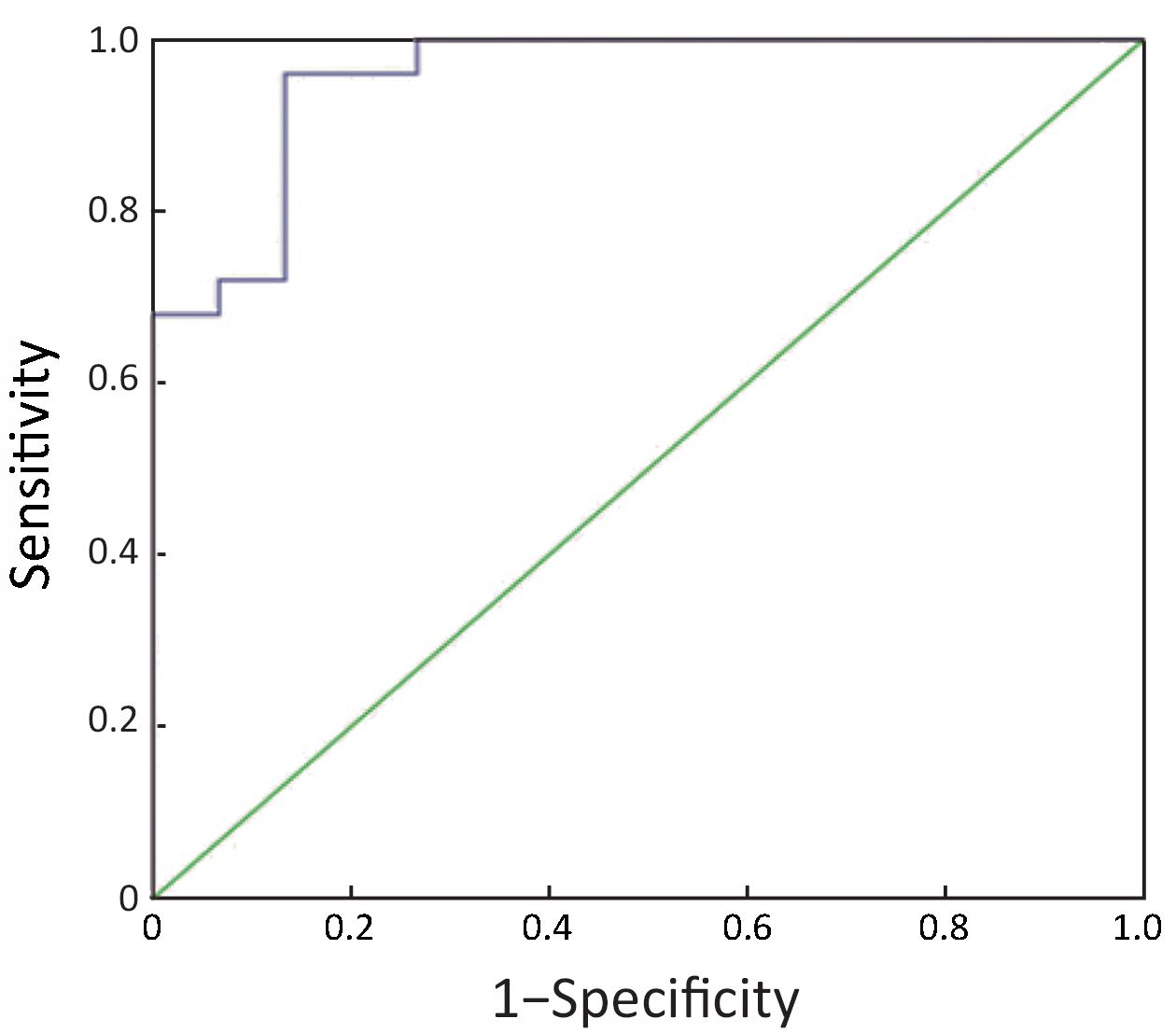
Objective To investigate differential diagnosis between intrahepatic cholangiocarcinoma (ICC) and arterial phase enhanced hepatic inflammatory lesions in patients without liver cirrhosis using contrast-enhanced ultrasound (CEUS). Methods ICC and hepatic inflammatory lesions cases with CEUS and pathological diagnosis between Sep 2013 and Oct 2016 were investigated retrospectively. Imaging features of conventional ultrasound and CEUS were analyzed. The parameters of time intensity curve (TIC), including the arrival time, peak intensity (PI) in the lesions, the starting time for washout, and the intensity difference at 3 min (ΔI3) after contrast agent infection between the lesion and the liver parenchyma, were compared between ICC and hepatic inflammatory lesions. Results Twenty-five ICC and fifteen inflammatory patients were included in this study. Seventeen ICC (68.0%) and two inflammatory cases (13.3%) showed bile duct dilatation on conventional ultrasound. Using CEUS, three ICC cases (12.0%) were misdiagnosed as inflammatory lesions and three inflammatory lesions (20.0%) as ICC; two ICC (8.0%) and one inflammatory case (6.7%) could not be made definite diagnosis. Washout started at 34.5±3.5 s and 61.5±12.9 s for ICC and inflammatory lesions respectively (P<0.001). The intensity difference between lesion and liver parenchyma at 3 min after contrast agent injection was 10.8±3.1 dB in ICC and 4.2±2.3 dB in inflammatory group (P<0.001). The sensitivity and specificity differentiating ICC and inflammatory lesions were 76% and 87% if the cut-off value of the intensity difference was 7.7 dB. Conclusions Combined with TIC analysis, and particularly with the characteristic of the early-starting and obvious washout in ICC, CEUS can be useful in differential diagnosis between hepatic inflammatory lesions and ICC.

2017, 29(3): 231-236.
doi: 10.21147/j.issn.1000-9604.2017.03.09
Abstract:
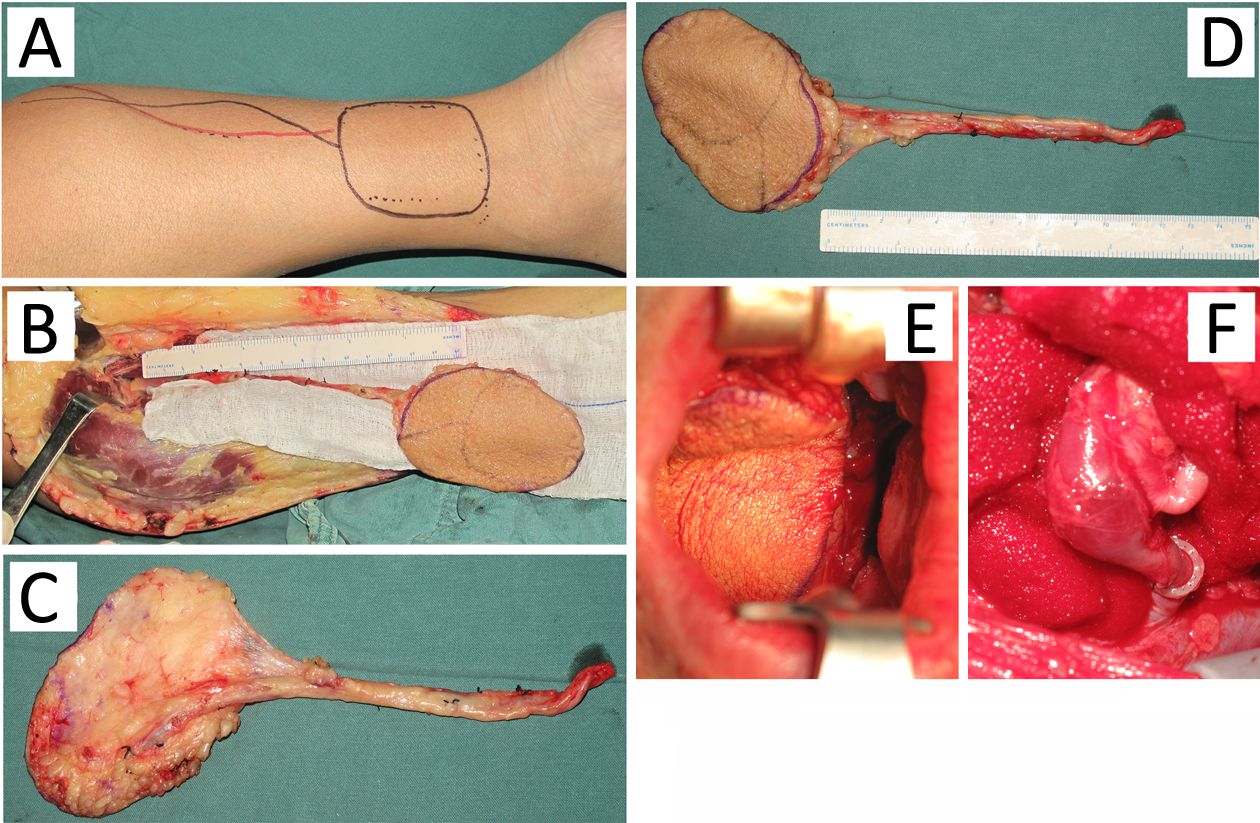
Tumor resection causes damage in the head and neck which creates problems in swallowing, chewing, articulation, and vision, all of which seriously affect patients’ quality of life. In this work, we evaluated the application of a free medial tibial flap in reconstruction of head and neck defects after tumor resection. We discussed the anatomy, surgical technique, and the advantages and disadvantages of the flap. We found several benefits for the flap, such as, it is especially effective for the defects that require thin-layer epithelium to cover or the separated soft tissue defect; a two-team approach can be used because the donor site is far away from the head and neck; and the flap is easy to integrate because of the subcutaneous fat layer of the free medial tibial flap is thin and the flap is soft. Thus, the medial tibial flap could replace the forearm flap for certain applications.
Tumor resection causes damage in the head and neck which creates problems in swallowing, chewing, articulation, and vision, all of which seriously affect patients’ quality of life. In this work, we evaluated the application of a free medial tibial flap in reconstruction of head and neck defects after tumor resection. We discussed the anatomy, surgical technique, and the advantages and disadvantages of the flap. We found several benefits for the flap, such as, it is especially effective for the defects that require thin-layer epithelium to cover or the separated soft tissue defect; a two-team approach can be used because the donor site is far away from the head and neck; and the flap is easy to integrate because of the subcutaneous fat layer of the free medial tibial flap is thin and the flap is soft. Thus, the medial tibial flap could replace the forearm flap for certain applications.

2017, 29(3): 237-252.
doi: 10.21147/j.issn.1000-9604.2017.03.10
Abstract:
Breast cancer has been shown to live in the tumor microenvironment, which consists of not only breast cancer cells themselves but also a significant amount of pathophysiologically altered surrounding stroma and cells. Diverse components of the breast cancer microenvironment, such as suppressive immune cells, re-programmed fibroblast cells, altered extracellular matrix (ECM) and certain soluble factors, synergistically impede an effective anti-tumor response and promote breast cancer progression and metastasis. Among these components, stromal cells in the breast cancer microenvironment are characterized by molecular alterations and aberrant signaling pathways, whereas the ECM features biochemical and biomechanical changes. However, triple-negative breast cancer (TNBC), the most aggressive subtype of this disease that lacks effective therapies available for other subtypes, is considered to feature a unique microenvironment distinct from that of other subtypes, especially compared to Luminal A subtype. Because these changes are now considered to significantly impact breast cancer development and progression, these unique alterations may serve as promising prognostic factors of clinical outcome or potential therapeutic targets for the treatment of TNBC. In this review, we focus on the composition of the TNBC microenvironment, concomitant distinct biological alteration, specific interplay between various cell types and TNBC cells, and the prognostic implications of these findings.
Breast cancer has been shown to live in the tumor microenvironment, which consists of not only breast cancer cells themselves but also a significant amount of pathophysiologically altered surrounding stroma and cells. Diverse components of the breast cancer microenvironment, such as suppressive immune cells, re-programmed fibroblast cells, altered extracellular matrix (ECM) and certain soluble factors, synergistically impede an effective anti-tumor response and promote breast cancer progression and metastasis. Among these components, stromal cells in the breast cancer microenvironment are characterized by molecular alterations and aberrant signaling pathways, whereas the ECM features biochemical and biomechanical changes. However, triple-negative breast cancer (TNBC), the most aggressive subtype of this disease that lacks effective therapies available for other subtypes, is considered to feature a unique microenvironment distinct from that of other subtypes, especially compared to Luminal A subtype. Because these changes are now considered to significantly impact breast cancer development and progression, these unique alterations may serve as promising prognostic factors of clinical outcome or potential therapeutic targets for the treatment of TNBC. In this review, we focus on the composition of the TNBC microenvironment, concomitant distinct biological alteration, specific interplay between various cell types and TNBC cells, and the prognostic implications of these findings.


