2017 Vol.29(4)
Display Mode: |
2017, 29(4): 281-293.
doi: 10.21147/j.issn.1000-9604.2017.04.01
 Abstract
Abstract FullText HTML
FullText HTML PDF 565KB
PDF 565KB
Abstract:
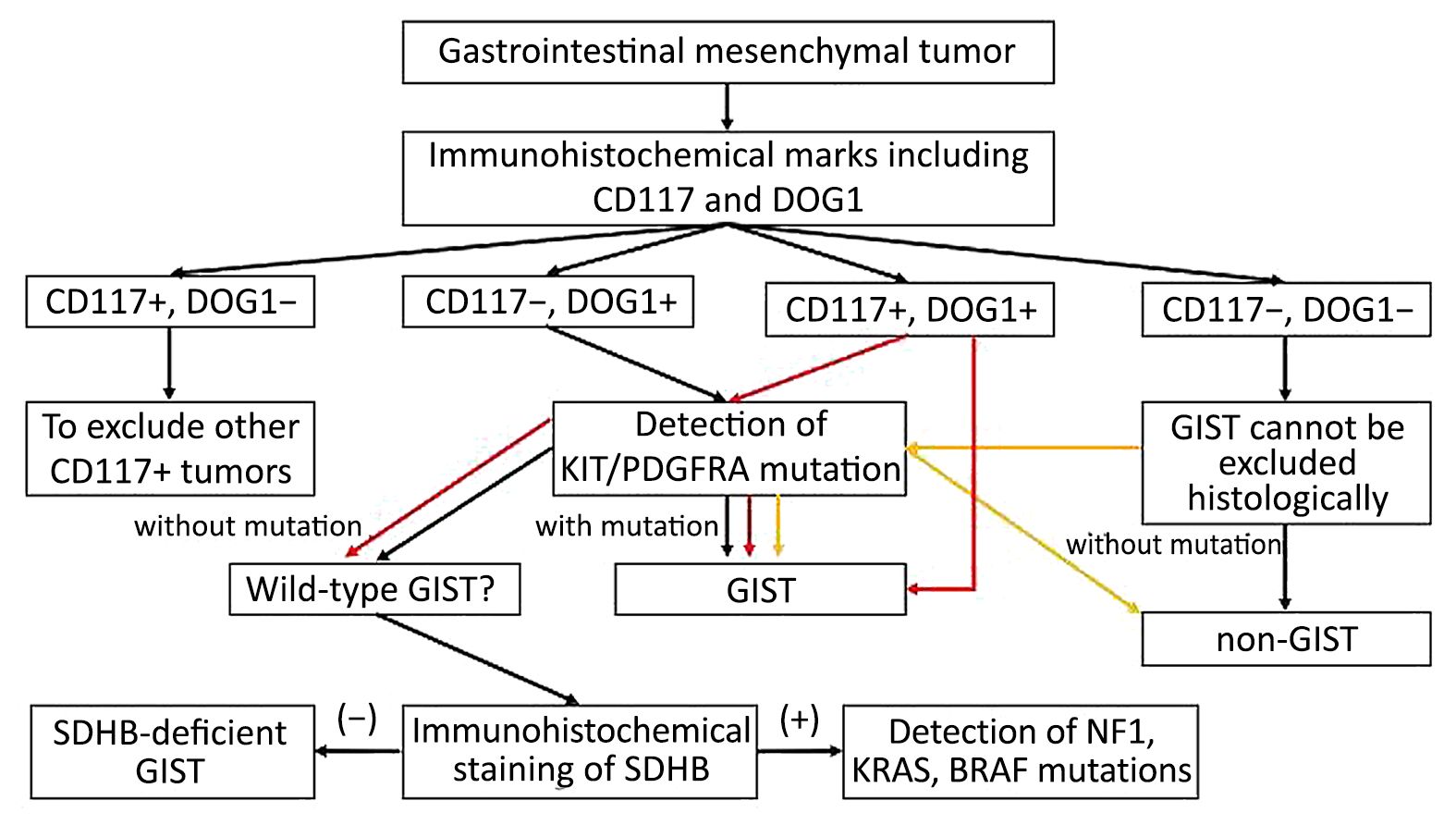
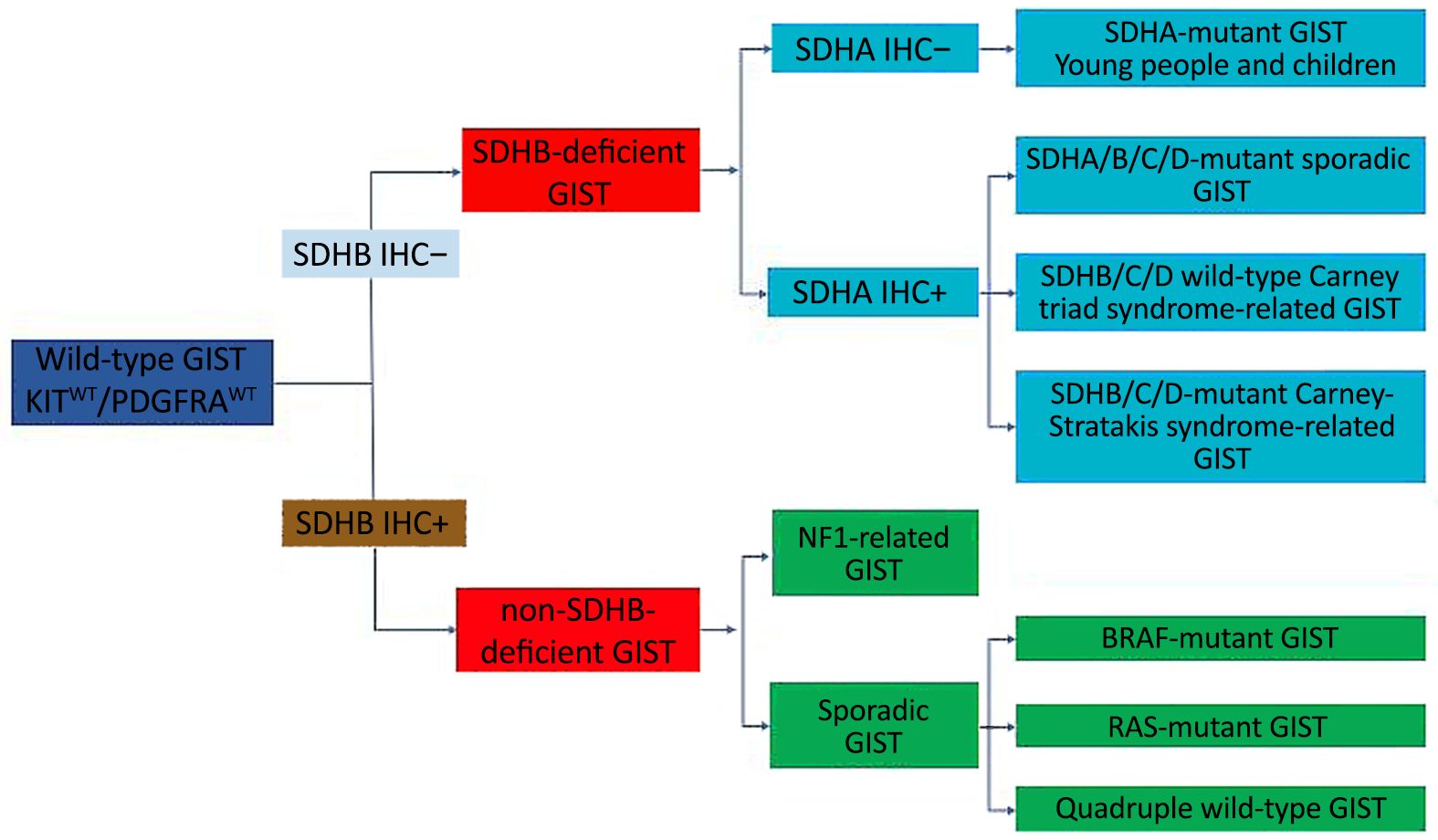
In order to further promote the standardization of diagnosis and treatment of gastrointestinal stromal tumor (GIST) in China, the members of Chinese Society of Clinical Oncology (CSCO) Expert Committee on GIST thoroughly discussed the key contents of the consensus guidelines, and voted on the controversial issue. In final, the Chinese consensus guidelines for the diagnosis and management of GIST (2017 edition) was formed on the basis of 2013 edition consensus guidelines, which is hereby announced. The consensus included the pathological diagnosis, recurrence risk classification evaluation, targeted agent therapy, surgery and principles of surveillance of GIST.
In order to further promote the standardization of diagnosis and treatment of gastrointestinal stromal tumor (GIST) in China, the members of Chinese Society of Clinical Oncology (CSCO) Expert Committee on GIST thoroughly discussed the key contents of the consensus guidelines, and voted on the controversial issue. In final, the Chinese consensus guidelines for the diagnosis and management of GIST (2017 edition) was formed on the basis of 2013 edition consensus guidelines, which is hereby announced. The consensus included the pathological diagnosis, recurrence risk classification evaluation, targeted agent therapy, surgery and principles of surveillance of GIST.
2017, 29(4): 294-302.
doi: 10.21147/j.issn.1000-9604.2017.04.02
Abstract:
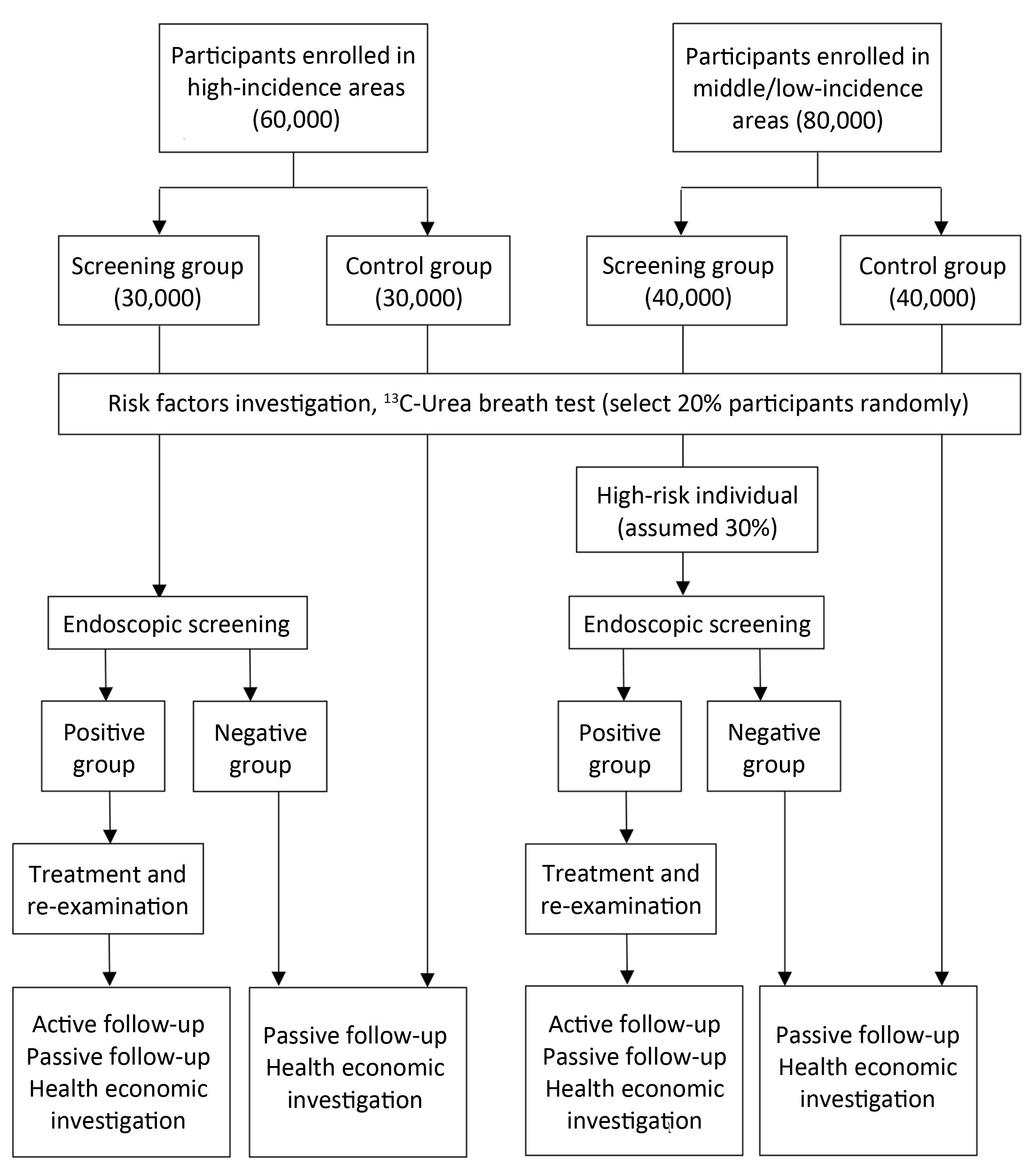
Objective To evaluate the efficacy and feasibility of screening procedure for upper gastrointestinal cancer in both high-risk and non-high-risk areas in China. Setting Seven cities/counties, representing three economical-geographical regions (Eastern, Central and Western) in China, were selected as screening centers: three in high-risk areas and four in non-high-risk areas. Participants Villages/communities in these seven centers regarded as clusters were randomly assigned to either intervention group (screening by endoscopic examination) or control group (with normal community care) in a 1:1 ratio stratified by each center. Eligible participants are local residents aged 40–69 years in the selected villages/communities with no history of cancer or endoscopic examination in the latest 3 years who are mentally and physically competent. Those who are not willing to take endoscopic examination or are unwilling to sign the consent form are excluded from the study. Totally 140,000 participants will be enrolled. Interventions In high-risk areas of upper gastrointestinal cancer, all subjects in screening group will be screened by endoscopy. In non-high-risk areas, 30% of the subjects in screening group, identified through a survey, will be screened by endoscopy. Primary and secondary outcome measures The primary outcome is the mortality caused by upper gastrointestinal cancer. The secondary outcomes include detection rate, incidence rate, survival rate, and clinical stage distribution. Additional data on quality of life and cost-effectiveness will also be collected to answer important questions regarding screening effects. Conclusions Screening strategy evaluated in those areas with positive findings may be promoted nationally and applied to the majority of Chinese people. On the other hand, negative findings will provide scientific evidence for abandoning a test and shifting resources elsewhere. Trial registration The study has been registered with the Protocol Registration System in Chinese Clinical Trial Registry (identifier: ChiCTR-EOR-16008577).

2017, 29(4): 303-312.
doi: 10.21147/j.issn.1000-9604.2017.04.03
Abstract:
Erythroprotein-producing human hepatocellular carcinoma receptors (Eph receptors) compose a subfamily of transmembrane protein-tyrosine kinases receptors that takes part in numerous physiological and pathological processes. Eph family receptor-interacting proteins (Ephrins) are ligands for those receptors. Eph/ephrin system is responsible for the cytoskeleton activity, cell adhesion, intercellular connection, cellular shape as well as cell motility. It affects neuron development and functioning, bone and glucose homeostasis, immune system and correct function of enterocytes. Moreover Eph/ephrin system is one of the crucial ones in angiogenesis and lymphangiogenesis. With such a wide range of impact it is clear that disturbed function of this system leads to pathology. Eph/ephrin system is involved in carcinogenesis and cancer progression. Although the idea of participation of ephrin in carcinogenesis is obvious, the exact way remains unclear because of complex bi-directional signaling and cross-talks with other pathways. Further studies are necessary to find a new target for treatment.
Erythroprotein-producing human hepatocellular carcinoma receptors (Eph receptors) compose a subfamily of transmembrane protein-tyrosine kinases receptors that takes part in numerous physiological and pathological processes. Eph family receptor-interacting proteins (Ephrins) are ligands for those receptors. Eph/ephrin system is responsible for the cytoskeleton activity, cell adhesion, intercellular connection, cellular shape as well as cell motility. It affects neuron development and functioning, bone and glucose homeostasis, immune system and correct function of enterocytes. Moreover Eph/ephrin system is one of the crucial ones in angiogenesis and lymphangiogenesis. With such a wide range of impact it is clear that disturbed function of this system leads to pathology. Eph/ephrin system is involved in carcinogenesis and cancer progression. Although the idea of participation of ephrin in carcinogenesis is obvious, the exact way remains unclear because of complex bi-directional signaling and cross-talks with other pathways. Further studies are necessary to find a new target for treatment.
2017, 29(4): 313-322.
doi: 10.21147/j.issn.1000-9604.2017.04.04
Abstract:
Objective Curative gastric cancer surgery entails removal of the primary tumor with adequate margins including regional lymph nodes. European randomized controlled trials with recruitment in the 1990’s reported increased morbidity and mortality for D2 compared to D1. Here, we examined the extent of lymphadenectomy during gastric cancer surgery and the associated risk for postoperative complications and mortality using the strengths of a population-based study. Methods A prospective nationwide study conducted within the National Register of Esophageal and Gastric Cancer. All patients in Sweden from 2006 to 2013 who underwent gastric cancer resections with curative intent were included. Patients were categorized into D0, D1, or D1+/D2, and analyzed regarding postoperative morbidity and mortality using multivariable logistic regression. Results In total, 349 (31.7%) patients had a D0, 494 (44.9%) D1, and 258 (23.4%) D1+/D2 lymphadenectomy. The 30-d postoperative complication rates were 25.5%, 25.1% and 32.2% (D0, D1 and D1+/D2, respectively), and 90-d mortality rates were 8.3%, 4.3% and 5.8%. After adjustment for confounders, in multivariable analysis, there were no significant differences in risk for postoperative complications between the lymphadenectomy groups. For 90-d mortality, there was a lower risk for D1 vs. D0. Conclusions The majority of gastric cancer resections in Sweden have included only a limited lymphadenectomy (D0 and D1). More extensive lymphadenectomy (D1+/D2) seemed to have no impact on postoperative morbidity or mortality.
2017, 29(4): 323-332.
doi: 10.21147/j.issn.1000-9604.2017.04.05
Abstract:
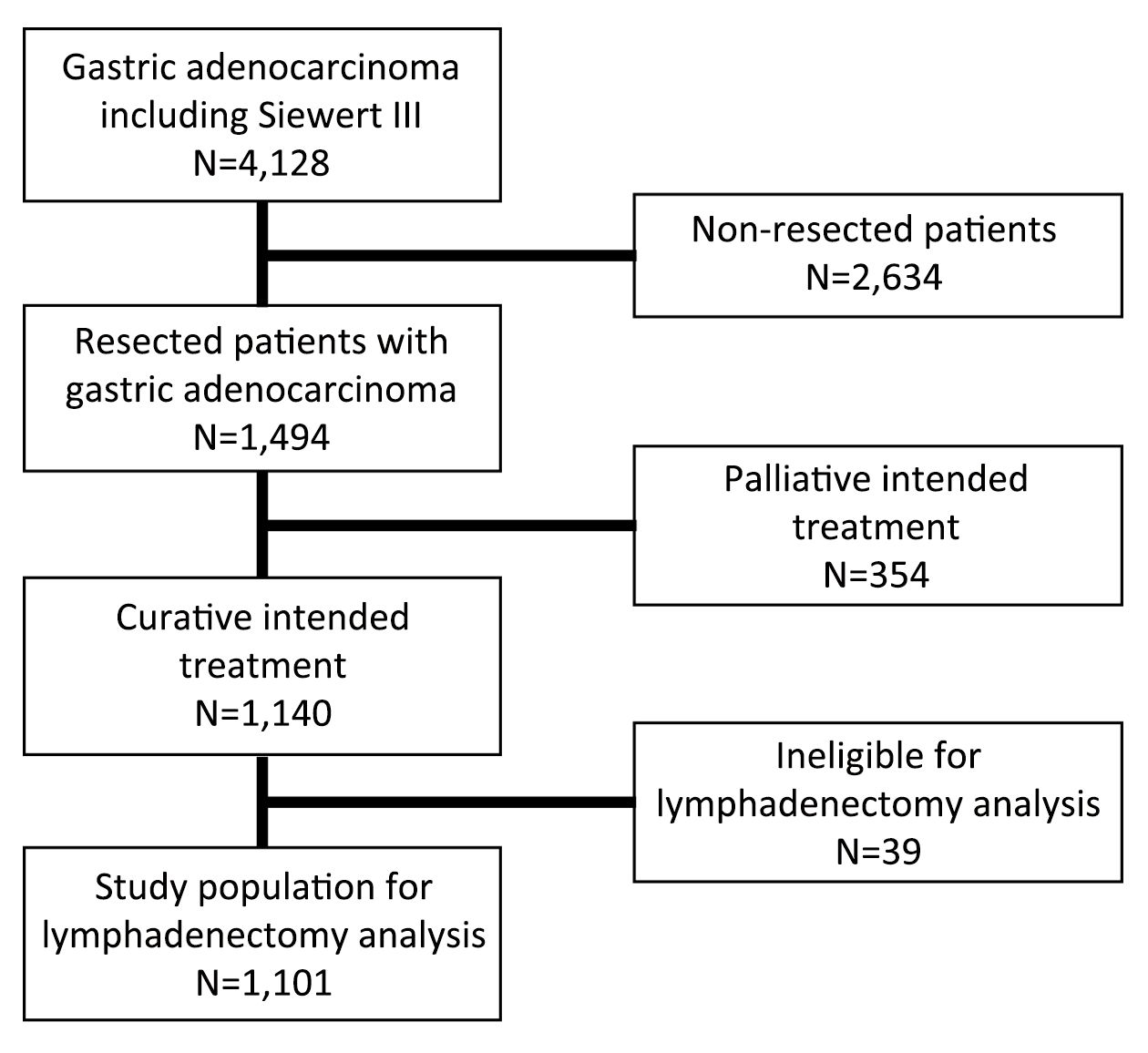
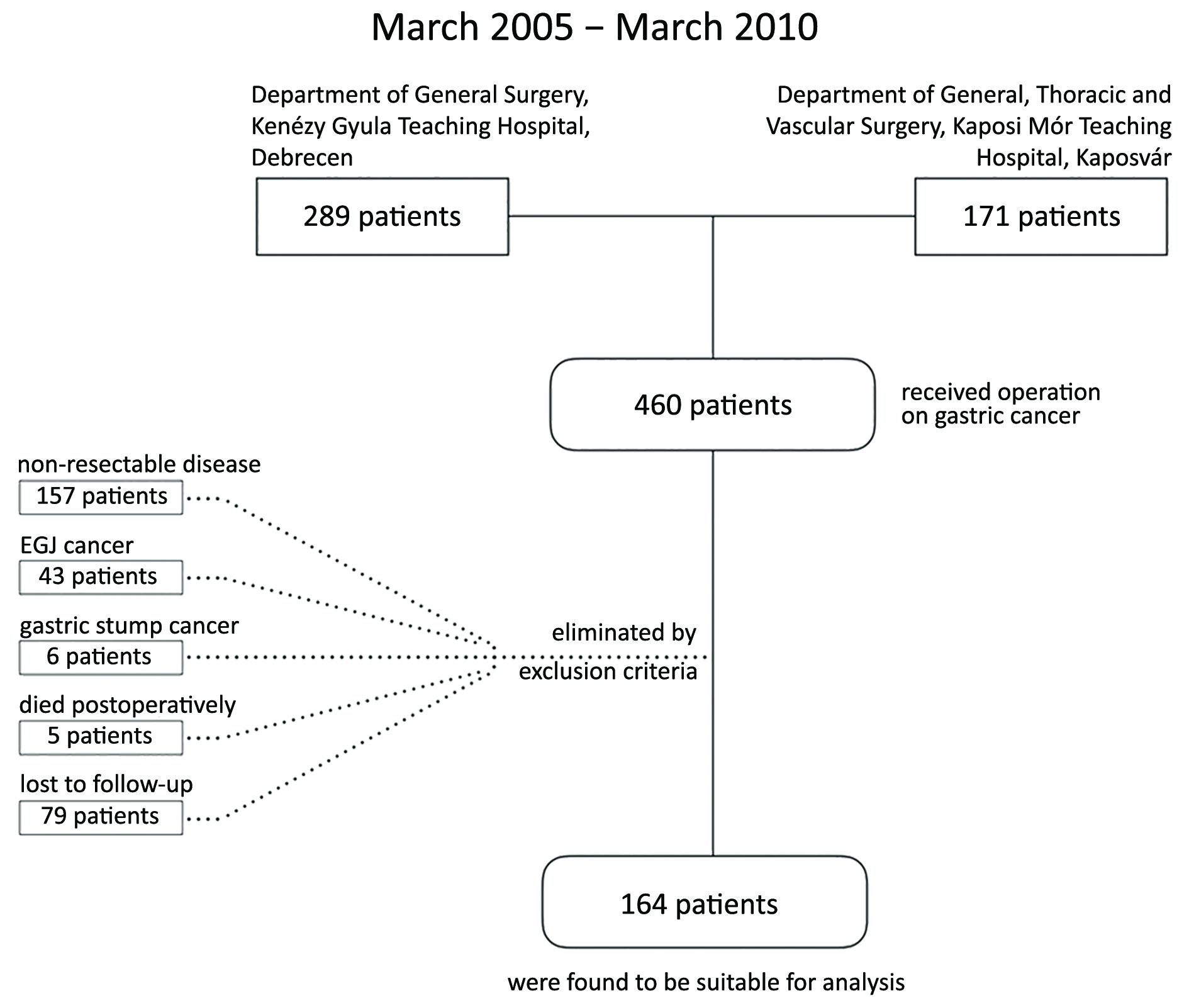
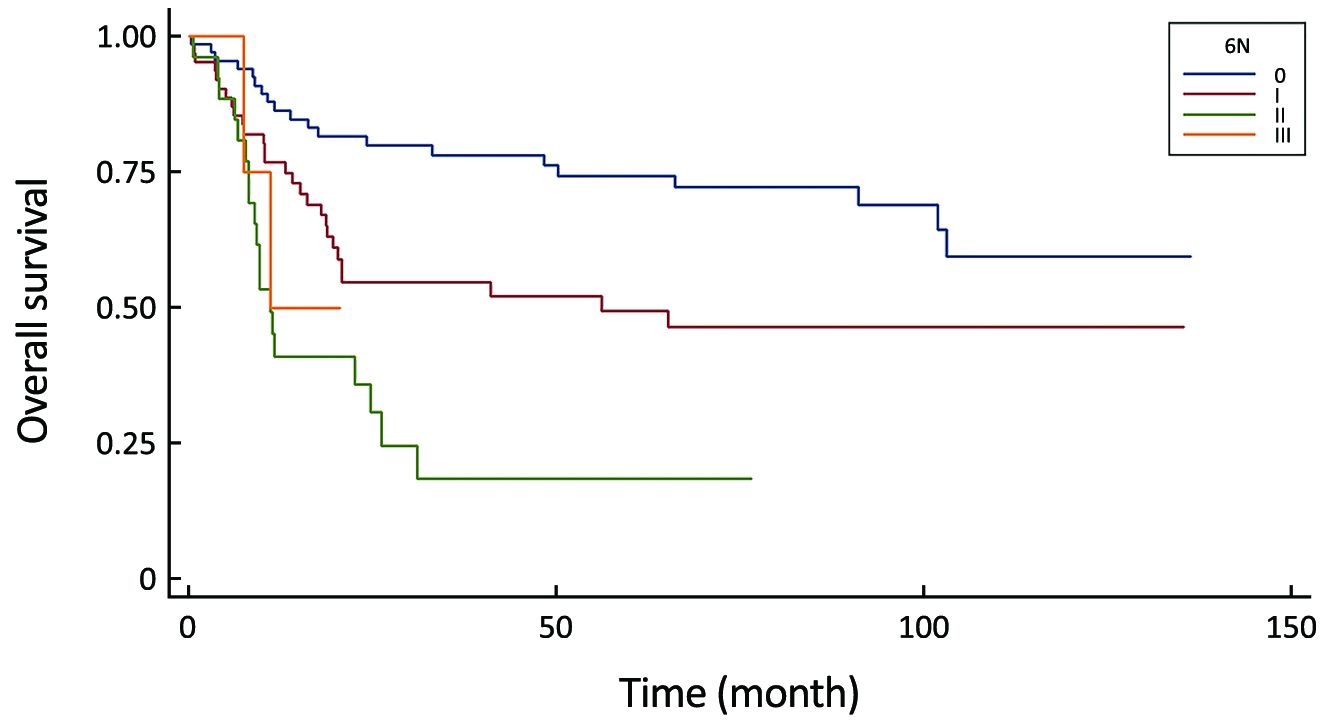
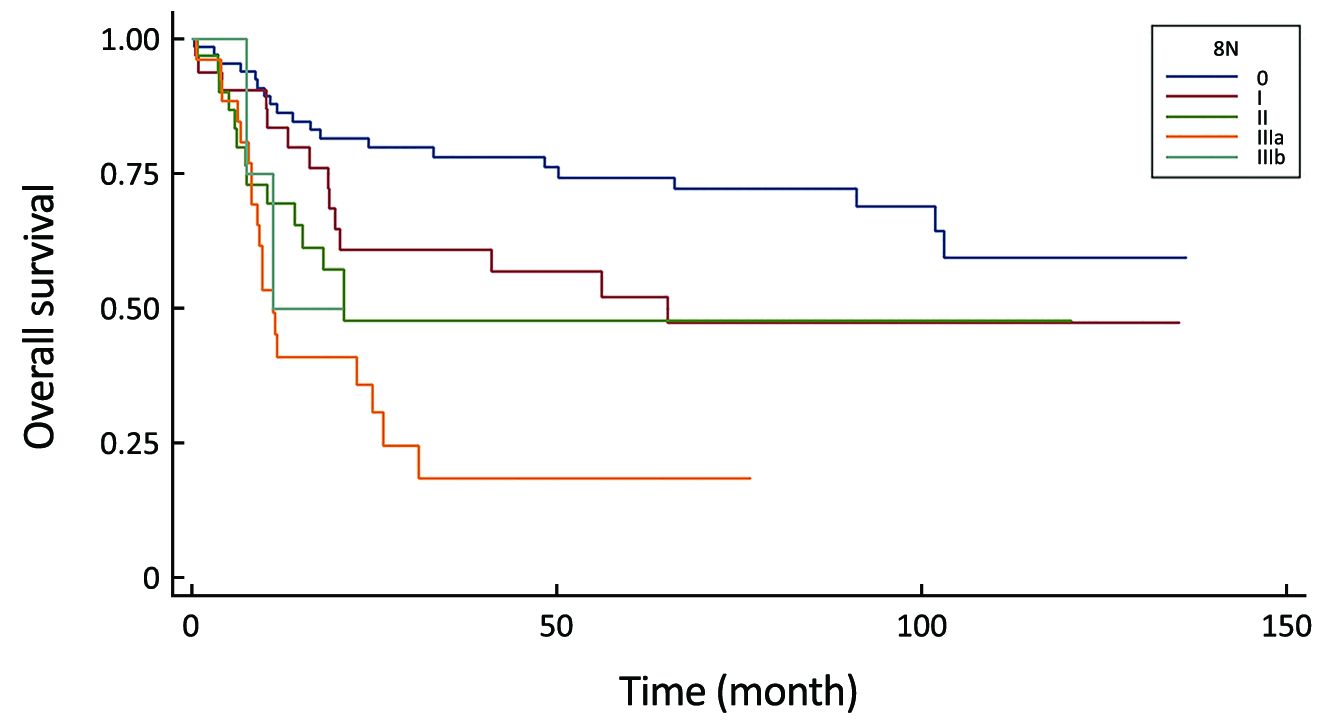
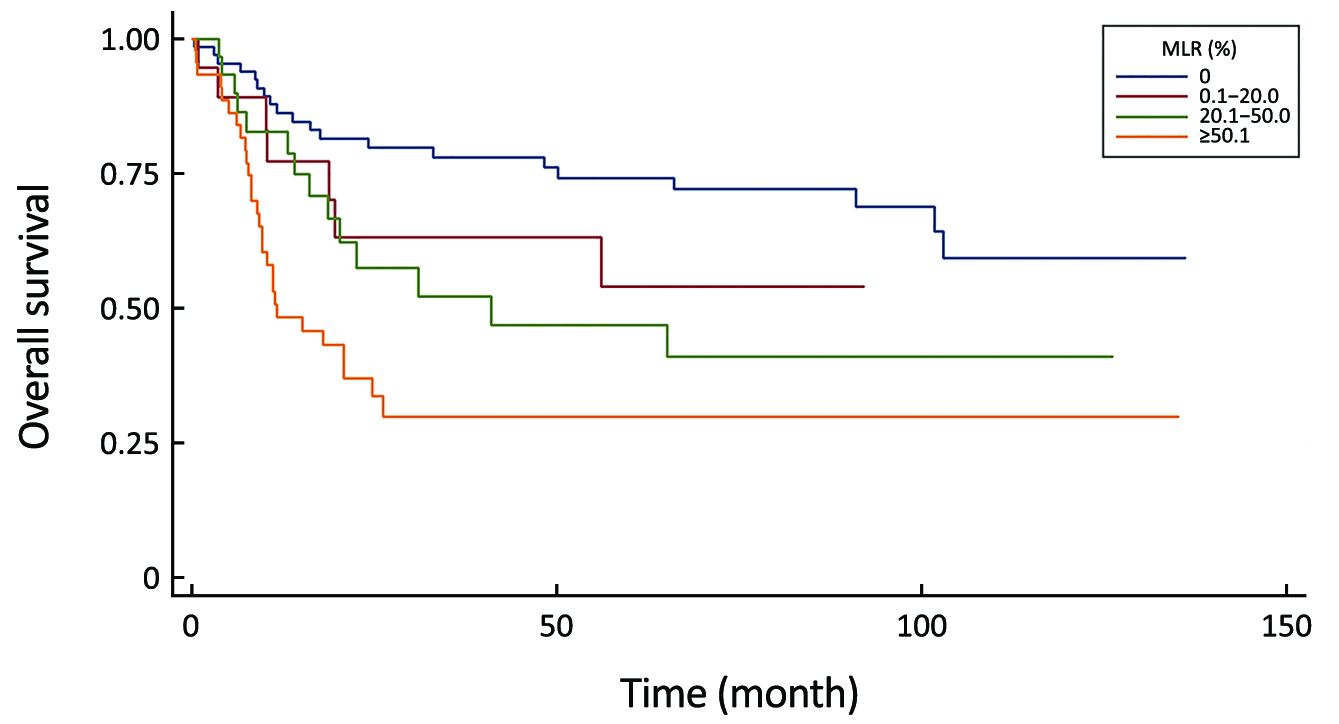
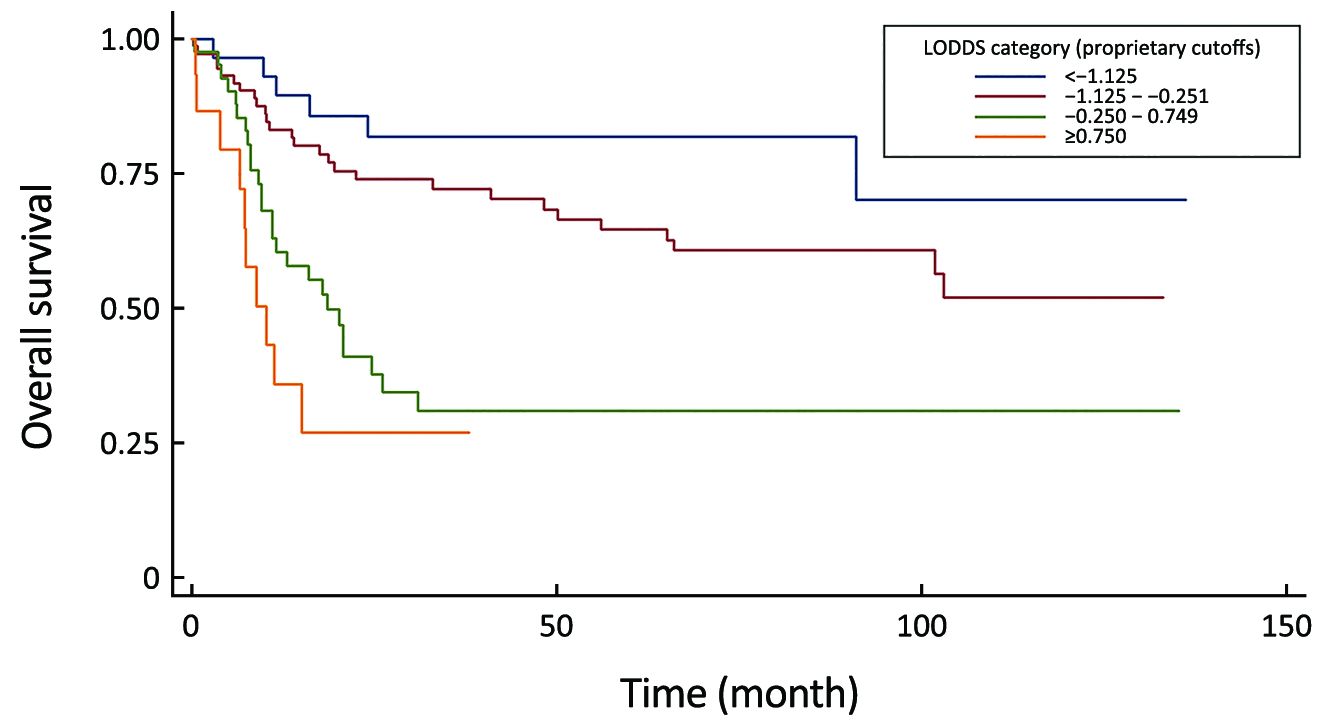
Objective The Union for International Cancer Control (UICC) Node (N) classification is the most common used staging method for the prognosis of gastric cancer. It demands adequate, at least 16 lymph nodes (LNs) to be dissected; therefore different staging systems were invented. Methods Between March 2005 and March 2010, 164 patients were evaluated at the Department of General Surgery in the Kenézy Gyula Hospital and at the Department of General, Thoracic and Vascular Surgery in the Kaposi Mór Hospital. The 6th, 7th and 8th UICC N-staging systems, the number of examined LNs, the number of harvested negative LNs, the metastatic lymph node ratio (MLR) and the log odds of positive LNs (LODDS) were determined to measure their 5-year survival rates and to compare them to each other. Results The overall 5-year survival rate for all patients was 55.5% with a median overall survival time of 102 months. The tumor stage, gender, UICC N-stages, MLR and the LODDS were significant prognostic factors for the 5-year survival with univariate analysis. The 6th UICC N-stage did not follow the adequate risk in comparing N2 vs. N0 and N3 vs. N0 with multivariate investigation. Comparison of performances of the residual N classifications proved that the LODDS system was first in the prediction of prognosis during the evaluation of all patients and in cases with less than 16 harvested LNs. The MLR gave the best prognostic prediction when adequate (more than or equal to 16) lymphadenectomy was performed. Conclusions We suggest the application of LODDS system routinely in western patients and the usage of MLR classification in cases with extended lymphadenectomy.

2017, 29(4): 333-340.
doi: 10.21147/j.issn.1000-9604.2017.04.06
Abstract:
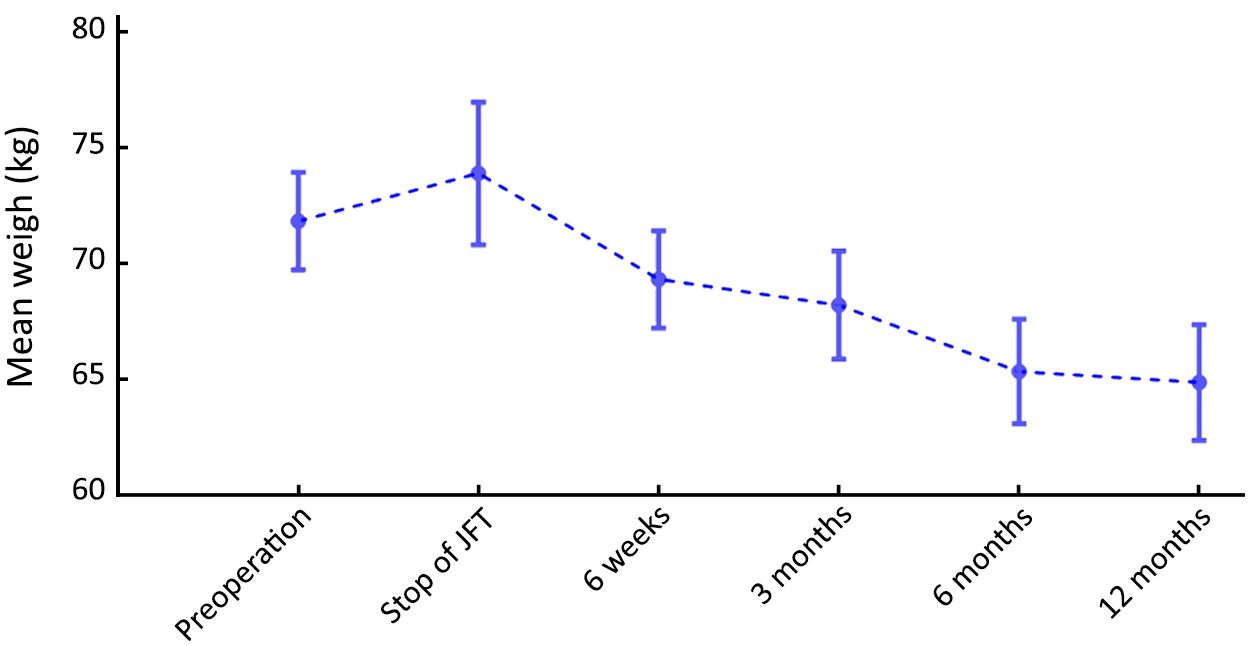
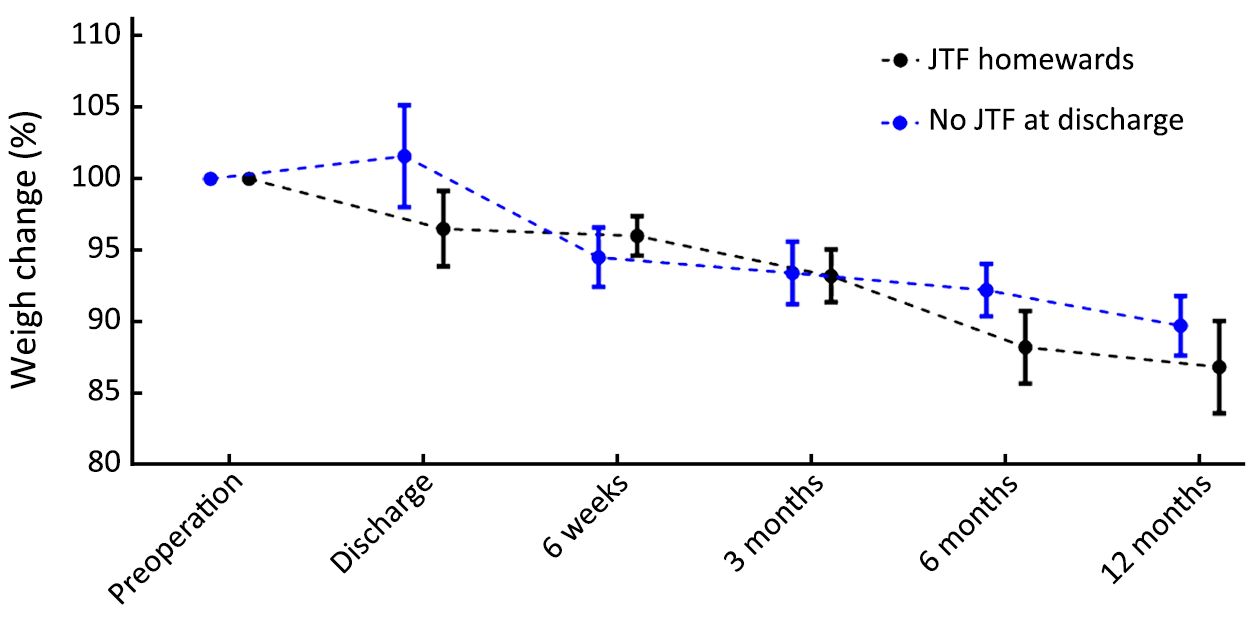
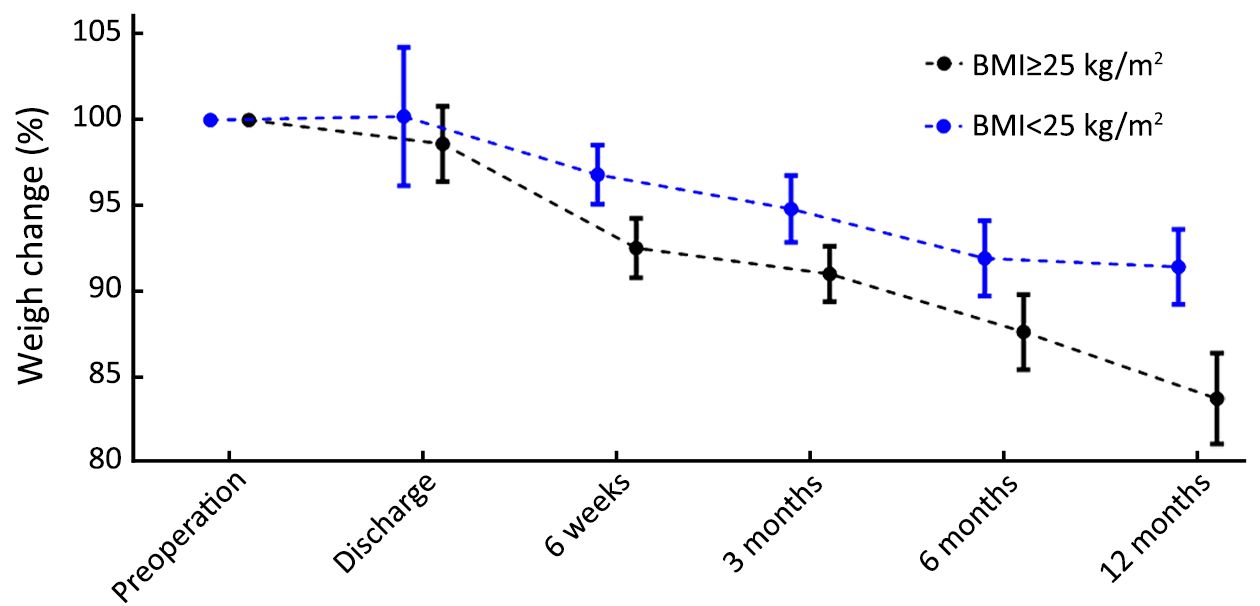
Objective Patients undergoing total gastrectomy for cancer are at risk of malnourishment. The aim of this self-controlled study was to examine the effect of jejunostomy tube feeding (JTF) and other factors on postoperative weight and the incidence of jejunostomy-related complications in patients undergoing total gastrectomy for cancer. Methods All consecutive patients who underwent total gastrectomy for gastric cancer with jejunostomy placement were included from a prospective single-center database (2003–2014). Jejunostomy-related complications and postoperative weight changes were evaluated up to 12 months after surgery. Multivariable linear regression analysis was performed to identify factors associated with weight loss 12 months after gastrectomy. Results Of 113 patients operated in the study period, 65 received JTF after total gastrectomy for a median duration of 18 d [interquartile range (IQR), 10–55 d]. Jejunostomy-related complications occurred in 11 (17%) patients, including skin leakage (n=3) and peritoneal leakage (n=2), luxation (n=3), occlusion (n=2), infection (n=1) and torsion (n=1). In 2 (3%) patients, a reoperation was needed due to jejunostomy-related complications. The mean preoperative weight of patients was 71.8 kg (100%), and remained stable during JTF (73.9 kg, 103%, P=0.331). After JTF was stopped, the mean weight of patients decreased to 64.9 kg (90%) at 12 months after surgery (P<0.001). A high preoperative body mass index (BMI) (≥25 kg/m2) was associated with high postoperative weight loss compared to patients with a low BMI (<25 kg/m2) (16.3% vs. 8.6%, P=0.016). Conclusions JTF can prevent weight loss in the early postoperative phase. However, this is at the prize of possible complications. As weight loss in the long term is not prevented, routine JTF should be re-evaluated and balanced against the selected use in preoperatively malnourished patients. Special attention should be paid to patients with a high preoperative BMI, who are at risk of more postoperative weight loss.
2017, 29(4): 341-350.
doi: 10.21147/j.issn.1000-9604.2017.04.07
Abstract:
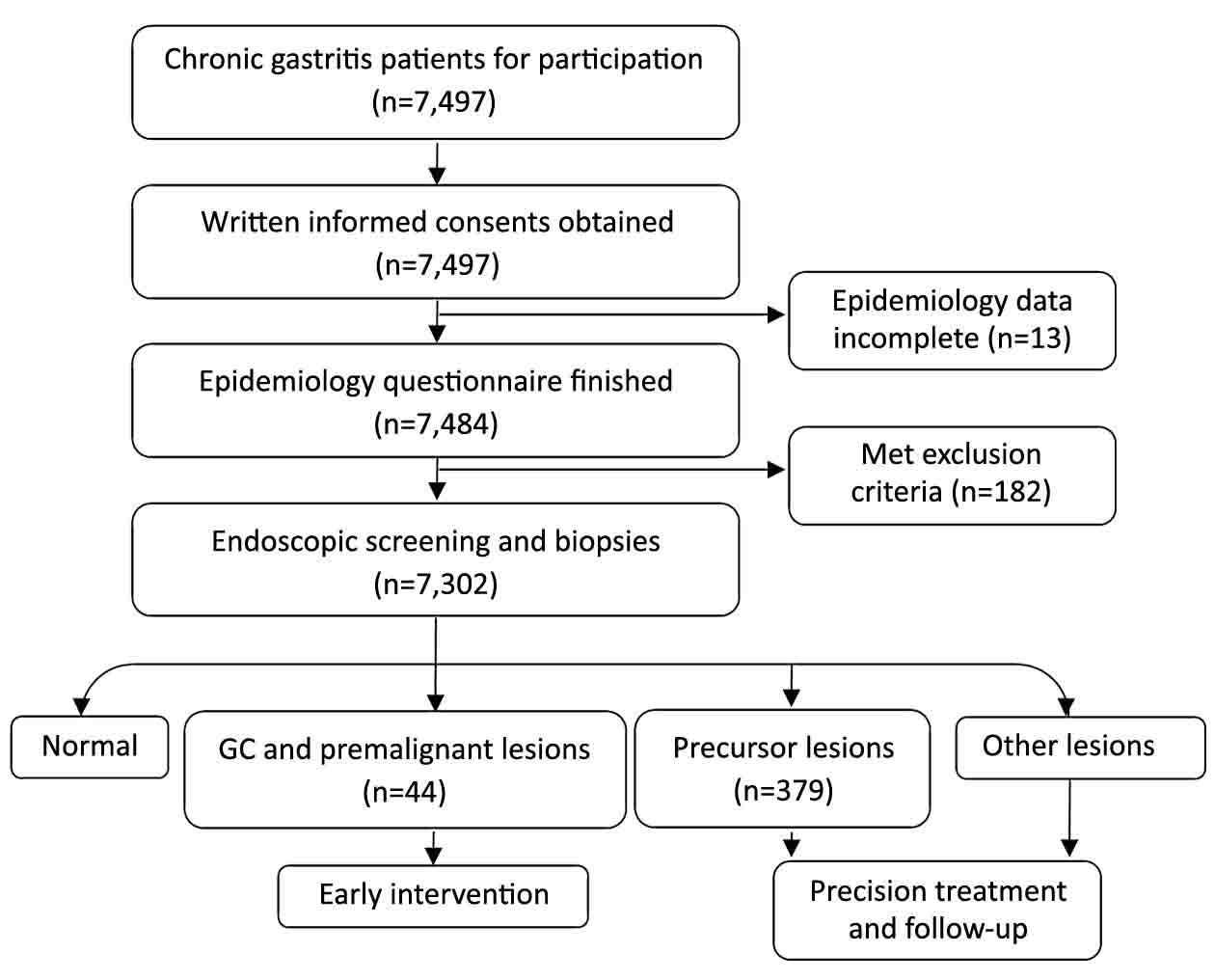
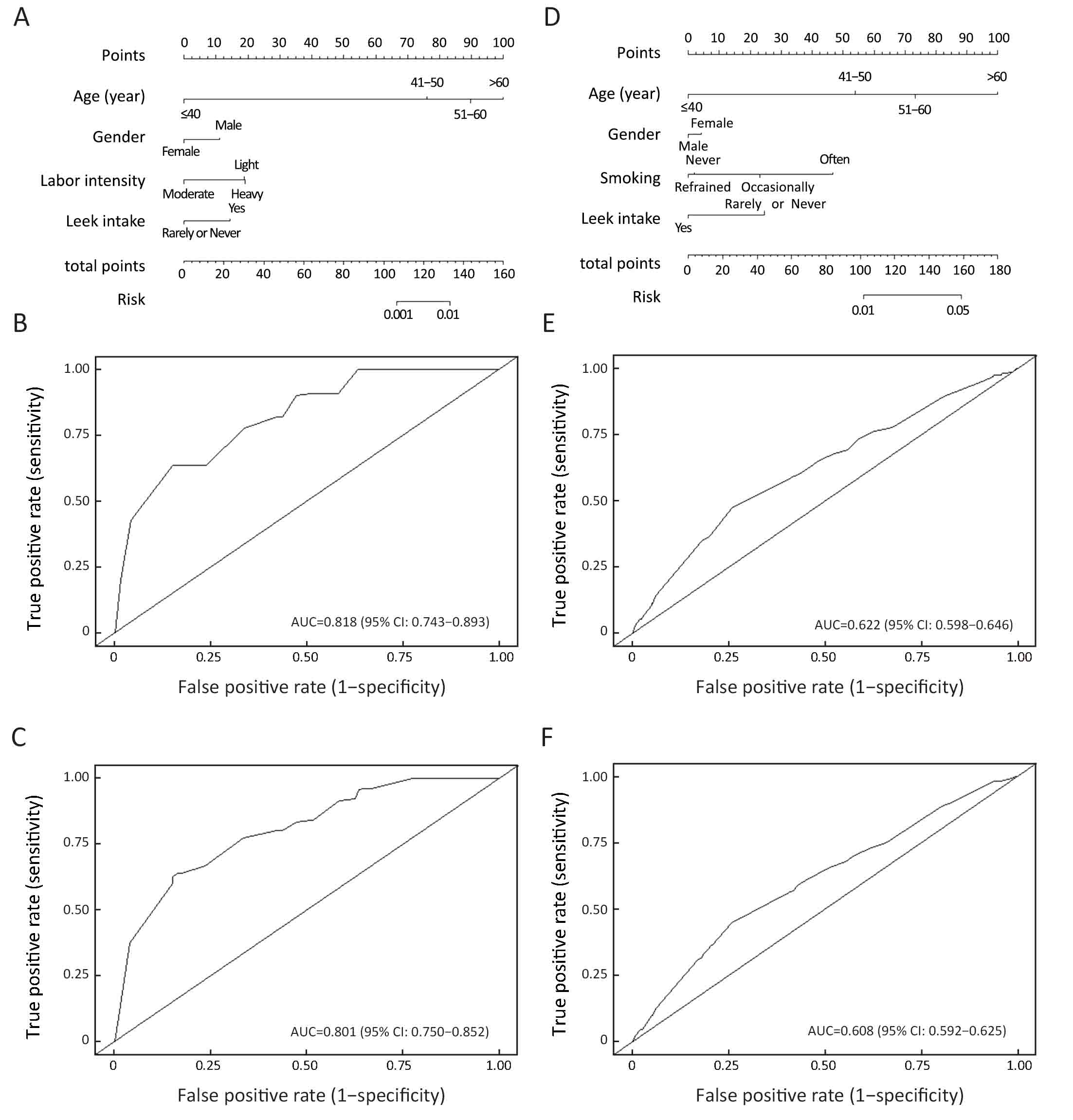
Objective Gastric cancer (GC) is one of the leading causes of death in China and other Asian countries. Recently, gastric endoscopy has become the main approach for GC screening, but the identification of high-risk individuals remains a challenge in GC screening programs. Methods There were 7,302 patients with chronic gastritis involved in this study. Endoscopic examinations were performed, and their demographic characteristics and lifestyle data were collected. Each possible associated factor of GC/premalignant and precursor lesions was evaluated by univariate and multivariate logistic regressions. Nomograms were used for visualization of those models, and receiver operating characteristic (ROC) curve analysis was used to present the predictive accuracy. Results We detected 8 (0.11%) gastric adenocarcinomas, 17 (0.23%) dysplasia cases, 14 (0.19%) hyperplasia cases, 52 (0.71%) intestinal metaplasia cases, 217 (2.97%) inflammatory lesions, 141 (1.93%) gastric ulcers, 10 (0.14%) atrophic gastritis cases, 1,365 (18.69%) erosive gastritis cases, and 5,957 (81.58%) superficial gastritis cases in 7,302 patients. The age (P<0.001), gender (P=0.086), labor intensity (P=0.018) and leek food intake (P=0.143) were identified as independent predictive factors of GC/premalignant lesions possibility. The corresponding nomogram exhibited an area under the curve (AUC) [95% confidence interval (95% CI)] of 0.82 (0.74–0.89) for the modeling group and 0.80 (0.75–0.85) for the validation group. The age (P=0.002), gender (P=0.024), smoking (P=0.002) and leek food intake (P=0.039) were independent predictive factors of precursor lesions possibility. The corresponding nomogram exhibited an AUC (95% CI) of 0.62 (0.60–0.65) for the modeling group and 0.61 (0.59–0.63) for the validation group. Conclusions We identified several potential associated factors and provided a preclinical nomogram with the potential to predict the possibility of GC/premalignant and precursor lesions.
2017, 29(4): 351-360.
doi: 10.21147/j.issn.1000-9604.2017.04.08
Abstract:
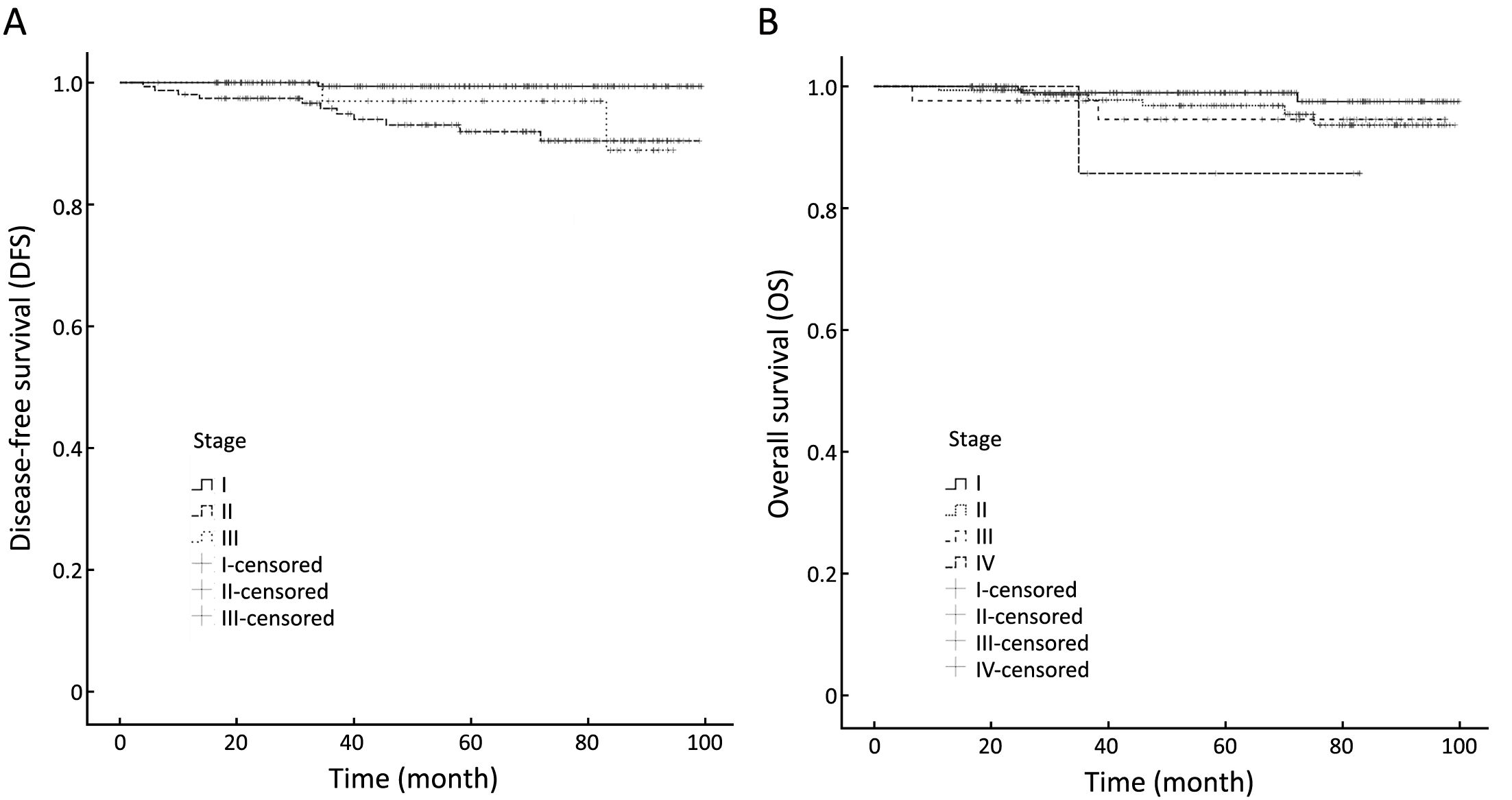
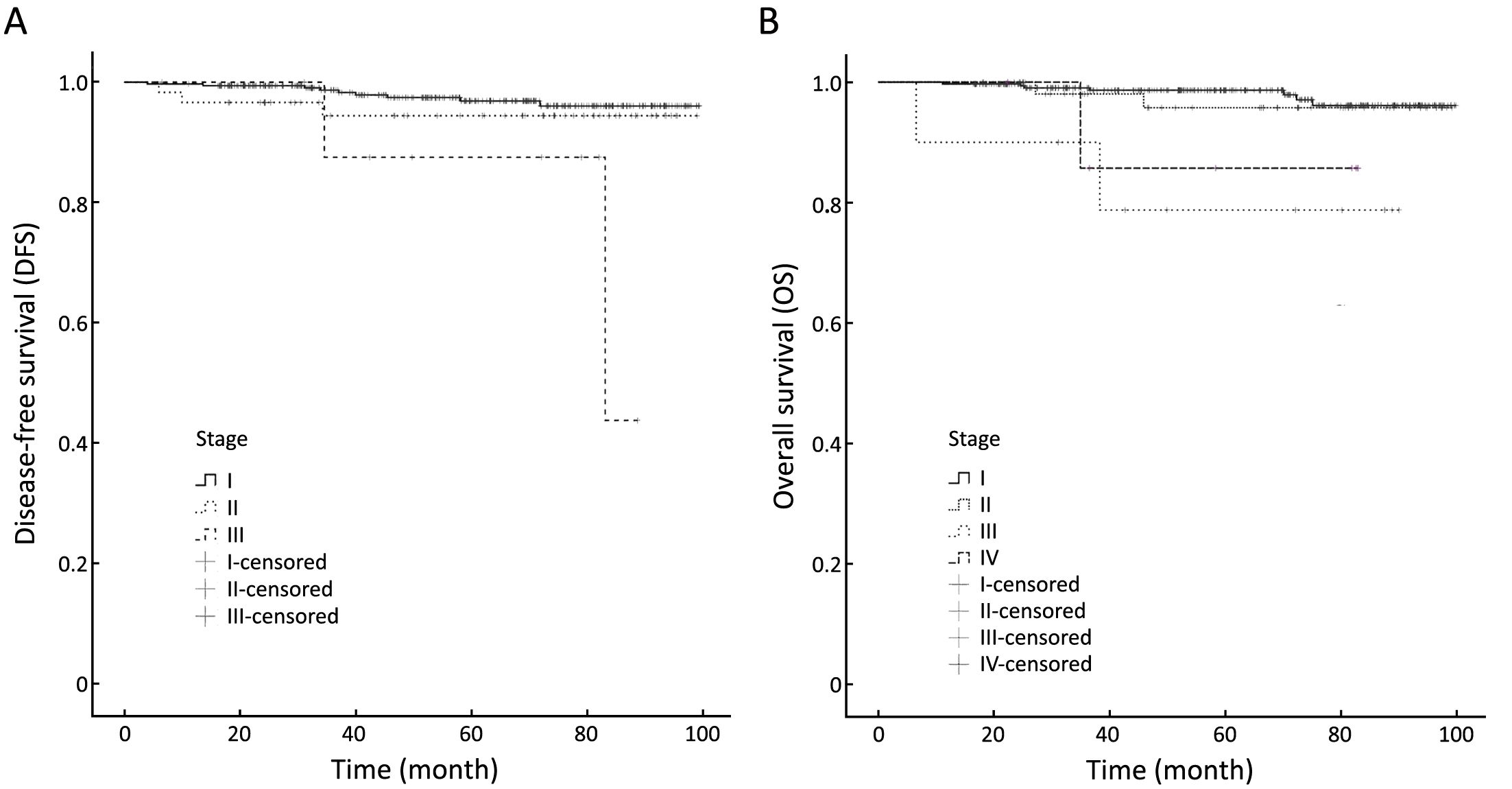
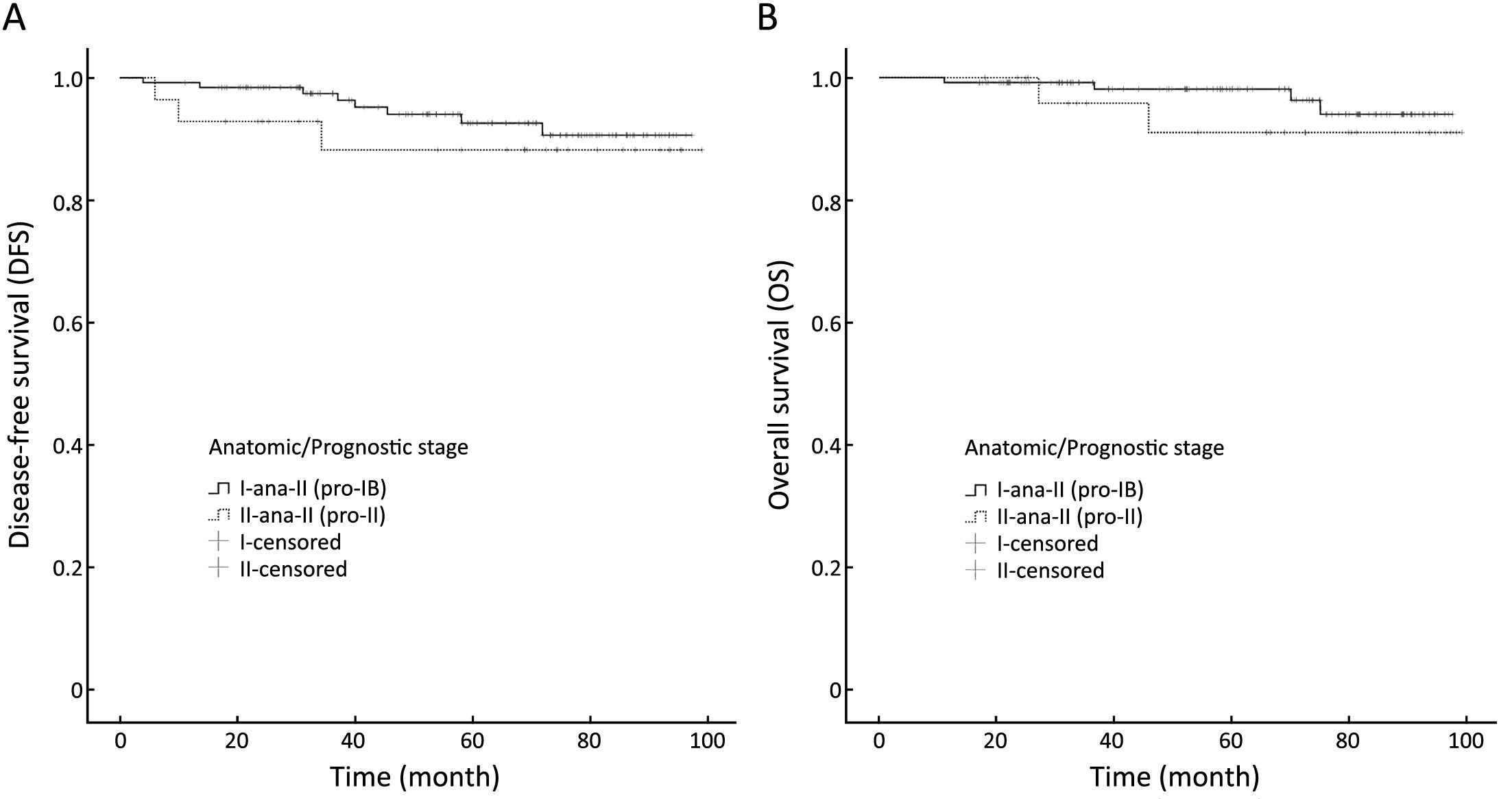
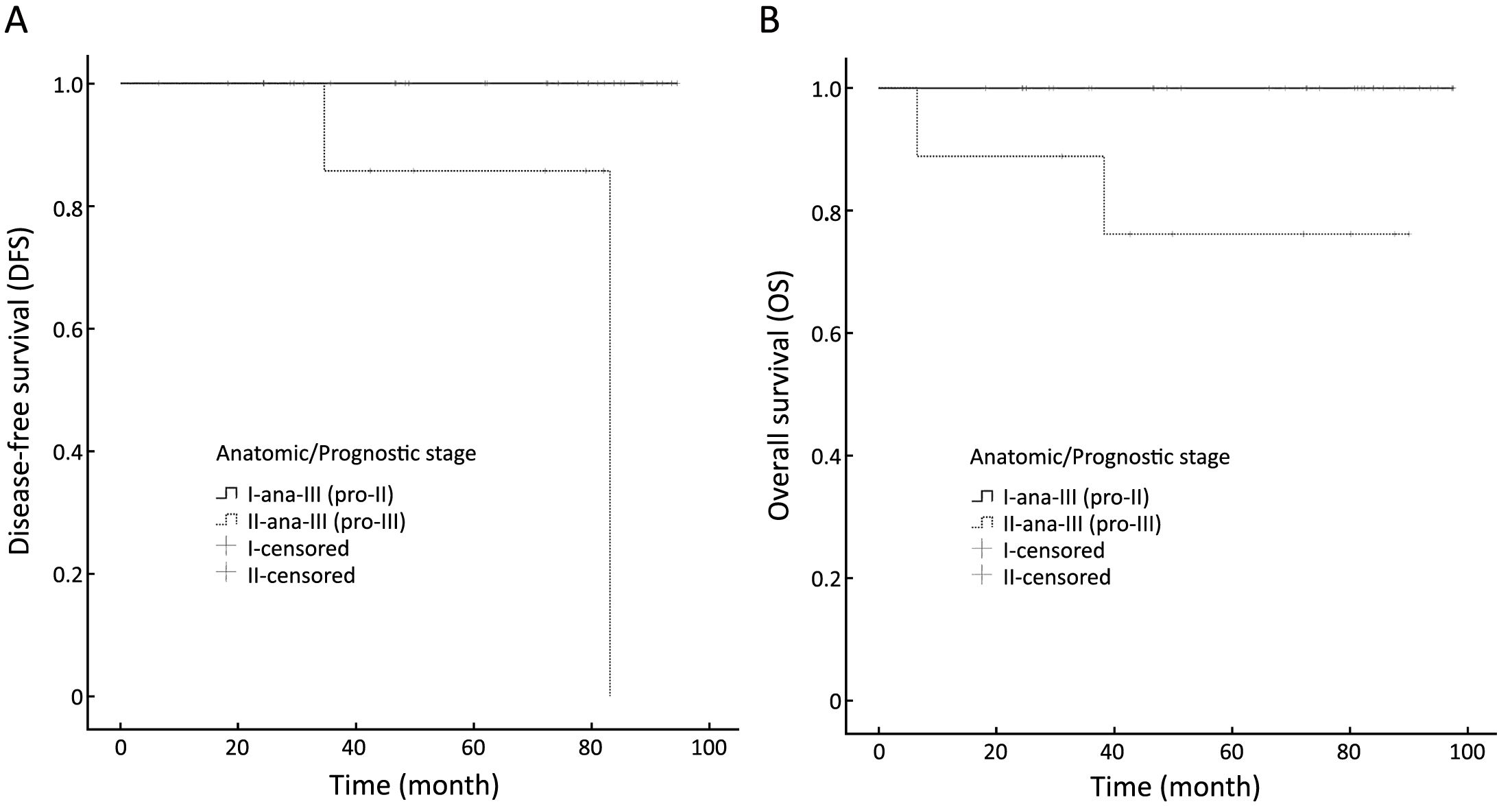
Objective We retrospectively analyzed the clinical prognostic value of the 8th edition of the American Joint Committee on Cancer (AJCC) staging system for luminal A breast cancer. Methods Using both the anatomic and prognostic staging in the 8th edition of AJCC cancer staging system, we restaged patients with luminal A breast cancer treated at the Breast Disease Center, Peking University First Hospital from 2008 to 2014. Follow-up data including 5-year disease free survival (DFS), overall survival (OS) and other clinic-pathological data were collected to analyze the differences between the two staging subgroups. Results This study included 421 patients with luminal A breast cancer (median follow-up, 61 months). The 5-year DFS and OS rates were 98.3% and 99.3%, respectively. Significant differences in 5-year DFS but not OS were observed between different anatomic disease stages. Significant differences were observed in both 5-year DFS and OS between different prognostic stages. Application of the prognostic staging system resulted in assignment of 175 of 421 patients (41.6%) to a different group compared to their original anatomic stages. In total, 102 of 103 patients with anatomic stage IIA changed to prognostic stage IB, and 24 of 52 patients with anatomic stage IIB changed to prognostic stage IB, while 1 changed to prognostic stage IIIB. Twenty-two of 33 patients with anatomic stage IIIA were down-staged to IIA when staged by prognostic staging system, and the other 11 patients were down-staged to IIB. Two patients with anatomic stage IIIB were down-staged to IIIA. Among seven patients with anatomic stage IIIC cancer, two were down-staged to IIIA and four were down-staged to stage IIIB. Conclusions The 8th edition of AJCC prognostic staging system is an important supplement to the breast cancer staging system. More clinical trials are needed to prove its ability to guide selection of proper systemic therapy and predict prognosis of breast cancer.
2017, 29(4): 361-368.
doi: 10.21147/j.issn.1000-9604.2017.04.09
Abstract:
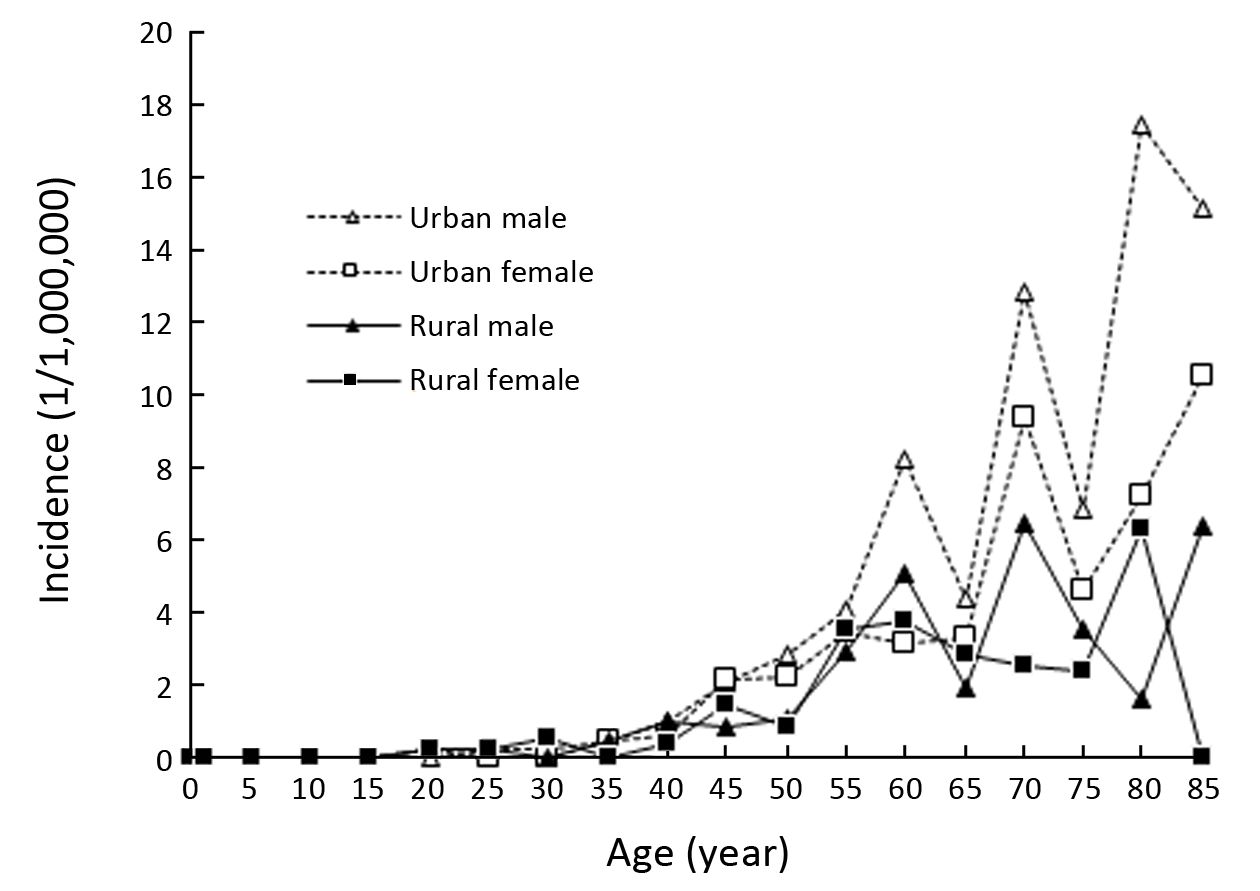
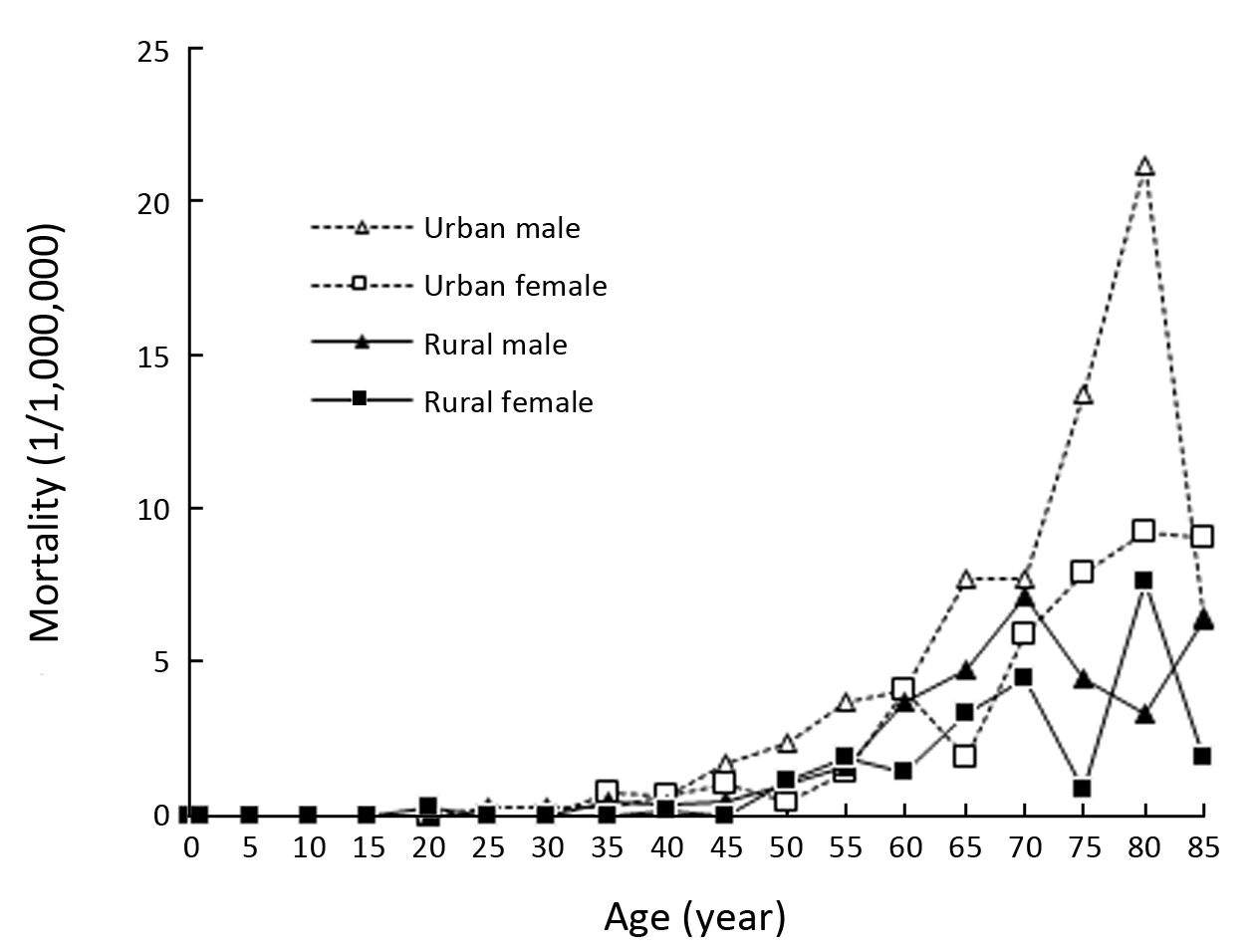
Objective Population-based cancer registration data were used to analyze the epidemiology and trend of malignant mesothelioma in China, and the result would provide basic data for its prevention and control. Methods Malignant mesothelioma data in 2013 were retrieved from the database of National Cancer Registry. Malignant mesothelioma incidence and mortality were estimated using age-specific rate by urban/rural and gender according to the national population in 2013. Malignant mesothelioma data from 22 cancer registries were used for trend analysis during 2000–2013. Results It is estimated that there were 2,041 new malignant mesothelioma cases and 1,659 malignant mesothelioma deaths occurred in 2013. The crude incidence rate in China were 1.50/106 (males 1.67/106, females 1.32/106), age-standardized incidence rates by Chinese standard population (ASIRC) and by world standard population (ASIRW) were 1.03/106 and 1.02/106, respectively. The crude mortality rate in China was 1.22/106 (males 1.67/106, females 1.32/106), age-standardized mortality rates by Chinese standard population (ASMRC) and by world standard population (ASMRW) were 0.83/106 and 0.81/106, respectively. There was an increasing trend of incidence rate for malignant mesothelioma in registration areas of China during 2000–2013 with annual percentage change (APC) of 2.5% [95% confidence interval (95% CI): 0.6%–4.5%]. After age standardization, no significant differences were observed. No matter for crude mortality rates or age-standardized mortality rates, no significant differences were observed during 2000–2013. Conclusions Malignant mesothelioma is the major occupational and environmental neoplasm associated with asbestos exposure. The increasing incidence trend suggests that more attention should be paid on this disease.
2017, 29(4): 369-373.
doi: 10.21147/j.issn.1000-9604.2017.04.10
Abstract:
There is a lack of investigation into the biological characteristics and preoperative systemic therapy (PST) for occult breast cancer (OBC). For this study, departmental records in Breast Disease Center of Peking University First Hospital from January 2008 to December 2015 were retrospectively reviewed to identify cases of OBC. Eleven cases were included, and all patients were female, with a median age of 56 (range: 29–75) years. The sensitivity of magnetic resonance imaging (MRI) was 100%, and the false positive rate was 33.3%. Based on histologic analysis of the axillary node, 9 (81.8%) cases were grade 3, and 2 (18.2%) cases were grade 2; 4 (36.4%) cases were ≥10% estrogen receptor (ER) positive and 6 (54.5%) human epidermal growth receptor 2 (HER2) positive. Nine cases (81.8%) exhibited over 30% Ki67 expression. PST was performed in 5 of the 11 cases. The lymph node response rate was 100% (5/5), but no complete remission was achieved. In conclusion, aggressive subtypes were predominant among the included cases, and PST should be considered for OBC treatment options.
There is a lack of investigation into the biological characteristics and preoperative systemic therapy (PST) for occult breast cancer (OBC). For this study, departmental records in Breast Disease Center of Peking University First Hospital from January 2008 to December 2015 were retrospectively reviewed to identify cases of OBC. Eleven cases were included, and all patients were female, with a median age of 56 (range: 29–75) years. The sensitivity of magnetic resonance imaging (MRI) was 100%, and the false positive rate was 33.3%. Based on histologic analysis of the axillary node, 9 (81.8%) cases were grade 3, and 2 (18.2%) cases were grade 2; 4 (36.4%) cases were ≥10% estrogen receptor (ER) positive and 6 (54.5%) human epidermal growth receptor 2 (HER2) positive. Nine cases (81.8%) exhibited over 30% Ki67 expression. PST was performed in 5 of the 11 cases. The lymph node response rate was 100% (5/5), but no complete remission was achieved. In conclusion, aggressive subtypes were predominant among the included cases, and PST should be considered for OBC treatment options.
2017, 29(4): 374-378.
doi: 10.21147/j.issn.1000-9604.2017.04.11
Abstract:
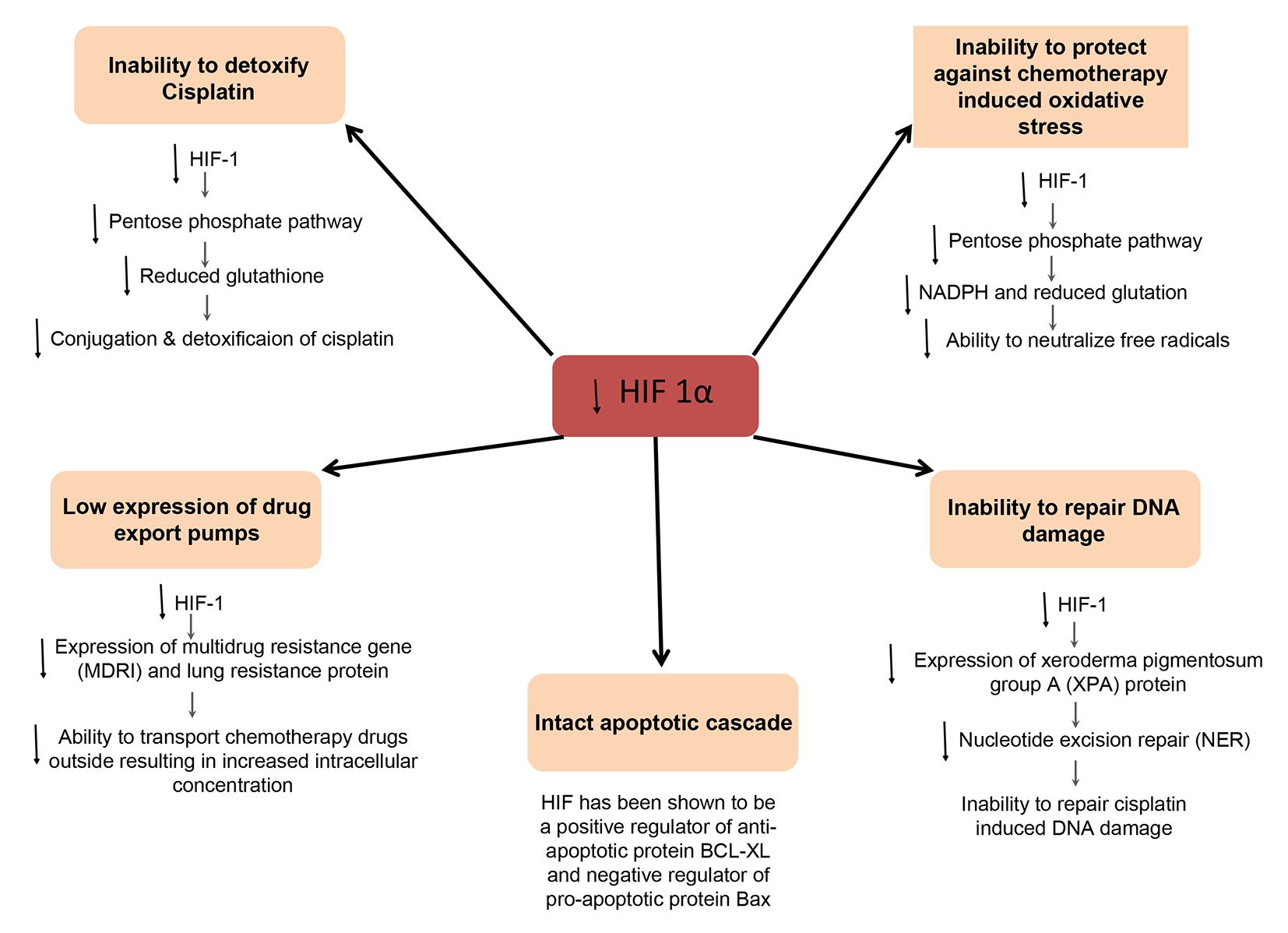
The molecular basis for enhanced chemosensitivity of testicular germ cell tumors (GCT) has been an area of great interest, as it could potentially give us therapeutic leads in other resistant malignancies. Thus far, however, the increased sensitivity of GCT has been variously attributed to multiple factors — an inability to detoxify cisplatin, a lack of export pumps, an inability to repair the DNA damage, an intact apoptotic cascade and lack of p53 mutation; but a unifying underlying etiology leading to the aforementioned processes and having a translational implication has so far been elusive. Herein, we offer evidence to support a potential significant role for the previously demonstrated low hypoxia inducible factor-1α (HIF-1α) expression in mediating the general exquisite chemosensitivity of testicular GCT, through the aforementioned processes. This molecular mechanism based hypothesis could have a significant translational implication in platinum refractory GCT as well as other platinum resistant malignancies.
The molecular basis for enhanced chemosensitivity of testicular germ cell tumors (GCT) has been an area of great interest, as it could potentially give us therapeutic leads in other resistant malignancies. Thus far, however, the increased sensitivity of GCT has been variously attributed to multiple factors — an inability to detoxify cisplatin, a lack of export pumps, an inability to repair the DNA damage, an intact apoptotic cascade and lack of p53 mutation; but a unifying underlying etiology leading to the aforementioned processes and having a translational implication has so far been elusive. Herein, we offer evidence to support a potential significant role for the previously demonstrated low hypoxia inducible factor-1α (HIF-1α) expression in mediating the general exquisite chemosensitivity of testicular GCT, through the aforementioned processes. This molecular mechanism based hypothesis could have a significant translational implication in platinum refractory GCT as well as other platinum resistant malignancies.