2017 Vol.29(5)
Display Mode: |
2017, 29(5): 379-384.
doi: 10.21147/j.issn.1000-9604.2017.05.01
 Abstract
Abstract FullText HTML
FullText HTML PDF 190KB
PDF 190KB
Abstract:
Secretory carcinoma (SC), previously described as mammary analogue secretory carcinoma (MASC), is a recently described salivary gland tumor which morphologically resembles mammary secretory carcinoma. The first description of SC/MASC, reported by Skálová et al. in 2010, was as a rare salivary carcinoma imitating secretory carcinoma of the breast. SC/MASC is a unique salivary gland tumor with morphological overlap with acinic cell carcinoma (AciCC), mucoepidermoid carcinoma (MEC), and adenocarcinoma not otherwise specified (ADC-NOS). SC/MASC shares similar clinicopathological features with AciCC. As a critical difference between SC/MASC and AciCC, SC/MASC characteristically has the chromosomal translocation t(12;15)(p13;q25) which leads to a fusion gene between the ETV6 gene on chromosome 12 and the NTRK3 gene on chromosome 15. This genetic background is an important differential diagnostic finding for excluding other salivary gland tumors and may be a critical factor determining the prognosis for patients with SC/MASC. Research in recent years has provided a large body of new data on SC/MASC and suggests the possibility that the ETV6-NTRK3 translocation could be a therapeutic target. Here, we review the morphological and clinicopathological features of SC/MASC and discuss new directions for therapy.
Secretory carcinoma (SC), previously described as mammary analogue secretory carcinoma (MASC), is a recently described salivary gland tumor which morphologically resembles mammary secretory carcinoma. The first description of SC/MASC, reported by Skálová et al. in 2010, was as a rare salivary carcinoma imitating secretory carcinoma of the breast. SC/MASC is a unique salivary gland tumor with morphological overlap with acinic cell carcinoma (AciCC), mucoepidermoid carcinoma (MEC), and adenocarcinoma not otherwise specified (ADC-NOS). SC/MASC shares similar clinicopathological features with AciCC. As a critical difference between SC/MASC and AciCC, SC/MASC characteristically has the chromosomal translocation t(12;15)(p13;q25) which leads to a fusion gene between the ETV6 gene on chromosome 12 and the NTRK3 gene on chromosome 15. This genetic background is an important differential diagnostic finding for excluding other salivary gland tumors and may be a critical factor determining the prognosis for patients with SC/MASC. Research in recent years has provided a large body of new data on SC/MASC and suggests the possibility that the ETV6-NTRK3 translocation could be a therapeutic target. Here, we review the morphological and clinicopathological features of SC/MASC and discuss new directions for therapy.
2017, 29(5): 385-394.
doi: 10.21147/j.issn.1000-9604.2017.05.02
Abstract:
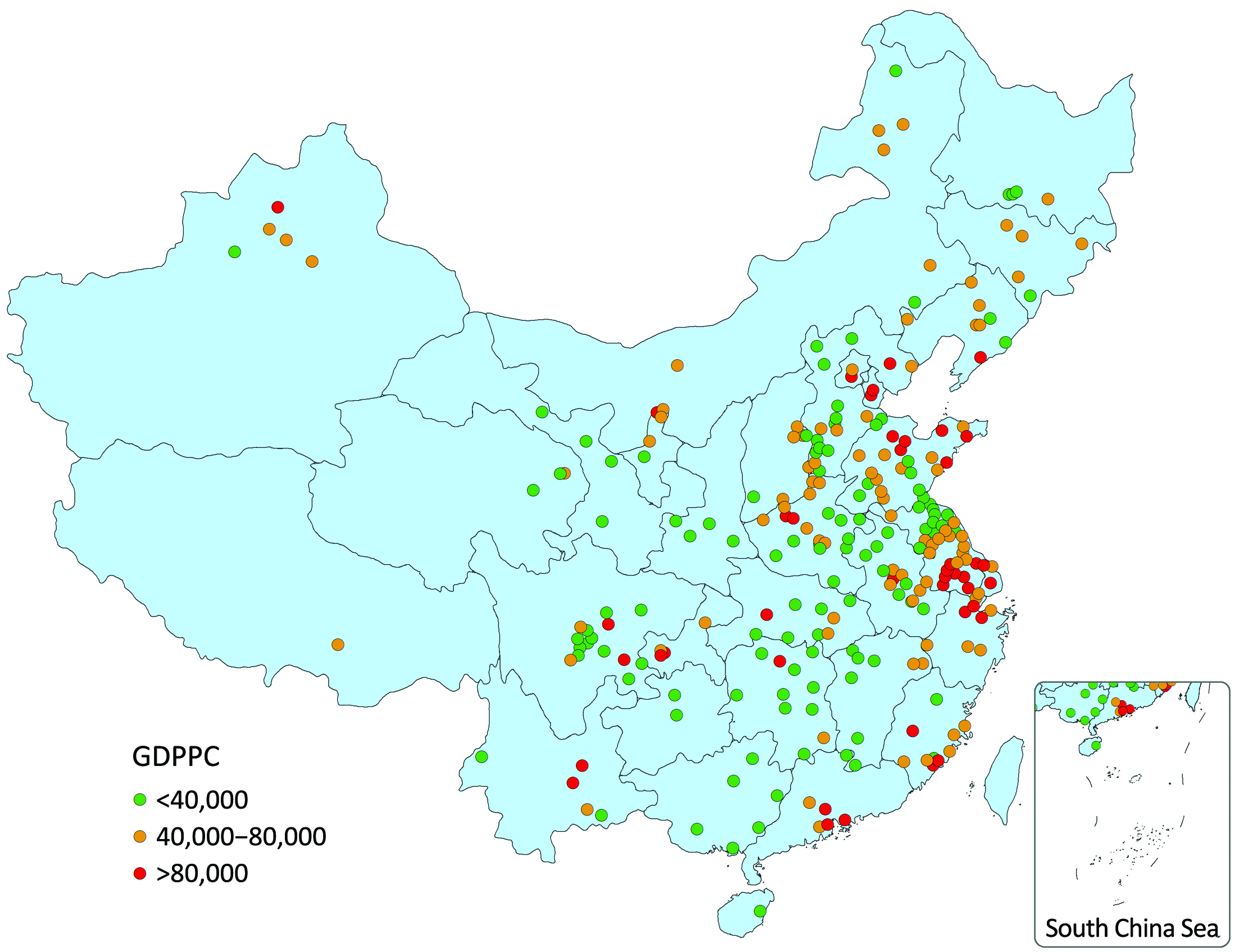
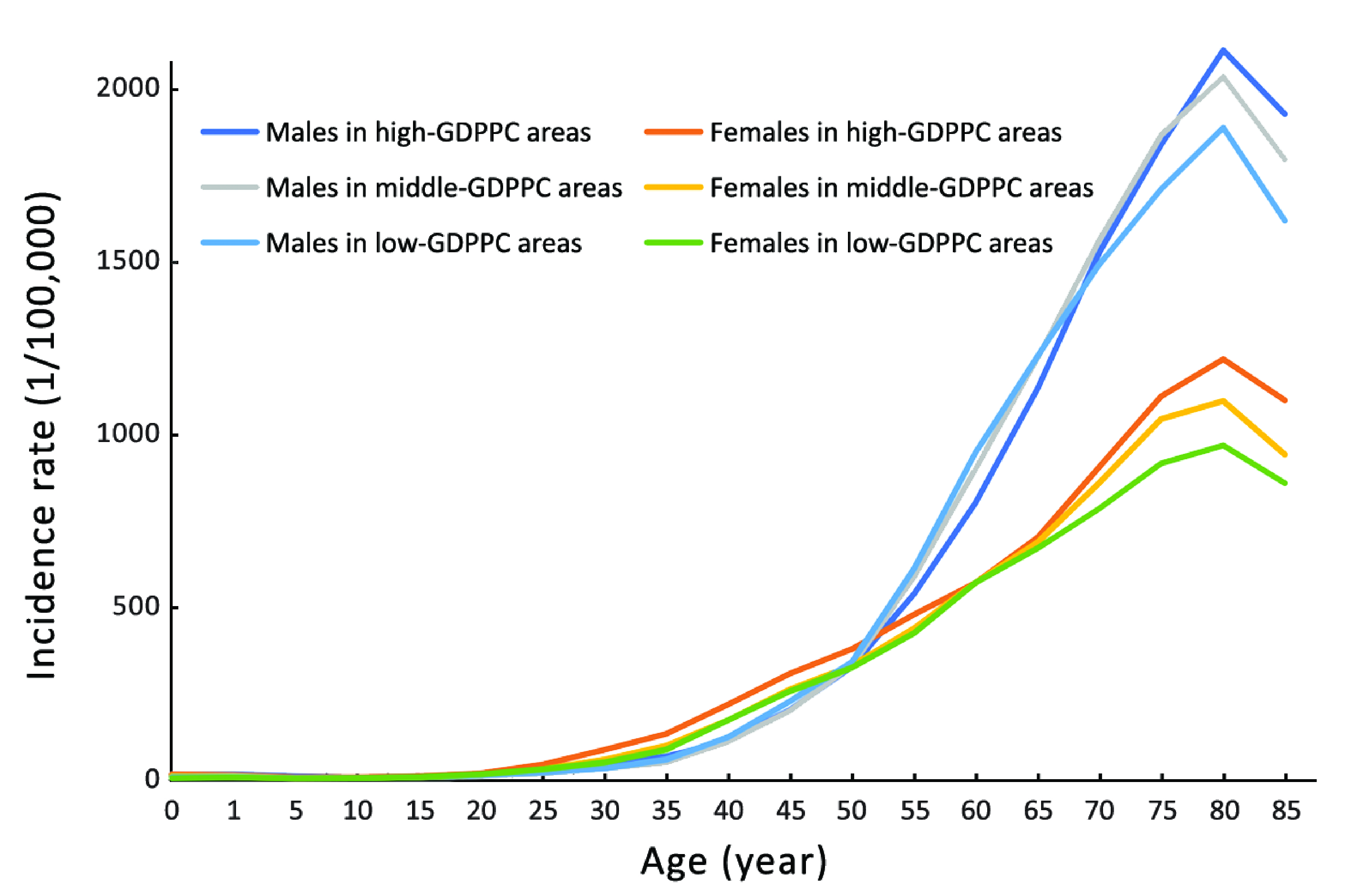
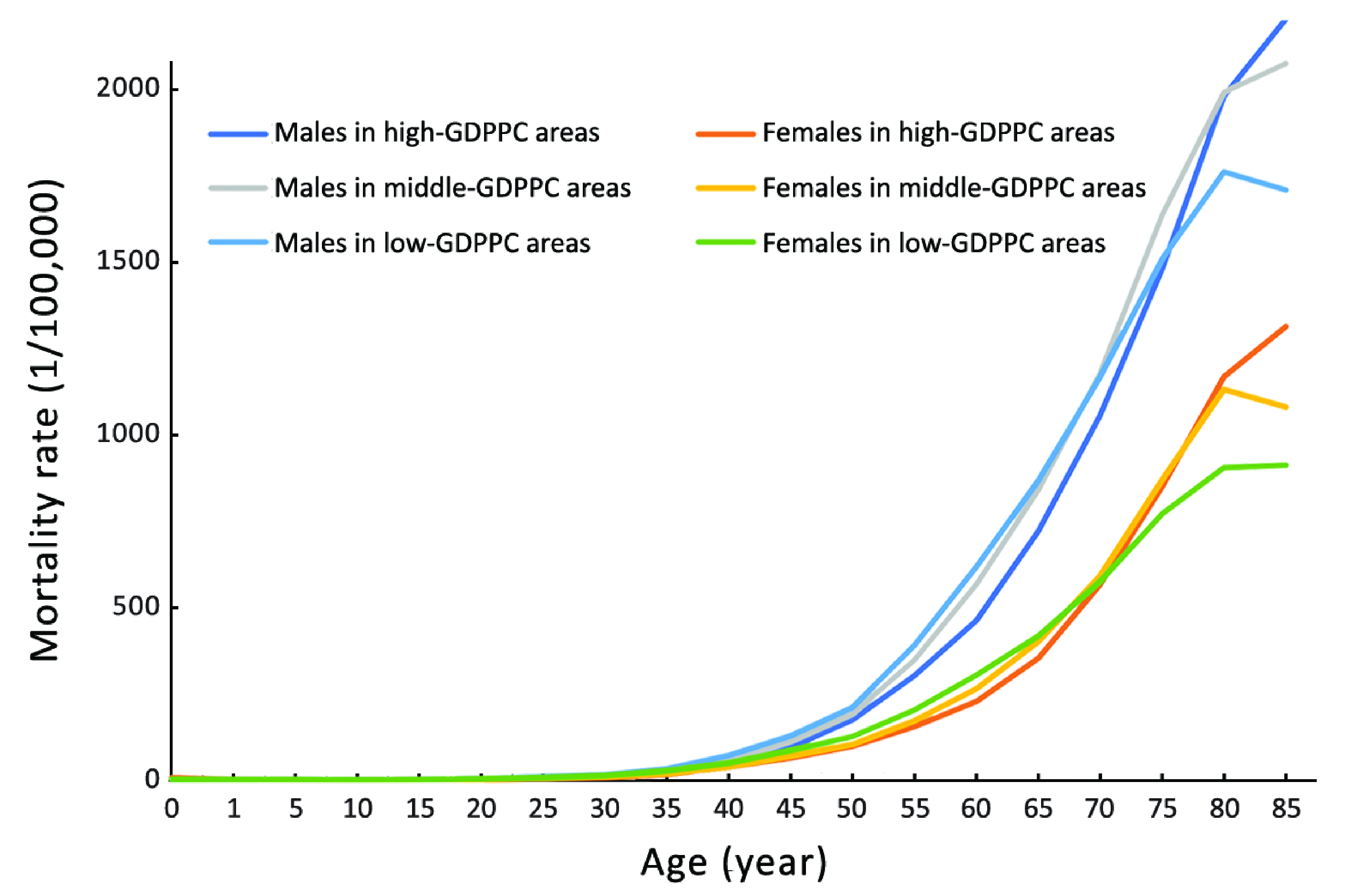
Objective In this research, the patterns of cancer incidence and mortality in areas with different gross domestic product per capita (GDPPC) levels in China were explored, using data from population-based cancer registries in 2013, collected by the National Central Cancer Registry (NCCR). Methods Data from 255 cancer registries were qualified and included in this analysis. Based on the GDPPC data of 2014, cities/counties were divided into 3 levels: high-, middle- and low-GDPPC areas, with 40,000 and 80,000 RMB per year as cut points. We calculated cancer incidences and mortalities in these three levels, stratified by gender and age group. The national population of the Fifth Census in 2000 and Segi’s population were applied for age-standardized rates. Results The crude incidence and mortality rates as well as age-standardized incidence rate (ASIR) showed positive associations with GDPPC level. The age-standardized mortality rate (ASMR) nevertheless showed a negative association with GDPPC level. The ASMR in high-, middle- and low-GDPPC areas was 103.12/100,000, 112.49/100,000 and 117.43/100,000, respectively. Lung cancer was by far the most common cancer in all three GDPPC levels. It was also the leading cause of cancer death, regardless of gender and GDPPC level. Negative associations with GDPPC level were found for the ASIRs of lung, stomach, esophageal and liver cancer, whereas colorectal and breast cancer showed positive associations. Except for breast cancer, the ASMRs of the other five cancers were always higher in middle- and low-GDPPC areas than in high-GDPPC areas. Conclusions The economic development is one of the main factors of the heavy cancer burden on Chinese population. It would be reasonable to implement cancer control strategies referring to the local GDPPC level.
2017, 29(5): 395-401.
doi: 10.21147/j.issn.1000-9604.2017.05.03
Abstract:
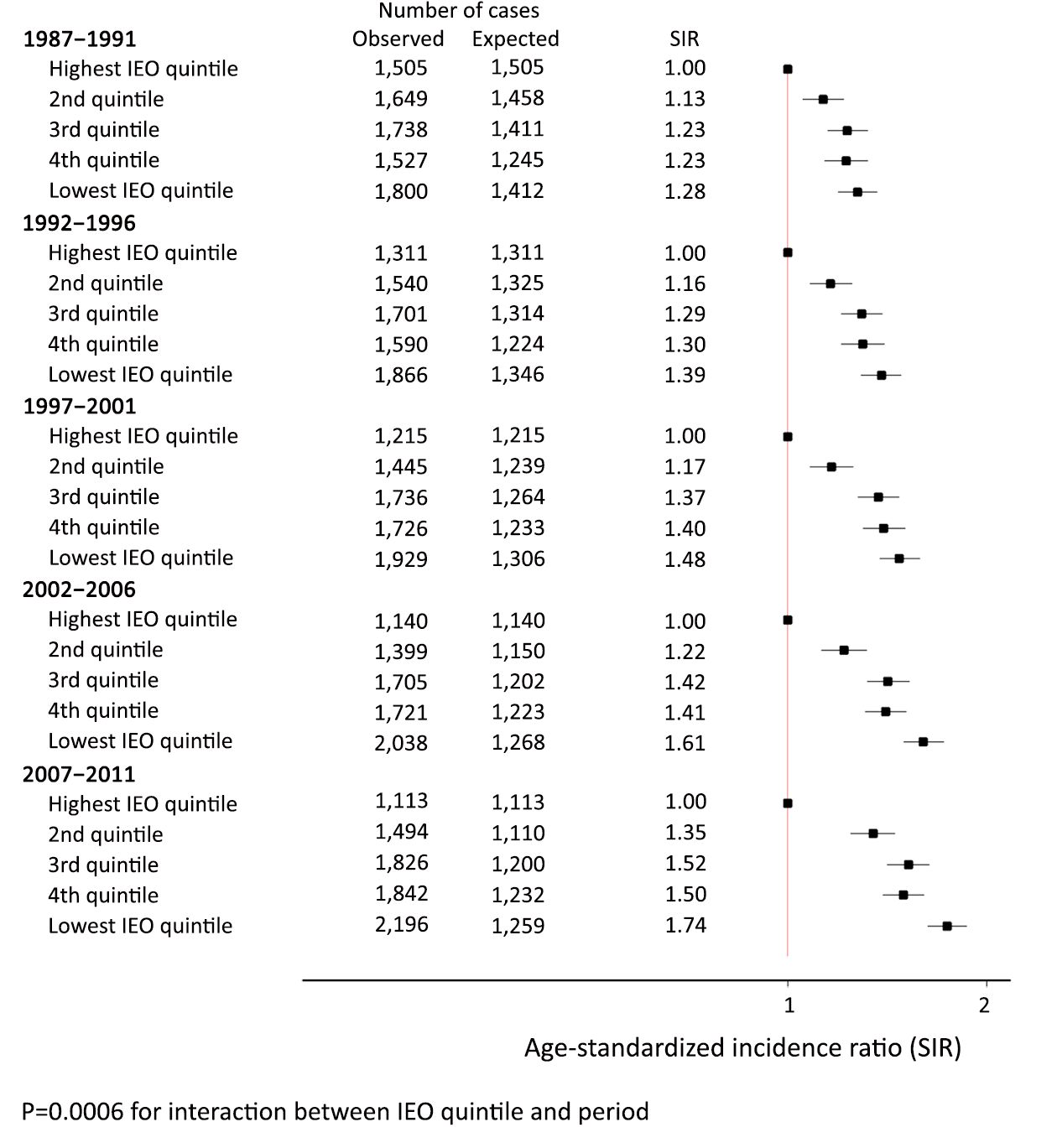
Objective We assessed the trends in lung cancer incidence over a 25-year period by socioeconomic groups for men in New South Wales (NSW), Australia. Methods Men diagnosed with lung cancer between 1987 and 2011 were divided into five quintiles according to an Index of Education and Occupation (IEO). We assessed relative socioeconomic differences over time by calculating age-standardized incidence ratios (SIRs) by 5-year period of diagnosis, and estimated absolute differences by comparing the observed and expected numbers of cases using the highest IEO quintile as the reference. Results Lung cancer incidence for men decreased from 1987 to 2011 for all IEO quintiles, with a greater rate of decline for men living in the highest IEO areas. Thus, the relative disparity increased significantly over the 25-year period (P=0.0006). For example, the SIR for the lowest IEO quintile increased from 1.28 during 1987–1991 to 1.74 during 2007–2011. Absolute differences also increased with the proportion of " potentially preventable” cases doubling from 14.5% in 1987–1991 to 30.2% in 2007–2011. Conclusions Despite the overall decline in lung cancer incidence among men in NSW over the past 25 years, there was a significant increase in disparity across socioeconomic areas in both relative and absolute terms.

2017, 29(5): 402-410.
doi: 10.21147/j.issn.1000-9604.2017.05.04
Abstract:
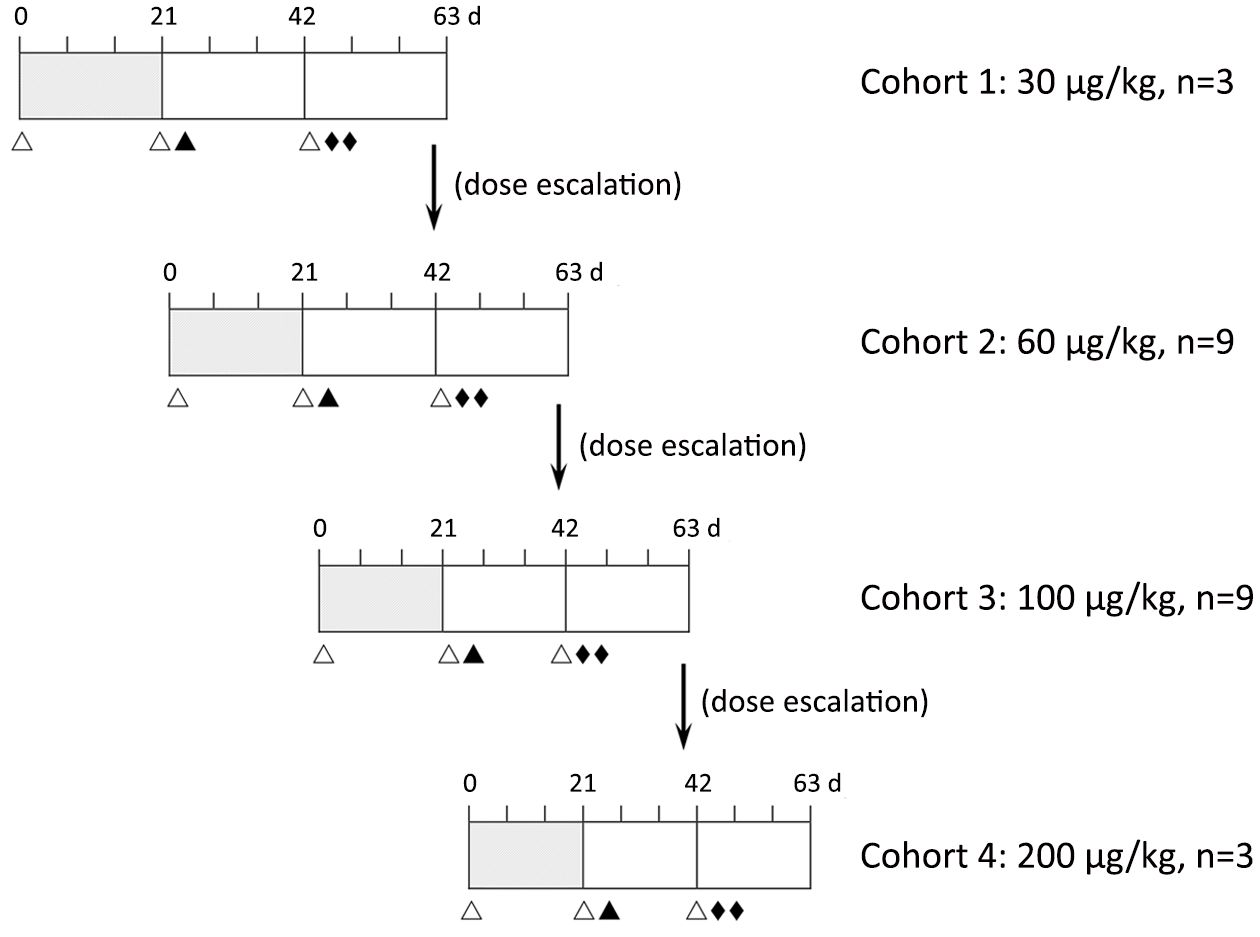
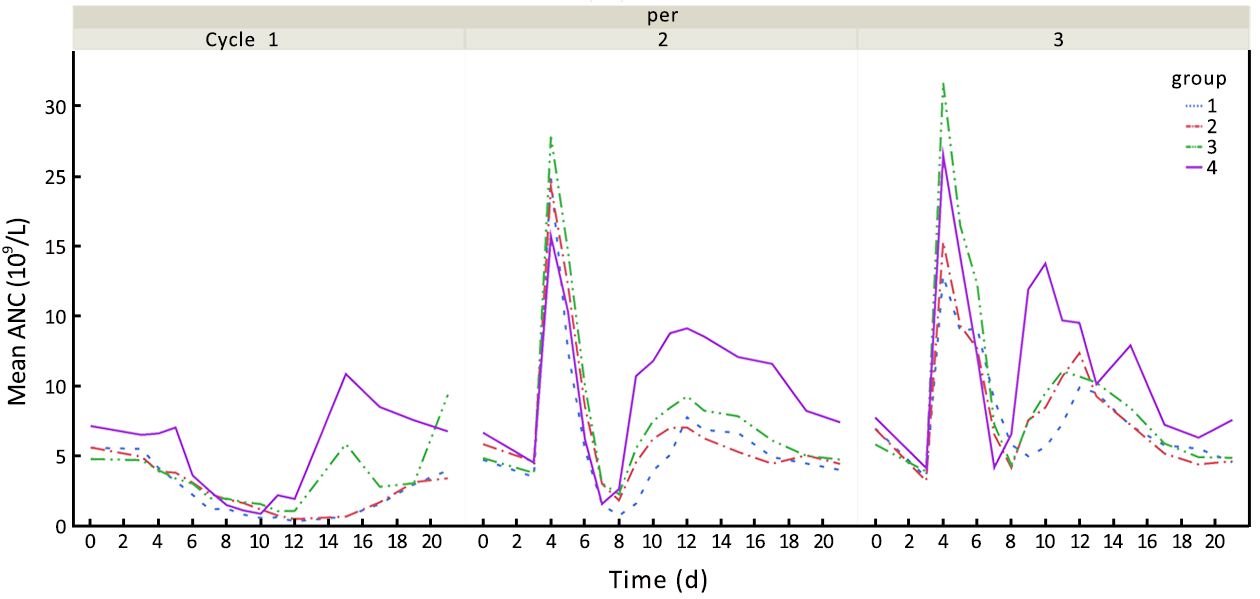
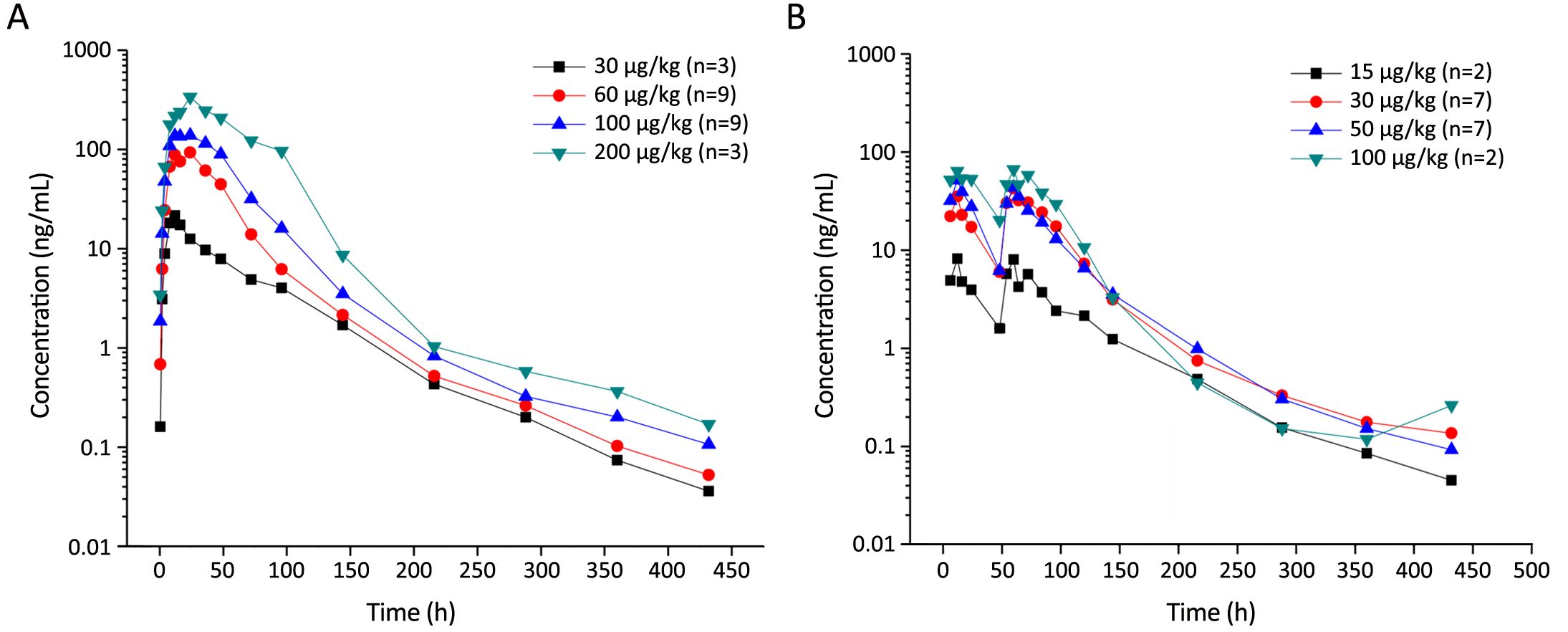
Objective The recommended dose of prophylactic pegylated recombinant human granulocyte-colony stimulating factor (PEG rhG-CSF) is 100 μg/kg once per cycle for patients receiving intense-dose chemotherapy. However, few data are available on the proper dose for patients receiving less-intense chemotherapy. The aim of this phase I study is to explore the proper dose and administration schedule of PEG rhG-CSF for patients receiving standard-dose chemotherapy. Methods Eligible patients received 3-cycle chemotherapy every 3 weeks. No PEG rhG-CSF was given in the first cycle. Patients experienced grade 3 or 4 neutropenia would then enter the cycle 2 and 3. In cycle 2, patients received a single subcutaneous injection of prophylactic PEG rhG-CSF on d 3, and received half-dose subcutaneous injection in cycle 3 on d 3 and d 5, respectively. Escalating doses (30, 60, 100 and 200 μg/kg) of PEG rhG-CSF were investigated. Results A total of 26 patients were enrolled and received chemotherapy, in which 24 and 18 patients entered cycle 2 and cycle 3 treatment, respectively. In cycle 2, the incidence of grade 3 or 4 neutropenia for patients receiving single-dose PEG rhG-CSF of 30, 60, 100 and 200 μg/kg was 66.67%, 33.33%, 22.22% and 0, respectively, with a median duration less than 1 (0–2) d. No grade 3 or higher neutropenia was noted in cycle 3 in all dose cohorts. Conclusions The pharmacokinetic and pharmacodynamic profiles of PEG rhG-CSF used in cancer patients were similar to those reported, as well as the safety. Double half dose administration model showed better efficacy result than a single dose model in terms of grade 3 neutropenia and above. The single dose of 60 μg/kg, 100 μg/kg and double half dose of 30 μg/kg were recommended to the phase II study, hoping to find a preferable method for neutropenia treatment.
2017, 29(5): 411-418.
doi: 10.21147/j.issn.1000-9604.2017.05.05
Abstract:
Objective Chemotherapy with paclitaxel is associated with significant neurotoxicity that may offset patients’ quality of life and therapeutic benefits. This prospective, non-randomized control study evaluated the efficacy and safety of an antidepressant drug, duloxetine, at 30 or 60 mg/d, in the treatment of paclitaxel-induced peripheral neuropathy (PIPN) in Chinese breast cancer patients. Methods A total of 102 patients with a median age of 50 (range, 25–60) years, treated in the Department of Medical Oncology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, between November 2014 and January 2017 were finally enrolled. Stratified by baseline characteristics, the patients were classified into two groups, receiving either duloxetine or alternative anti-neurotoxicity drugs. During the course of the paclitaxel regimen, the eligibility criteria included sensory neuropathy, as evaluated by the National Cancer Institute-Common Toxicity Criteria for Adverse Events. The treatment consisted of receiving 30 mg duloxetine (for the first 4 weeks) and 60 mg duloxetine for an additional 8 weeks, or any other anti-neurotoxicity drug daily during the same crossover period. The improvement associated with PIPN from the patient’s perspective were assessed by the Functional Assessment of Cancer Therapy-Taxane (FACT-Tax) Scales, which contained questions scored from 0 to 4 (0, not at all; 4, very much; total score range, 0–44). Results Duloxetine was more effective in decreasing PIPN (odds ratio=5.426; 95% confidence interval, 1.898–15.514; P=0.002). Between duloxetine group and control group, the median (25th–75th percentiles) decreasing difference in the FACT-Tax pain score was 4 (2–6) vs. 1 (0–4) (P=0.005). Conclusions Duloxetine is a promising and safe option with tolerable toxicity at a dose of 60 mg/d for Chinese breast cancer patients with PIPN. Non-neuropathy adverse events were mild and similar in both groups. The major toxicities of duloxetine included nausea, constipation, somnolence, dizziness and distention of the eyes. Further examination of the benefits of duloxetine in the prevention of PIPN is required.

2017, 29(5): 419-425.
doi: 10.21147/j.issn.1000-9604.2017.05.06
Abstract:
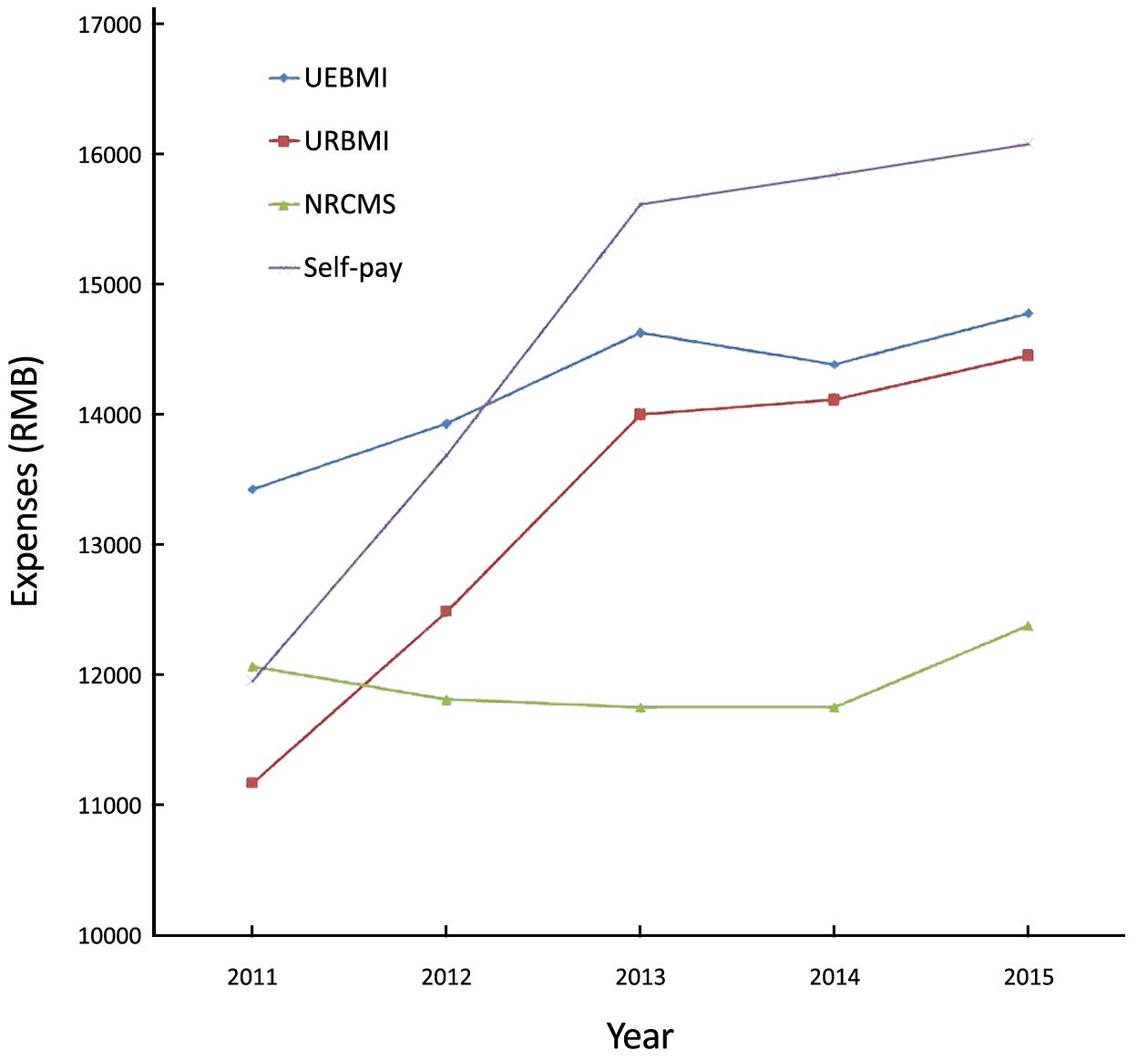
Objective An understanding of the levels and trends of medical cost is made for breast cancer patients with different medical insurance coverages in China (mainland), in an attempt to offer a clue to further control the costs. Methods The inpatient payments of 9,716,180 breast cancer patients spent in medical institutions of different types and grades during 2011–2015 were collected from the inpatient medical record home page (IMRHP) dataset. The data were then processed with SAS (Version 9.3; SAS Institute, Cary, NC, USA). Indicators like means, increase (decrease) percentages were used to descriptively analyze the average hospitalization expense of each time (AHEET) and its trends of breast cancer patients with different medical insurance coverages treated in medical institutions of different types and grades. Results In 2011–2015, the AHEET borne by breast cancer patients in China had been constantly increasing. Specifically, the self-pay inpatients had the largest increase, inpatients covered by Urban Employee Basic Medical Insurance (UEBMI) and Urban Resident Basic Medical Insurance (URBMI) were the next, and those covered by New Rural Cooperative Medical System (NRCMS) had the least increase. Breast cancer inpatient treated in public hospitals had quite greater increase and higher expenditure level than those in private hospitals. The AHEET borne by the inpatients in Grade 3 hospitals had greater increase and higher cost than those in Grade 2 hospitals. Conclusions The inpatient payments of breast cancer patients will be wisely controlled by reducing the number of self-pay inpatients, taking advantage of restriction mechanism of the medical insurances, and promoting healthy competition between private hospitals and public hospitals. The economic burden imposed on the society by breast cancer can be relieved through further control of inpatient payments of UEBMI- and URBMI-covered breast cancer patients and of Grade 3 hospitals.
2017, 29(5): 426-437.
doi: 10.21147/j.issn.1000-9604.2017.05.07
Abstract:
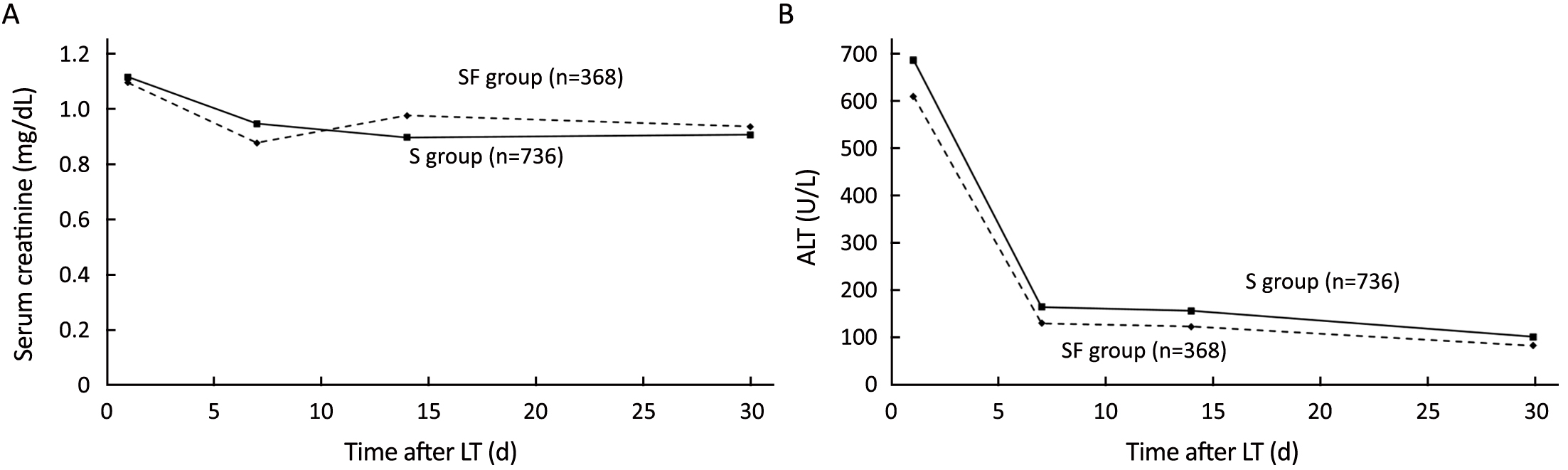
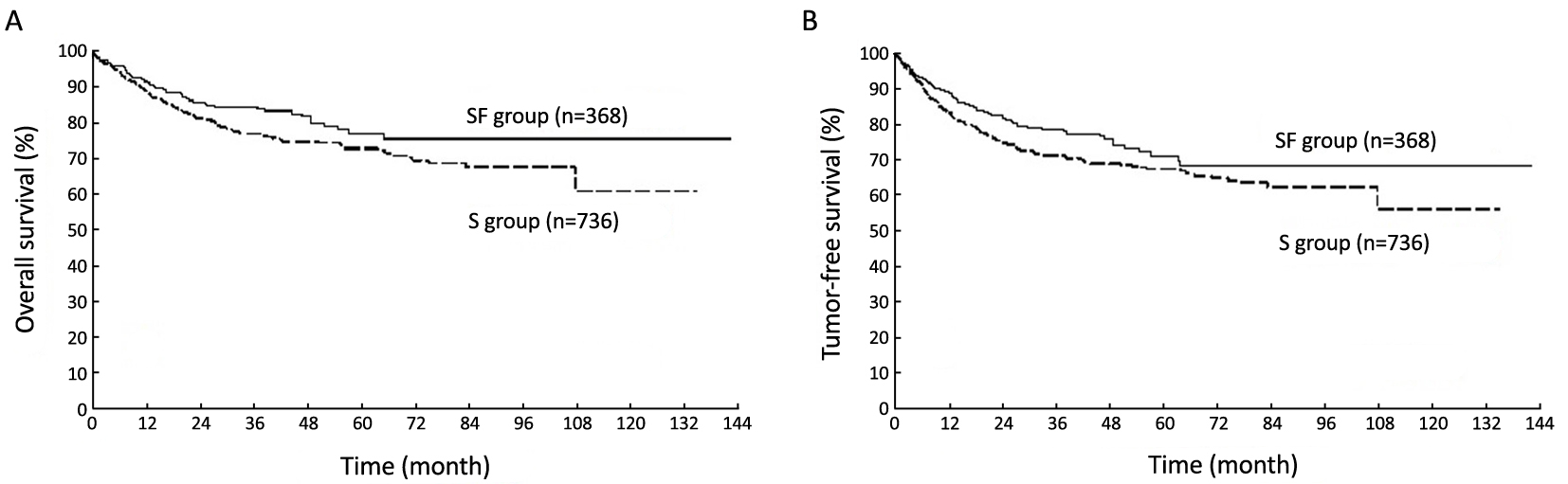
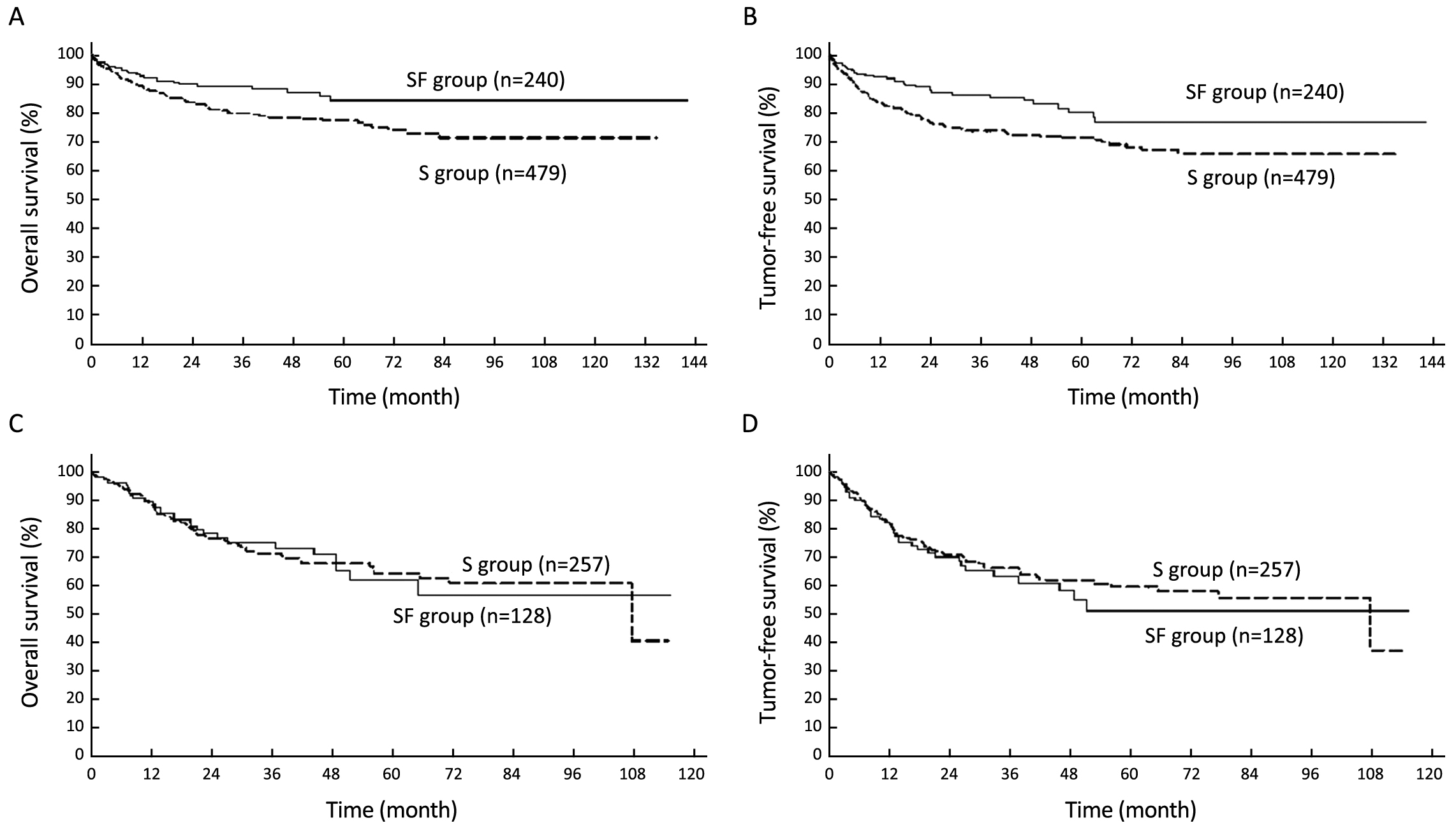
Objective We aimed to evaluate the efficacy and safety of steroid-free immunosuppression after liver transplantation (LT) for hepatocellular carcinoma (HCC). Methods We retrospectively analyzed HCC recipients without steroids after LT (SF group, n=368) based on the China Liver Transplant Registry (CLTR) database. These recipients were matched 1:2 with patients using steroids (S group, n=736) for the same period after LT for HCC, according to propensity scores. Results Multivariate analysis indicates that recipients with younger age [odds ratio (OR), 1.053; P=0.011], preoperative hepatitis B virus (HBV) DNA ≥1,000 copies/mL (OR, 2.597; P=0.004) and beyond Milan criteria (OR, 4.255; P<0.001) were identified as the risk factors associated with tumor recurrence in steroid avoidance recipients after LT. The patients fulfilling the Milan criteria in the SF group presented higher overall and tumor-free survival rates than those in the S group (P<0.05). Multivariate analysis revealed that recipient beyond Milan criteria was an independent prognostic factor for overall survival (OR, 1.690; P<0.001) and tumor-free survival (OR, 2.066; P<0.001). The incidences of new-onset diabetes mellitus (21.20% vs. 33.29%, P<0.001), new-onset hypertension (10.05% vs. 18.61%, P<0.001) and hyperlipidemia (4.08% vs. 7.20%, P=0.042) were significantly lower in the SF group. Conclusions Steroid-free immunosuppression could be safe and feasible for HBV-related HCC patients in LT. Age, HBV DNA level and Milan criteria maybe risk factors associated with tumor recurrence in steroid avoidance recipients. Recipient beyond Milan criteria was an independent prognostic factor and recipient fulfilling Milan criteria can benefit the most from steroid-free immunosuppression.
2017, 29(5): 438-446.
doi: 10.21147/j.issn.1000-9604.2017.05.08
Abstract:
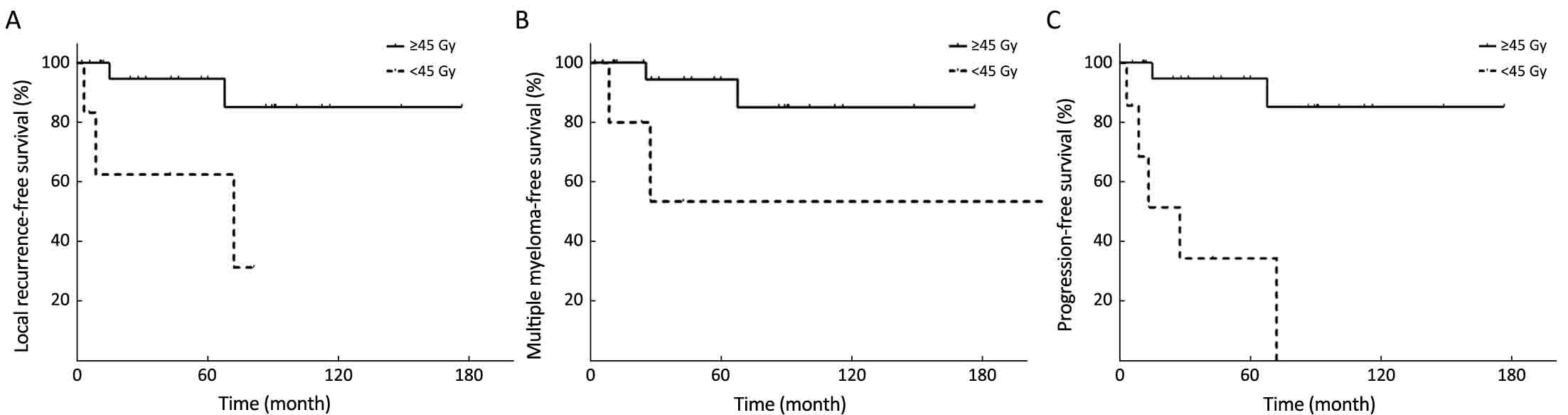
Objective To investigate potential prognostic factors affecting patient outcomes and to evaluate the optimal methods and effects of radiotherapy (RT) in the management of extramedullary plasmacytoma (EMP). Methods Data from 55 patients with EMP between November 1999 and August 2015 were collected. The median age was 51 (range, 22–77) years. The median tumor size was 3.5 (range, 1.0–15.0) cm. The median applied dose was 50.0 (range, 30.0–70.0) Gy. Thirty-nine patients (70.9%) presented with disease in the head or neck region. Twelve patients received RT alone, 9 received surgery (S) alone, 3 received chemotherapy (CT) alone, and 3 patients did not receive any treatment. Combination therapies were applied in 28 patients. Results The median follow-up duration was 56 months. The 5-year local recurrence-free survival (LRFS), multiple myeloma-free survival (MMFS), progression-free survival (PFS) and overall survival (OS) rates were 79.8%, 78.6%, 65.2% and 76.0%, respectively. Univariate analysis revealed that RT was a favourable factor for all examined endpoints. Furthermore, head and neck EMPs were associated with superior LRFS, MMFS and PFS. Tumor size <4 cm was associated with superior MMFS, PFS and OS; serum M protein negativity was associated with superior MMFS and PFS; age ≥50 years and local recurrence were associated with poor MMFS. The dose ≥45 Gy group exhibited superior 5-year LRFS, MMFS and PFS rates (94.7%, 94.4%, 90.0%, respectively), while the corresponding values for the dose <45 Gy group were 62.5% (P=0.008), 53.3% (P=0.036) and 41.7% (P<0.001). Conclusions Involved-site RT of at least 45 Gy should be considered for EMP. Furthermore, patients with head and neck EMP, tumor size <4 cm, age <50 years and serum M protein negativity had better outcomes.
2017, 29(5): 447-454.
doi: 10.21147/j.issn.1000-9604.2017.05.09
Abstract:
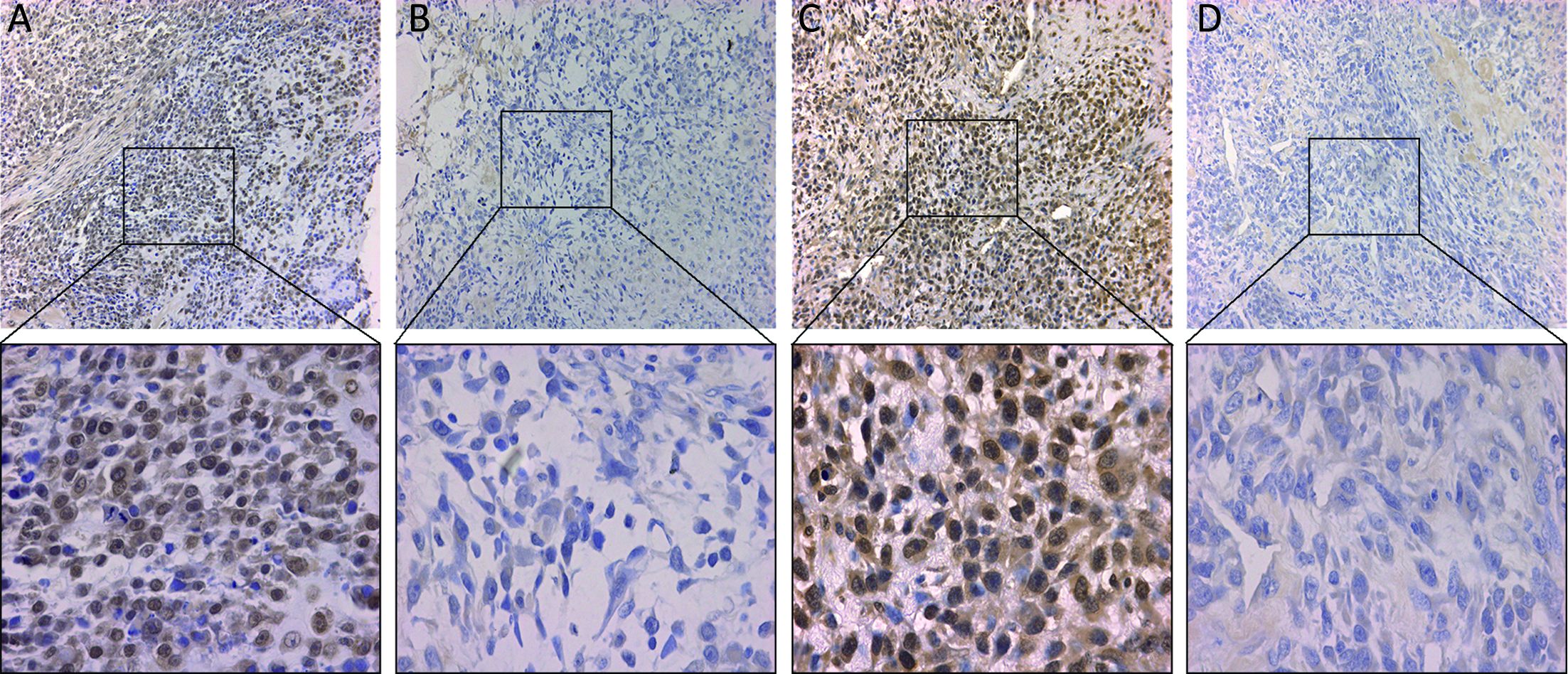
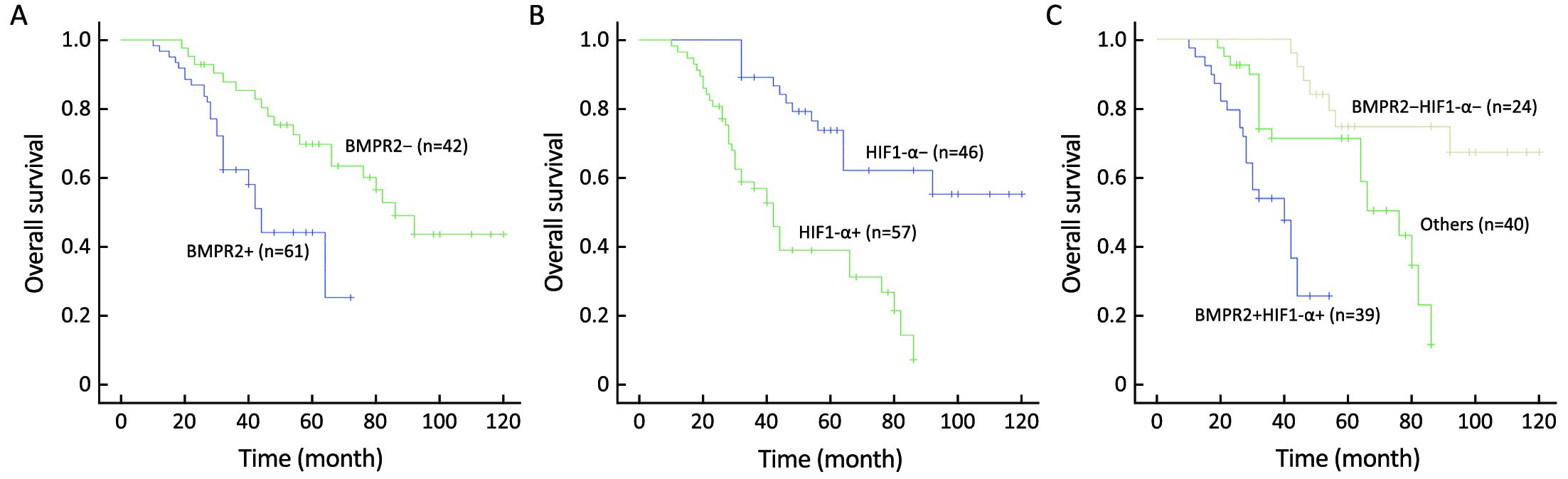
Objective Bone morphogenetic protein receptor 2 (BMPR2) and hypoxia-inducible factor 1-α (HIF1-α) existed abnormal expression in several types of cancer. However, their expressions and related roles in osteosarcoma are largely unknown. Methods To investigate the clinical significance of BMPR2 and HIF1-α in osteosarcoma, we analyzed their expression levels in 103 osteosarcoma specimens by immunochemistry. Meanwhile, we conducted a follow-up to examine the metastatic behavior and overall survival (OS) of osteosarcoma patients. Results Among 103 tissues, 61 cases had BMPR2-positive expression and 57 cases had HIF1-α positive expression. A significant correlation was noticed between BMPR2 and HIF1-α expression in osteosarcoma specimens (P=0.035). Receiver-operating characteristic (ROC) curves were calculated to investigate the predictive value of the two markers in tumor metastasis. By means of univariate and multivariate analysis, BMPR2 and HIF1-α expression, as well as higher tumor grade, were identified as significant risk factors for OS in patients with osteosarcoma. Kaplan-Meier survival analysis revealed that the patients with BMPR2 and HIF1-α positive expression had worse OS compared with patients with BMPR2-negative or HIF1-α-negative staining. Conclusions It can be concluded that BMPR2 and HIF1-α expression is highly correlated with metastatic behavior in patients with osteosarcoma and can serve as predictive markers for metastasis and OS of these patients.
2017, 29(5): 455-462.
doi: 10.21147/j.issn.1000-9604.2017.05.10
Abstract:
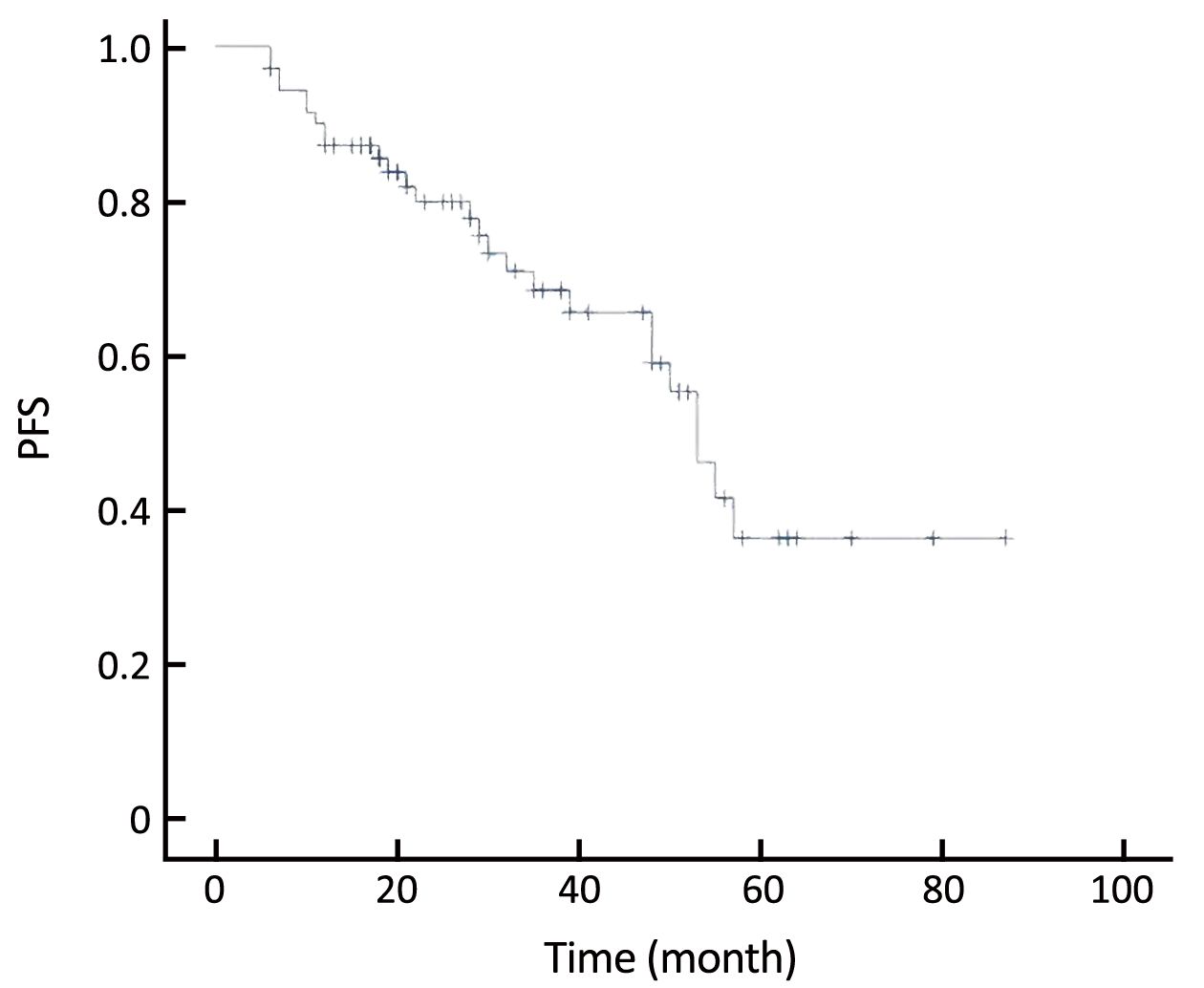
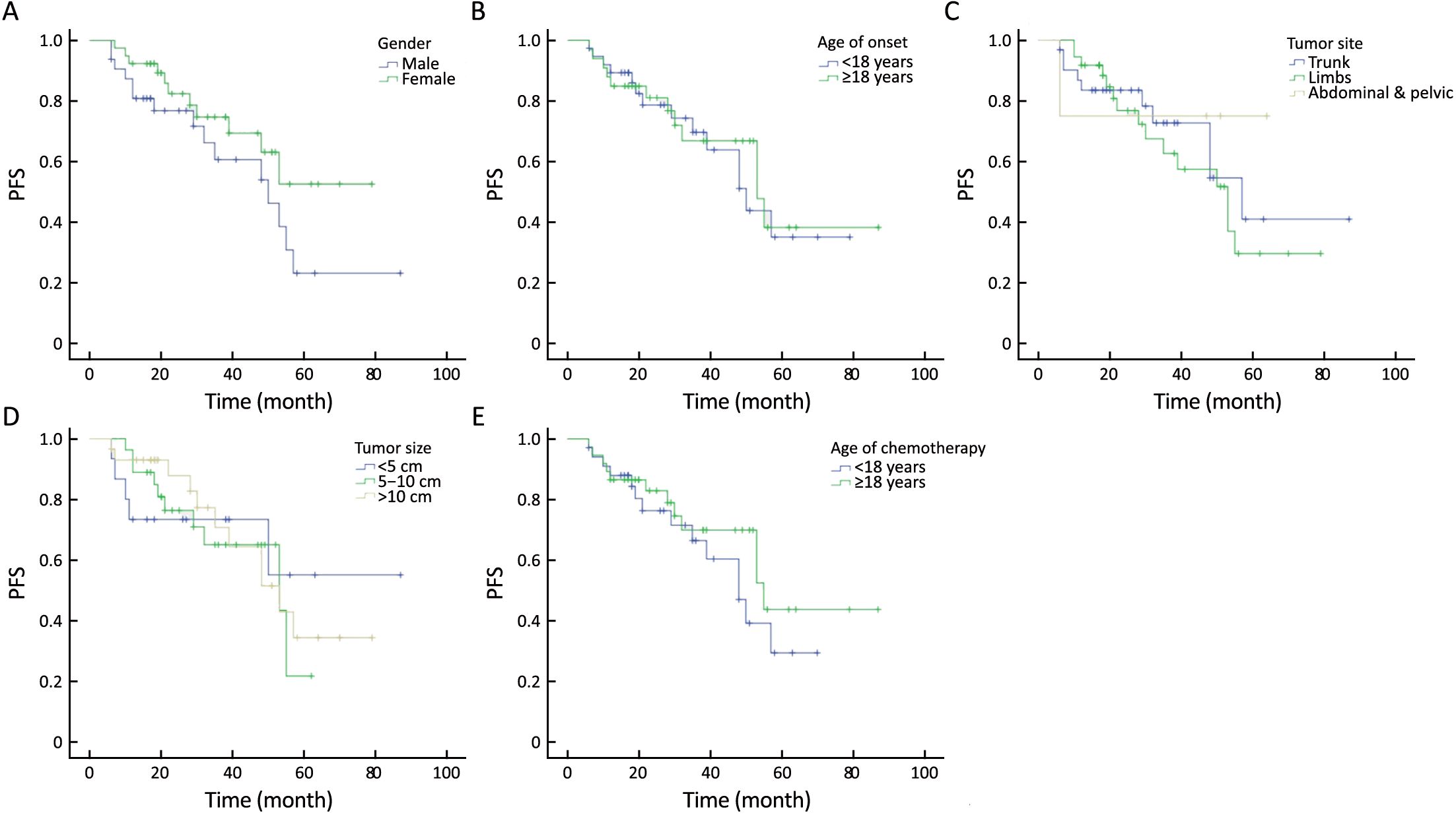
Objective To assess the efficacy of conservative chemotherapy for inoperable desmoid tumor (DT) and analyze the prognostic factors. Methods From November 2008 to April 2016, 71 patients of inoperable DT were treated with vinorelbine and low-dose methotrexate in the Department of Bone and Soft Tissue Tumors, Peking University Cancer Hospital & Institute, and enrolled in this retrospective study. The chemotherapy duration is one year. The efficacy of chemotherapy and the prognosis were observed. Results Of the 71 patients, 55% were female. Age of onset varied from 1 to 47 years, and the median age was 14 years. Only 11 (15.5%) cases suffered primary tumor. The distribution of the site of tumors was: 31 (43.7%) in the trunk, 36 (50.7%) in the limbs, and 4 (5.6%) in the peritoneal and pelvic cavity. The size of tumor (the maximum diameter) differed from 2 to 37 cm with a mean of 9.3 cm. The median follow-up duration was 28 (range, 6–87) months. Common side effects included: nausea and vomiting, liver injury, bone marrow suppression and oral ulcers. When the chemotherapy finished, 1 (1.4%) case achieved complete response, 24 (33.8%) achieved partial response, 37 (52.1%) achieved stable disease and 9 (12.7%) had progressive disease. The overall response rate was 87.3%. The progression-free survival (PFS) of the participants were from 6 to 87 months, and the 2-, 3- and 5-year PFS was 79.9%, 68.4% and 36.3%, respectively. No significant difference was identified in PFS in subgroups of gender, age of onset, age of chemotherapy, tumor site and tumor size. Conclusions For recurrent, inoperable and progressive DT, enough course of chemotherapy with vinorelbine combined with low-dose methotrexate was an optional choice for local control.

2017, 29(5): 463-470.
doi: 10.21147/j.issn.1000-9604.2017.05.11
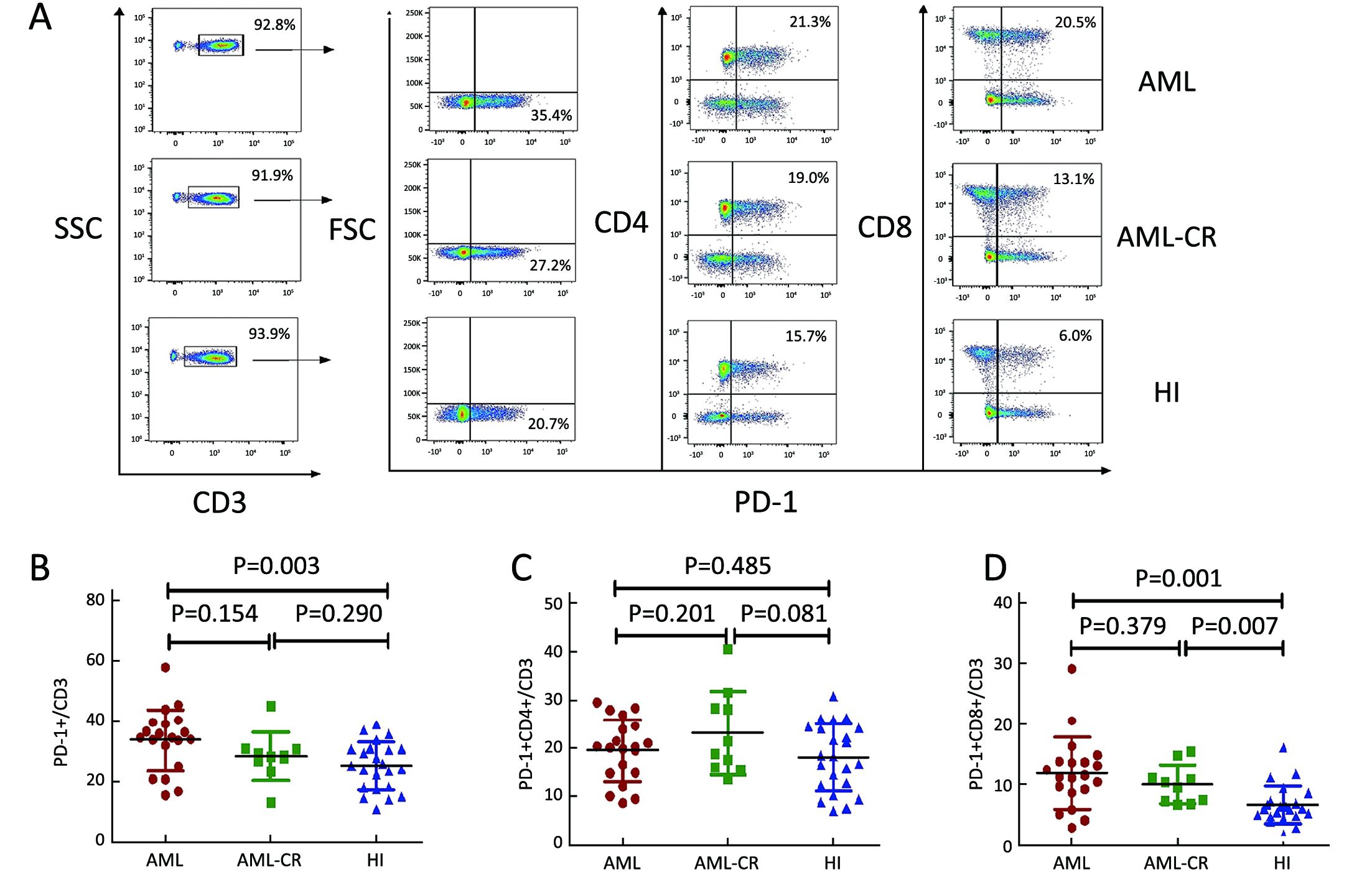
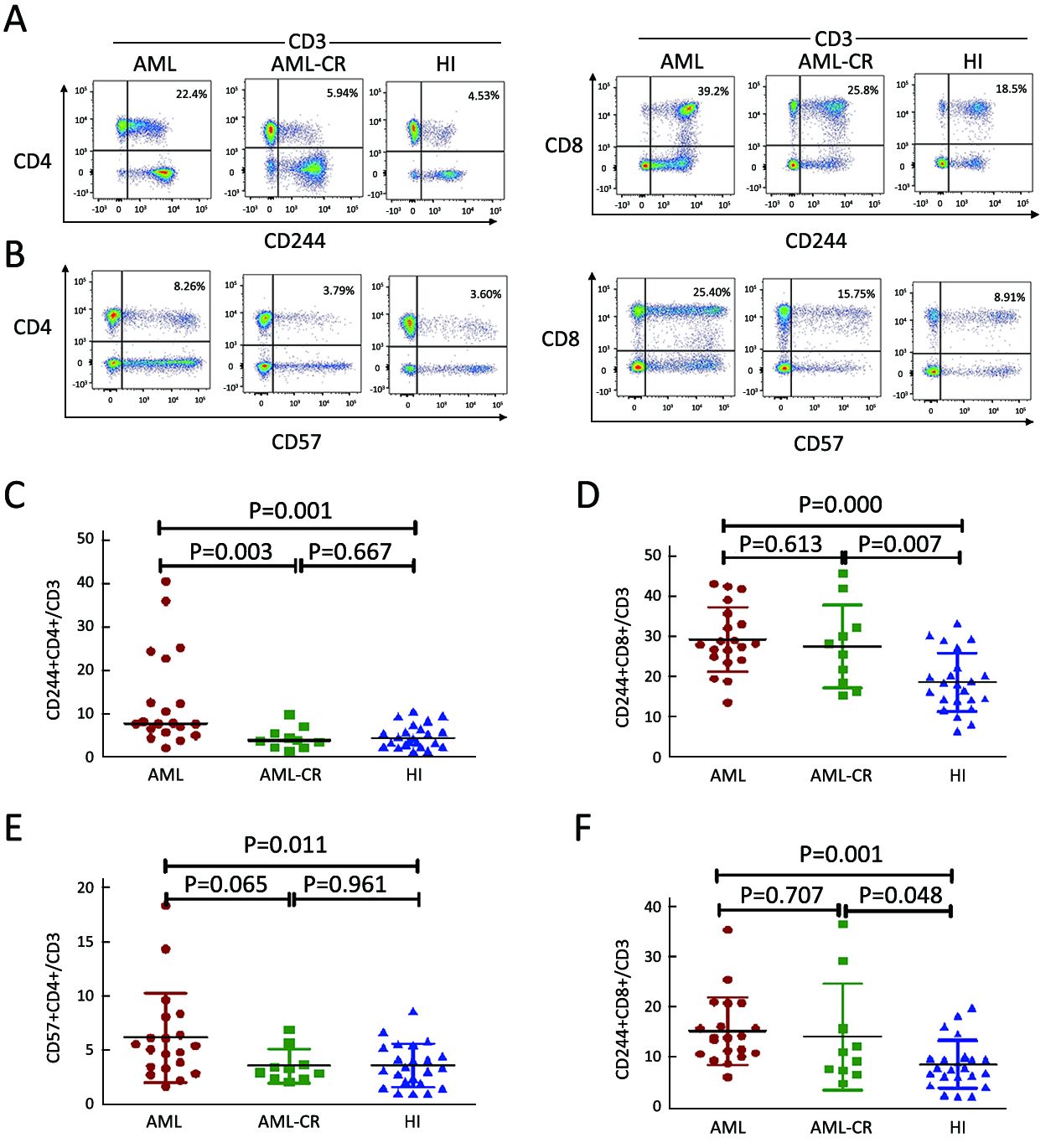
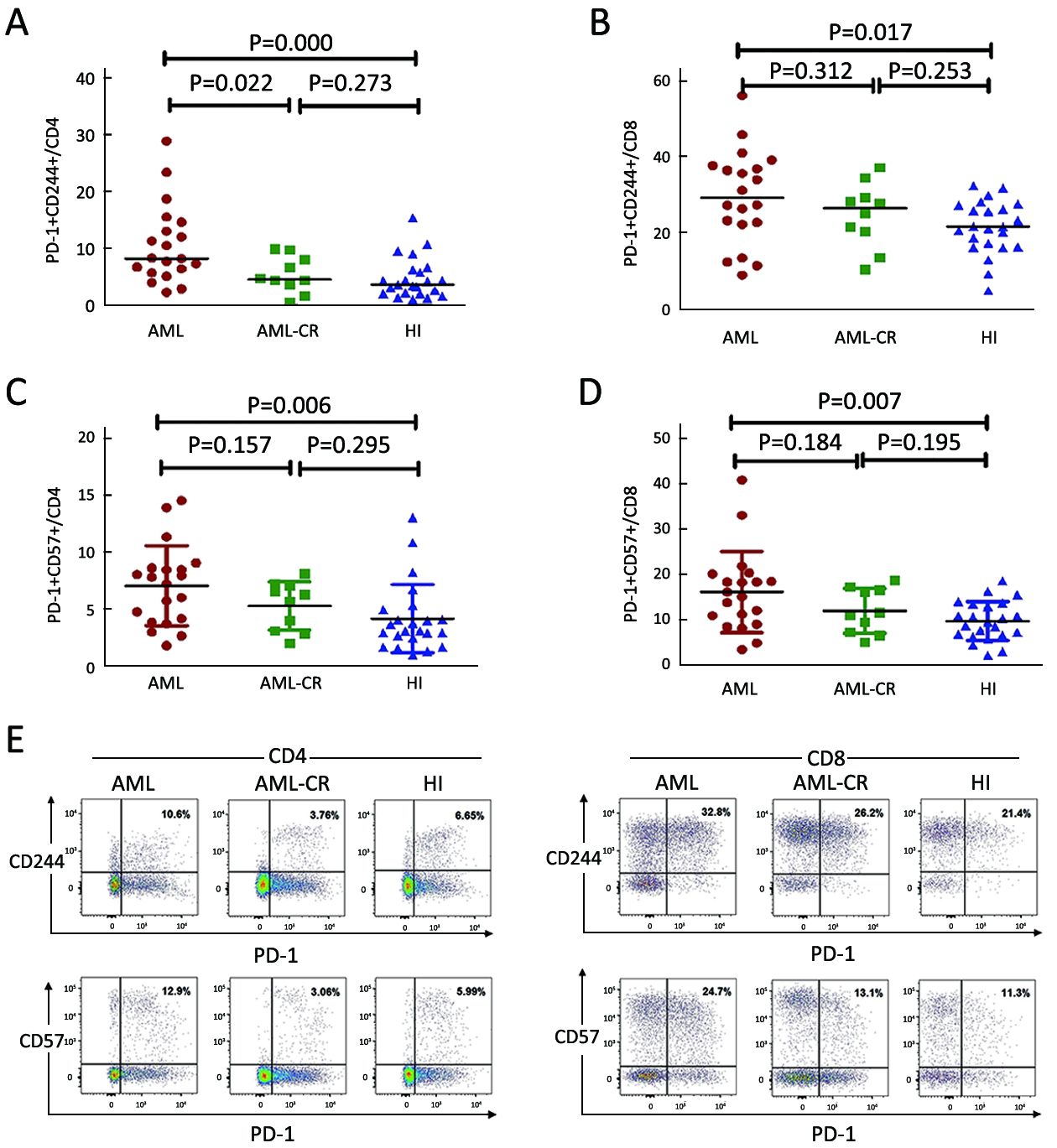
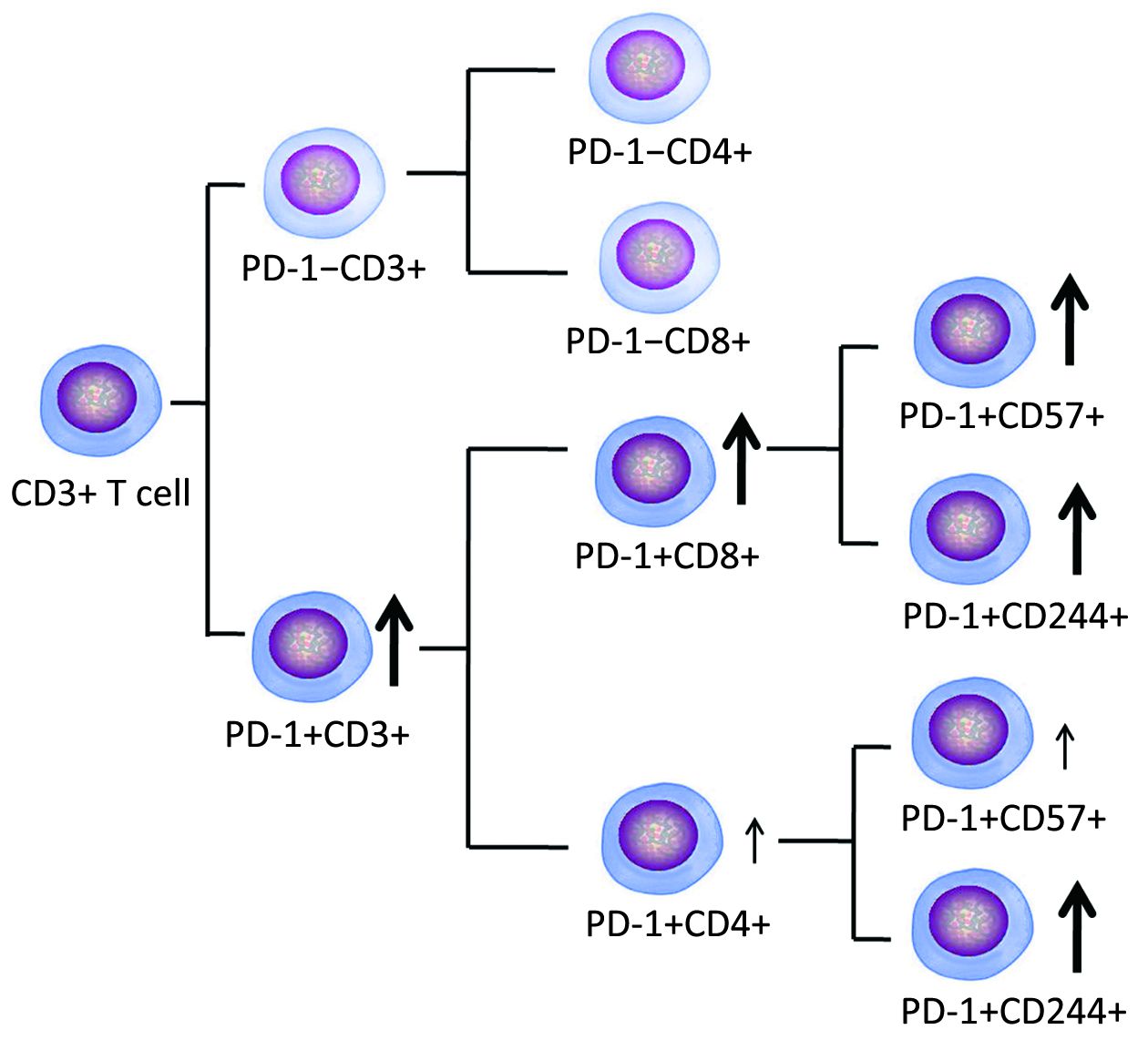
Abstract:
Objective To investigate the association between the T cell inhibitory receptor programmed death 1 (PD-1) and T cell exhaustion status in T cells from patients with de novo acute myeloid leukemia (AML) and AML in complete remission (CR). Methods Surface expression of PD-1 and the exhaustion and immunosenescence markers CD244 and CD57 on CD3+, CD4+ and CD8+ T cells from peripheral blood samples from 20 newly diagnosed, untreated AML patients and 10 cases with AML in CR was analyzed by flow cytometry. Twenty-three healthy individuals served as control. Results A significantly higher percentage of PD-1+ cells were found for CD3+ T cells in the de novo AML group compared with healthy controls. In addition, an increased level of PD-1+CD8+ T cells, but not PD-1+CD4+, was found for CD3+ T cells in the de novo AML and AML-CR samples. A higher percentage of CD244+CD4+, CD244+CD8+, CD57+CD4+ and CD57+CD8+ T cells was found in CD3+ T cells in samples from those with de novo AML compared with those from healthy controls. Strong increased PD-1+CD244+ and PD-1+CD57+ co-expression was found for CD4+ and CD8+ T cells in the de novo AML group compared with healthy controls. Conclusions We characterized the major T cell defects, including co-expression of PD-1 and CD244, CD57-exhausted T cells in patients with de novo AML, and found a particular influence on CD8+ T cells, suggesting a poor anti-leukemia immune response in these patients.