
2018 Vol.30(5)
Display Mode: |
2018, 30(5): 477-496.
doi: 10.21147/j.issn.1000-9604.2018.05.01
 Abstract
Abstract FullText HTML
FullText HTML PDF 2150KB
PDF 2150KB
Abstract:
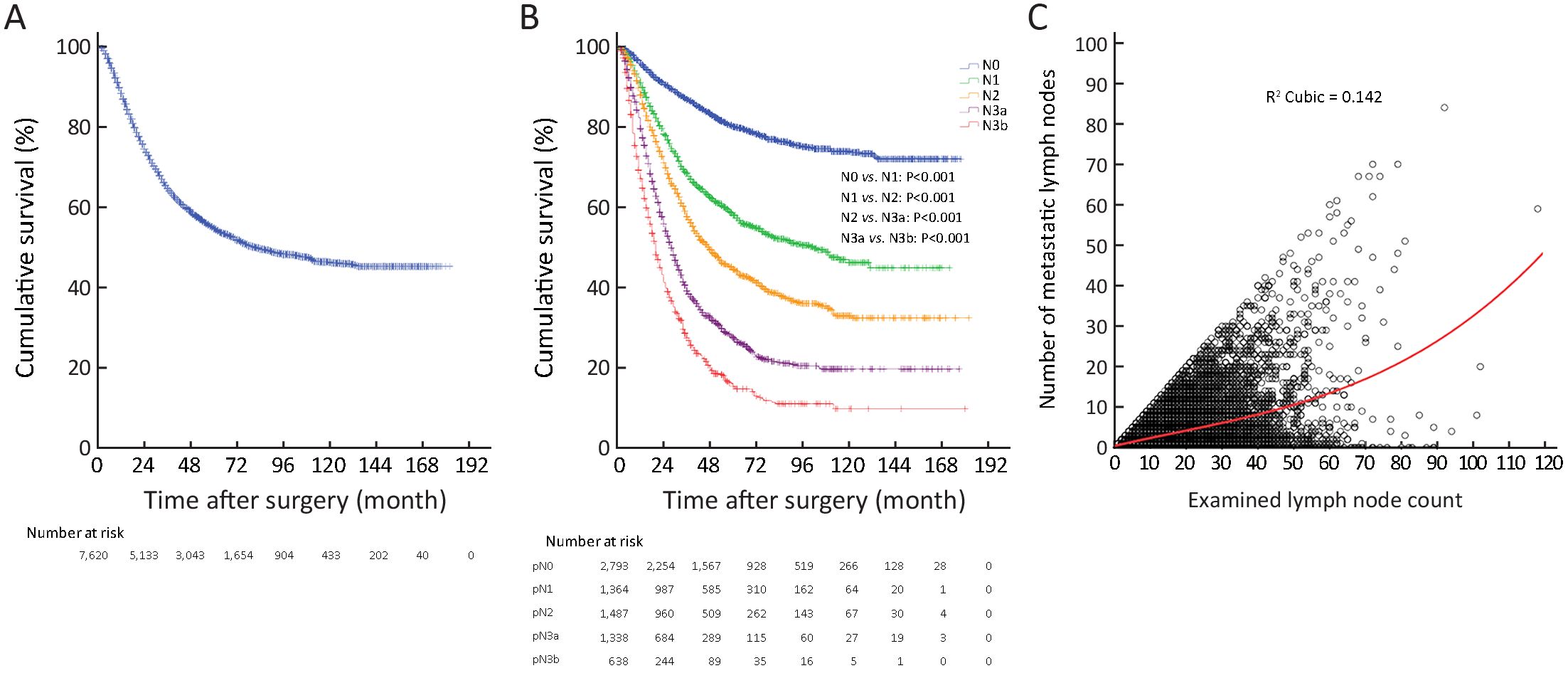
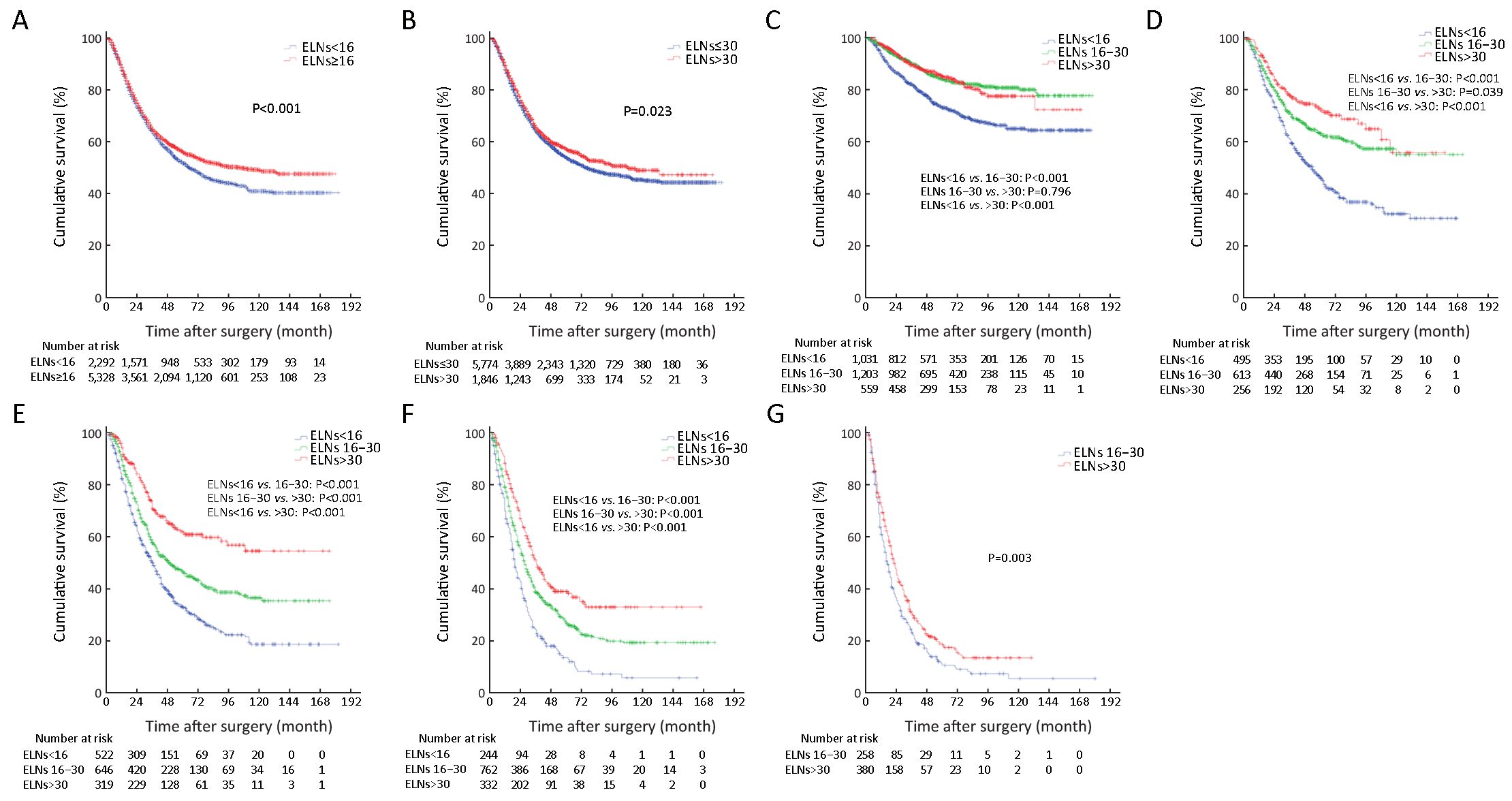
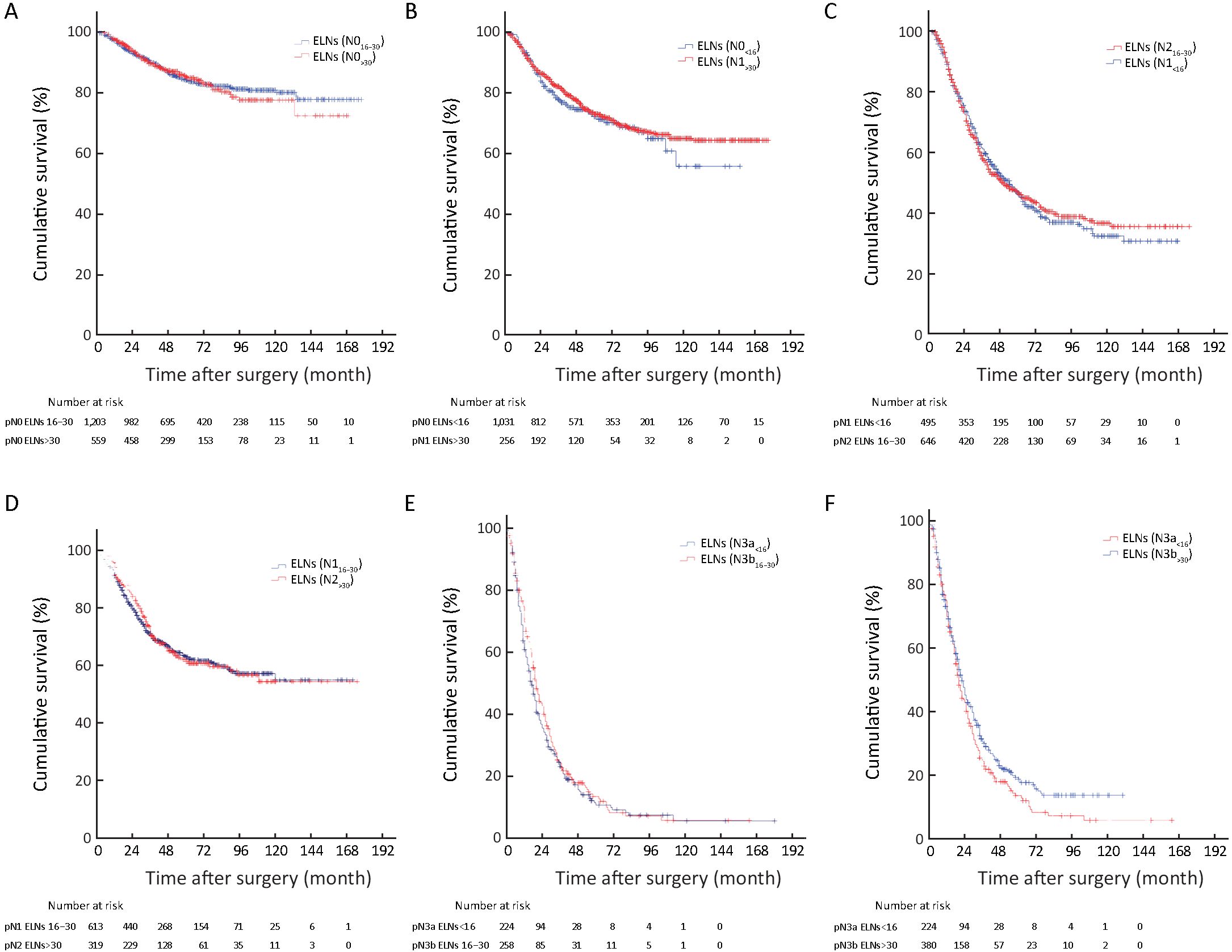
Objective To validate the necessity of increasing the examined lymph node (ELN) count for enhancing the accuracy of prognostic evaluation of gastric cancer (GC) patients after curative gastrectomy in multiple medical centers of China. Methods The clinicopathological data of 7,620 patients who underwent the curative resection for GC between 2001 and 2011 were included to demonstrate whether the ELN count is indispensable for enhancing the accuracy of prognostic evaluation of GC patients after surgery. After a meticulous stratification by using the cut-point survival analysis, all included 7,620 patients were allocated into three groups as: less than 16 (<16), between 16 and 30 (16−30), and more than 30 (>30) ELNs. Survival differences among various subgroups of GC patients were analyzed to assess the impact of the ELN count on the stage migration in accordance with the overall survival (OS) of GC patients. Results Survival analyses revealed that the ELN count was positively correlated with the OS (P=0.001) and was an independent prognostic predictor (P<0.01) of 7,620 GC patients. Stratum analysis showed that the accuracy of prognostic evaluation could be enhanced when the ELN count was no less than 16 (≥16) for node-negative patients and >30 for node-positive patients. Stage migrations were mainly detected in the various subgroups of patients with specific pN stages as follows: pN0 with 16−30 ELNs (pN016−30) and pN0 with >30 ELNs (pN0>30), pN0 with <16 ELNs (pN0<16) and pN1>30, pN1<16 and pN216−30, pN116−30 and pN2>30, pN3a<16 and pN3b16−30, and pN3a<16 and pN3b>30. These findings indicate that increasing the ELN count is a prerequisite to guarantee precisely prognostic evaluation of GC patients. Conclusions The ELN count should be proposed to be >30 for acquiring the accurate prognostic evaluation for GC patients, especially for node-positive patients.



2018, 30(5): 492-499.
doi: 10.21147/j.issn.1000-9604.2018.05.02
Abstract:
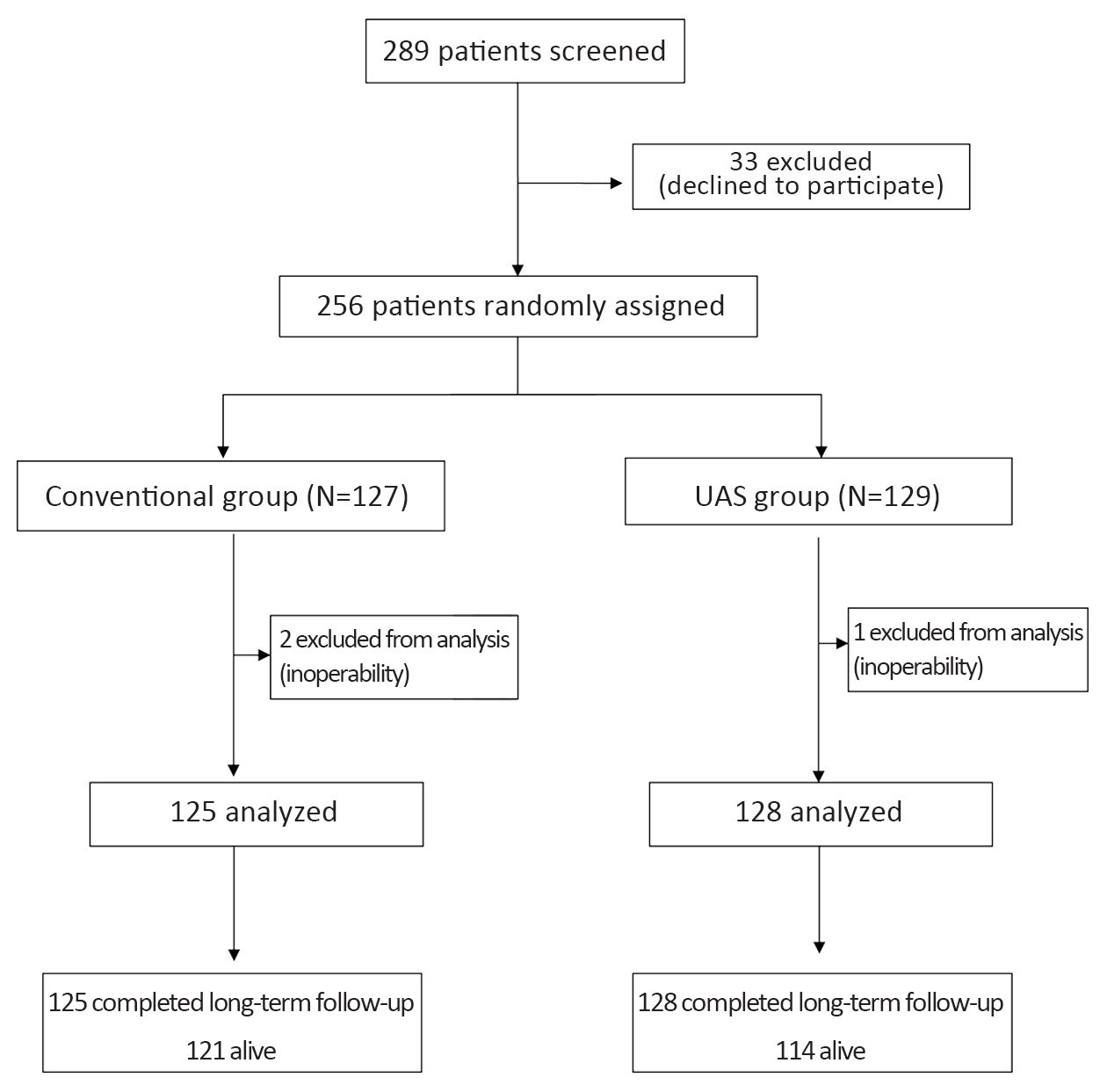
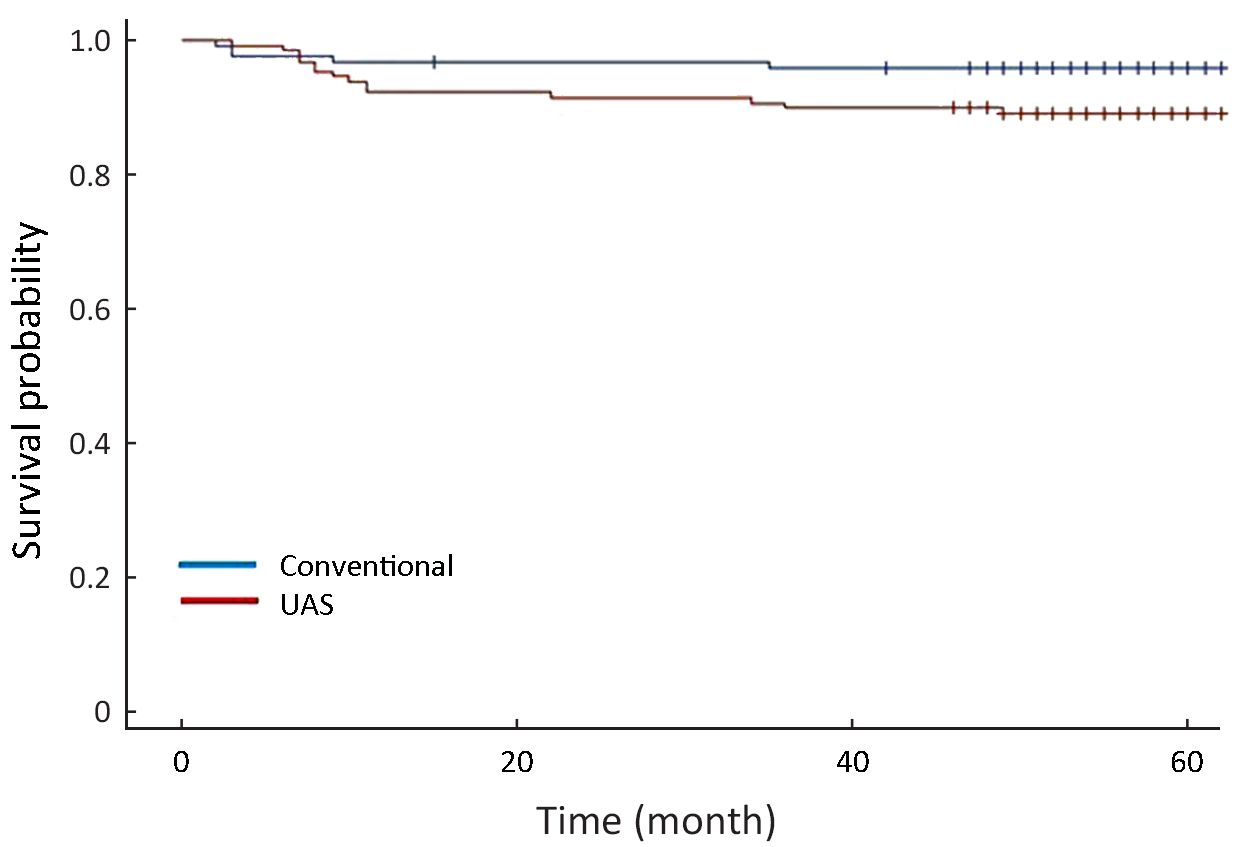
Objective Ultrasonically activated shears (UAS) have been applied in open gastric surgeries with no or little evidence. It was previously reported about the surgical outcome and effectiveness of UAS based on a randomized controlled trial of 256 patients with gastric cancer. We aimed to clarify the long-term oncological safety of the use of UAS in the aspect of overall survival and recurrence. Methods Gastric cancer patients who underwent gastrectomy with D2 lymph node dissection were enrolled and randomly assigned to either the conventional surgery group (n=125) or the UAS group (n=128). Survival, recurrence and long-term postoperative complications were compared between the two groups. The median follow-up period was 56 months. Results Gastric cancer-related death was higher in patients of the UAS group compared with the conventional group (P=0.019). Overall survival rates stratified by stage were not significantly different between the two groups (P=0.170). Disease-free survival rates stratified by stage and recurrence-free survival rates of gastric cancer were similar between the conventional group and the UAS group (P=0.313 and 0.199, respectively). The postoperative complication rate was not significantly different between the groups (P=1.000). Conclusions It is suggested that the use of UAS in gastrectomy for gastric cancer showed oncologically acceptable safety compared with conventional electric instruments even in long-term period.

2018, 30(5): 500-507.
doi: 10.21147/j.issn.1000-9604.2018.05.03
Abstract:
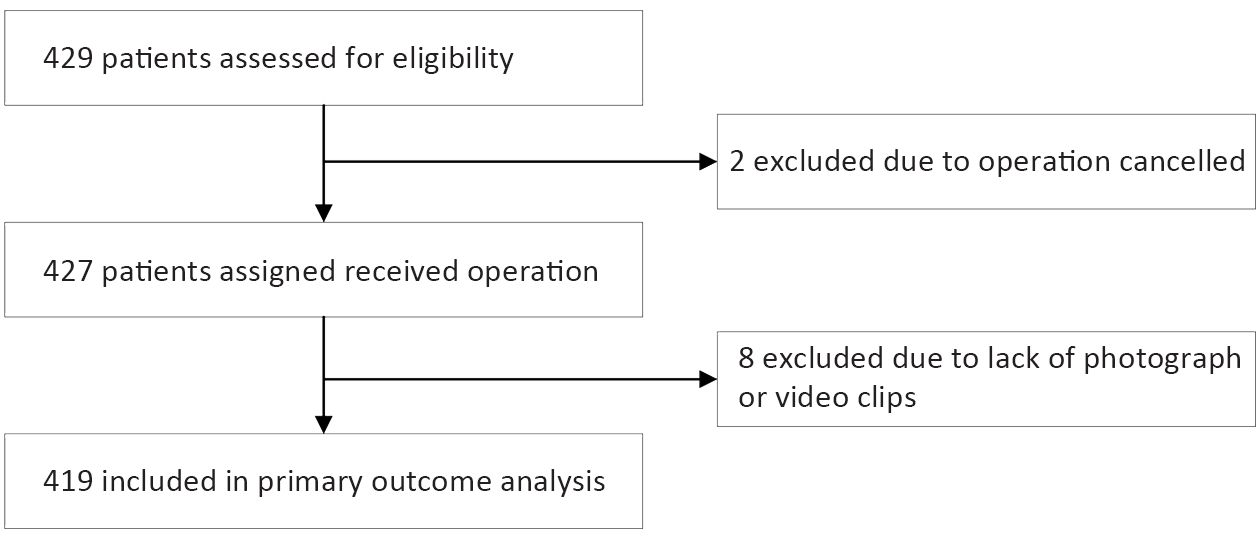
ObjectiveInfra-pyloric artery (IPA) is an important anatomical landmark in treatment of gastric cancer and is the key vessel for pylorus-preserving gastrectomy and subgroup of infra-pyloric lymph nodes. However, its anatomical variation is not thoroughly understood. Our study aimed to clarify the origination of the IPA. MethodsWe did this prospective, multicenter, open-label, observational study at gastric surgery departments of 34 hospitals in China. Gastric cancer patients aged 18 years or older and scheduled to undergo elective total or distal gastrectomy were assigned. During the surgery, IPA dissecting and exposing the origination point with photographs or video clips were required. The primary outcome was the origination of the IPA. Analysis of variance, χ2 tests and Fisher’s tests were used to analyze the differences between groups. The study is registered at Clinicaltrials.gov (No. NCT03071237). ResultsBetween May 8 and July 31, 2017, 429 patients were assigned for the study, and 419 (97.7%) patients had the IPA dissected and recorded through photograph or video and were included in the primary outcome analysis. The median age was 62 years old, and 73.7% were male. Among the patients, 78.5% received laparoscopic surgery. Single IPA origination was identified in 398 (95.0%) patients, including gastroduodenal artery (GDA) in 154 (36.8%) patients, anterior superior pancreaticoduodenal artery (ASPDA) in 130 (31.0%) patients, and right gastroepiploic artery (RGEA) in 114 (27.2%) patients. Fifteen (3.6%) patients were identified with multiple IPA and 6 (1.4%) patients were identified as IPA absence. The differences in the distribution of surgical approach (P=0.003) and geographic area (P=0.030) were statistically significant. No difference was shown in sex, age, gastrectomy type, tumor location, and clinical T, N and M stage. ConclusionsOur study found that the IPA originates from GDA, ASPDA and RGEA in similar proportions. Laparoscopic surgery may be more helpful in dissection of the IPA than open surgery.
2018, 30(5): 508-515.
doi: 10.21147/j.issn.1000-9604.2018.05.04
Abstract:
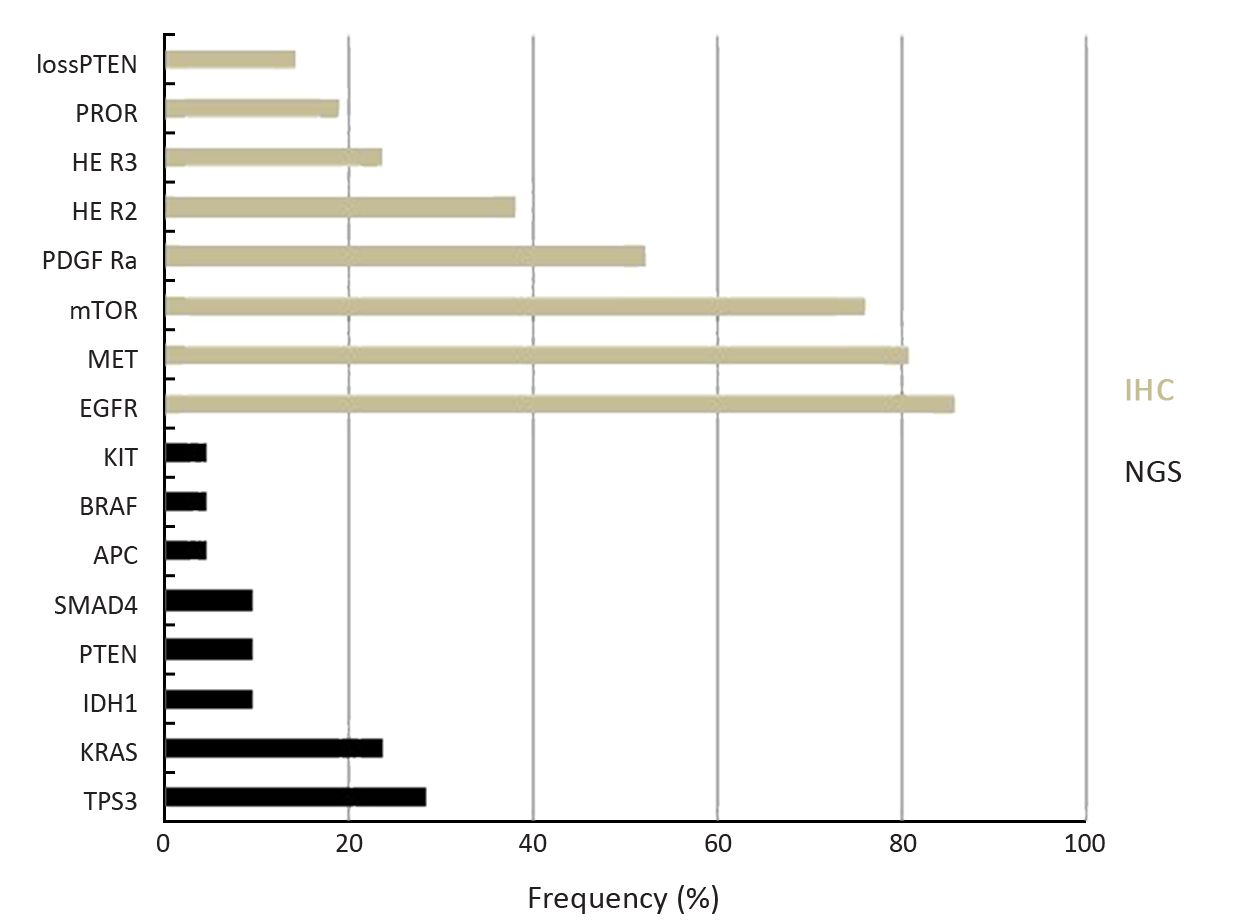
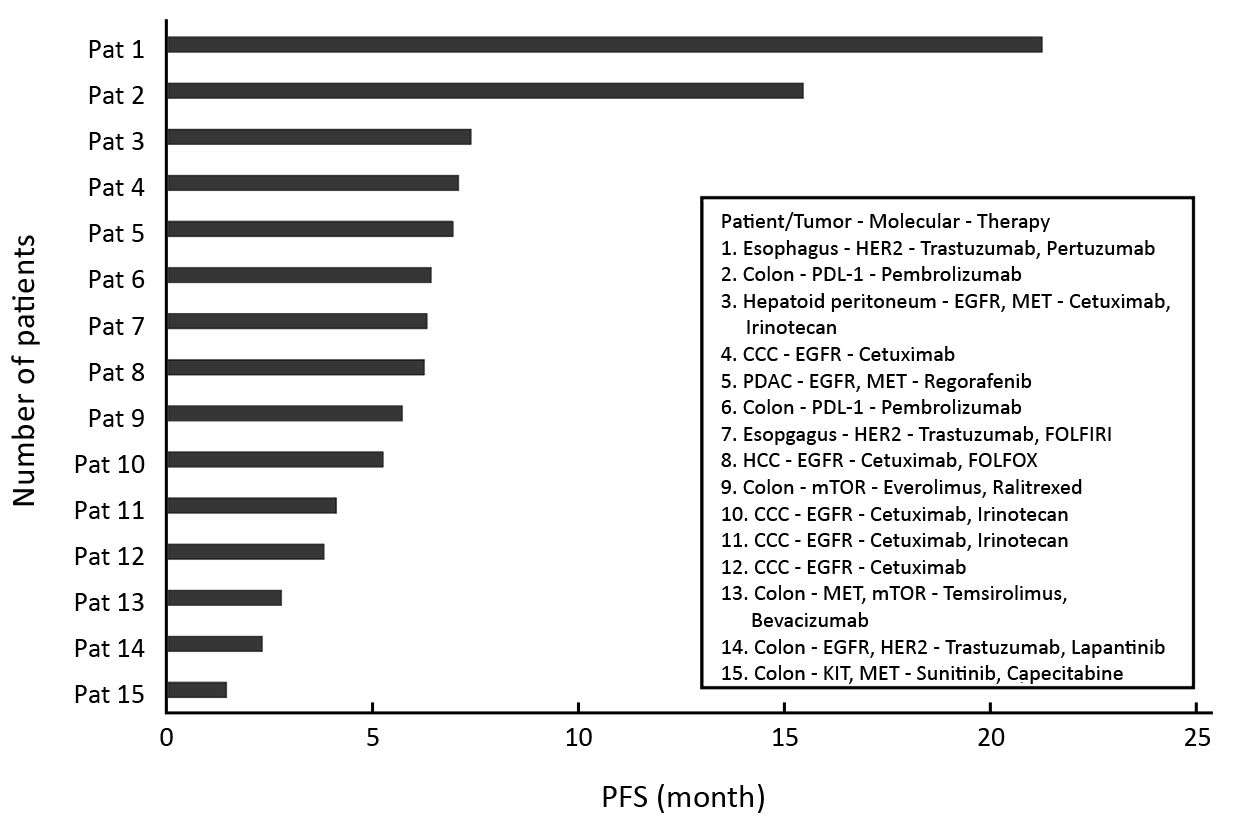
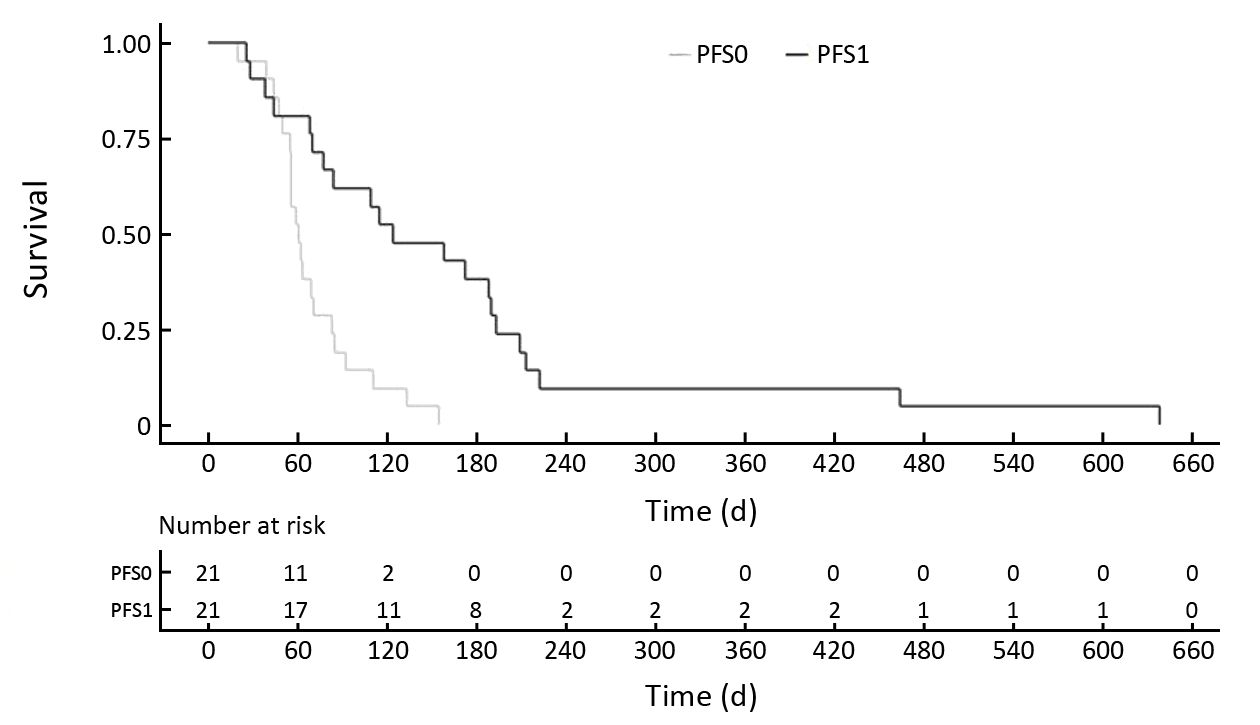
Objective Advances in high-throughput genomic profiling and the development of new targeted therapies improve patient’s survival. In gastrointestinal (GI) malignancies, the concept of personalized medicine (PM) was not investigated so far. The aim of this prospective study was to evaluate the efficacy of a personalized treatment in GI patients who failed standard treatment. Methods Out of the original prospective clinical phase II EXACT trial, 21 (38%) GI cancer patients who had no further treatment options were identified. A molecular profile (MP) via a 50 gene next generation sequencing (NGS) panel in combination with immunohistochemistry (IHC) was conducted using real-time biopsy tumor material. Results were discussed by a multidisciplinary team (MDT) to translate the individual MP in an experimental treatment. Results Of the 55 patients originally included in the EXACT trial, 21 (38%) suffered from GI malignancies. The final analysis showed that 15 (71%) patients had experienced a longer progression-free survival (PFS) upon experimental targeted treatment (124 d, quartiles 70/193 d), when compared with the PFS achieved by the previous conventional therapy (62 d, quartiles 55/83 d) (P=0.014). Thirteen (62%) patients receiving targeted treatment experienced a disease control according to Response Evaluation Criteria in Solid Tumors (RECIST). Median overall survival (OS) from the start of experimental therapy to time of censoring or death was 193 d (quartiles 115/374 d). Conclusions PM was not investigated in GI malignancies so far in a prospective trial. This study shows that treatment based on real-time molecular tumor profiling led to a superior clinical benefit, and survival as well as response was significantly improved when compared with previous standard medications.
2018, 30(5): 516-525.
doi: 10.21147/j.issn.1000-9604.2018.05.05
Abstract:
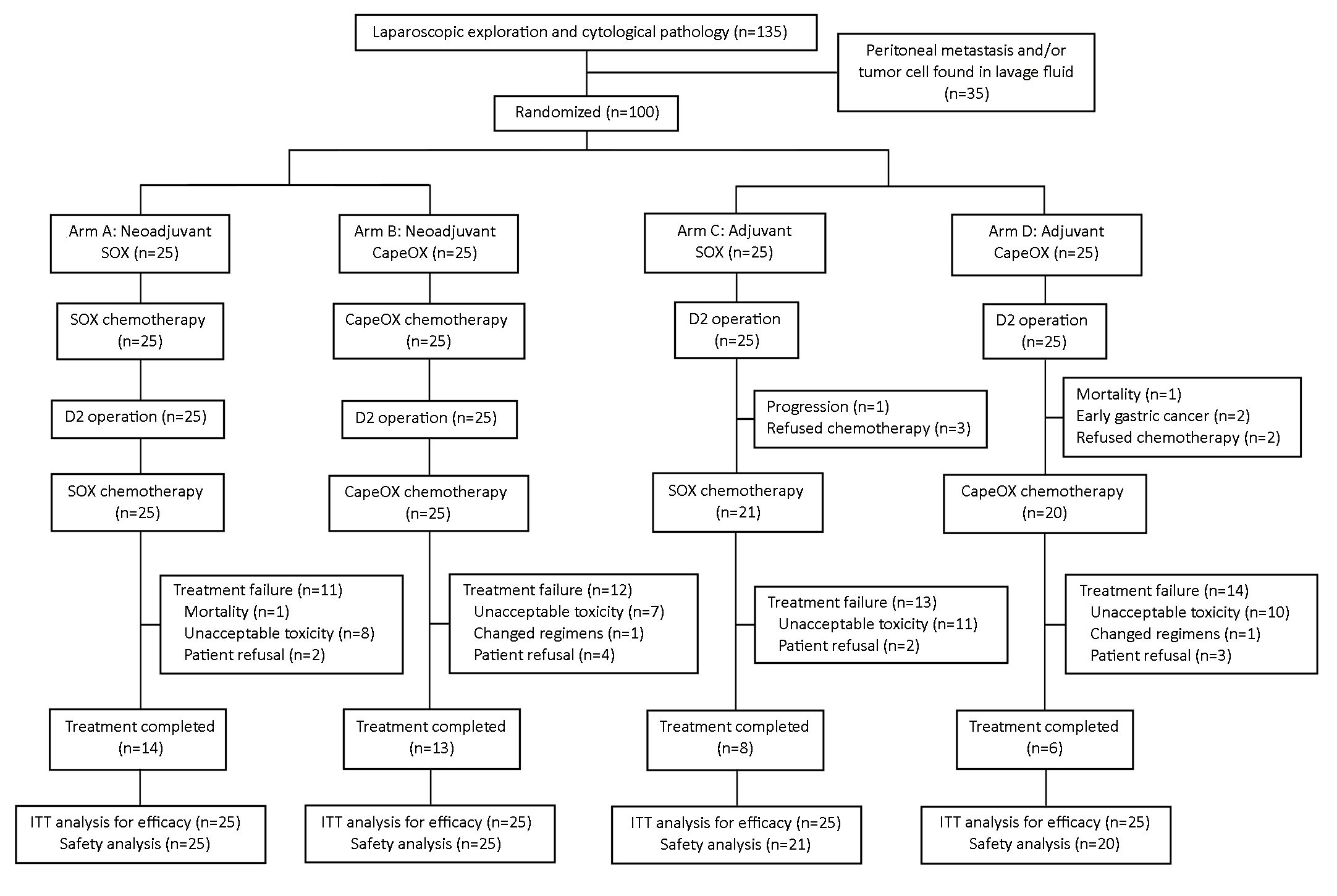
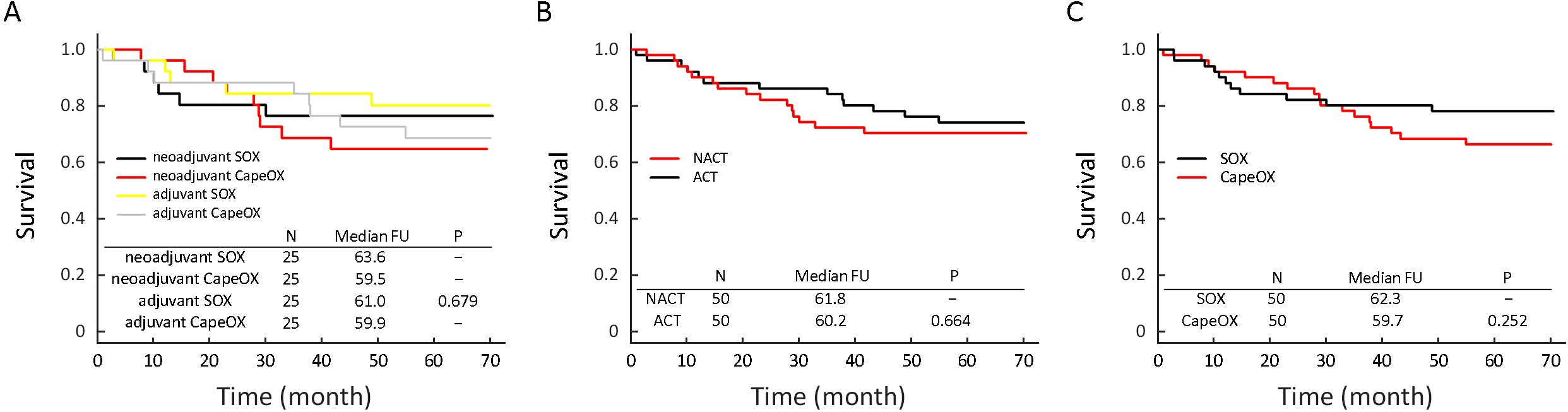
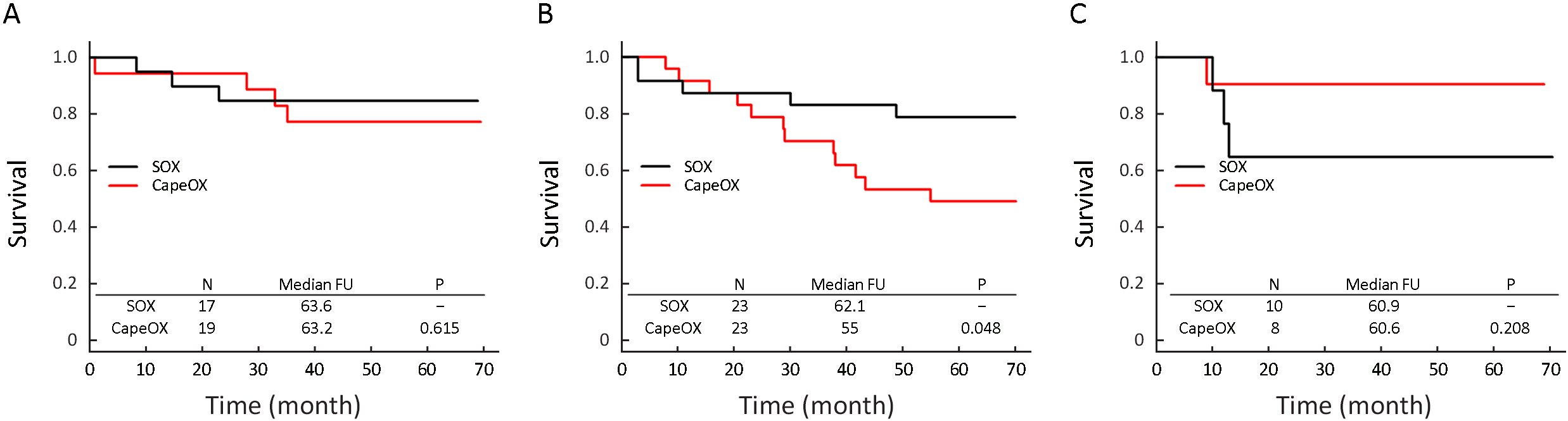
Objective To compare the effect of neoadjuvant chemotherapy (NACT) with adjuvant chemotherapy (ACT) using oxaliplatin plus S-1 (SOX) or capecitabine (CapeOX) on gastric cancer patients with D2 lymphadenectomy. Methods This was a two-by-two factorial randomized phase II−III trial, and registered on ISRCTN registry (No. ISRCTN12206108). Locally advanced gastric cancer patients were randomized to neoadjuvant SOX, neoadjuvant CapeOX, adjuvant SOX, or adjuvant CapeOX arms. Primary analysis was performed on an intention-to-treat (ITT) basis using overall survival (OS) as primary endpoint. Results This trial started in September 2011 and closed in December 2012 with 100 patients enrolled. Treatment completion rate was 56%, 52%, 38% and 30% in the four arms, respectively. NACT group had fewer dropouts due to unacceptable toxicity (P=0.042). Surgical complication rate did not differ by the four groups (P=0.986). No survival significant difference was found comparing NACT with ACT (P=0.664; 5-year-OS: 70% vs. 74% respectively), nor between the SOX and CapeOX groups (P=0.252; 5-year-OS: 78% vs. 66% respectively). Subgroup analysis showed SOX significantly improved survival in patients with diffuse type (P=0.048). Conclusions No significant survival difference was found between NACT and ACT. SOX and CapeOX had good safety and efficacy as neoadjuvant regimens. Diffuse type patients may survive longer due to SOX.
2018, 30(5): 526-536.
doi: 10.21147/j.issn.1000-9604.2018.05.06
Abstract:
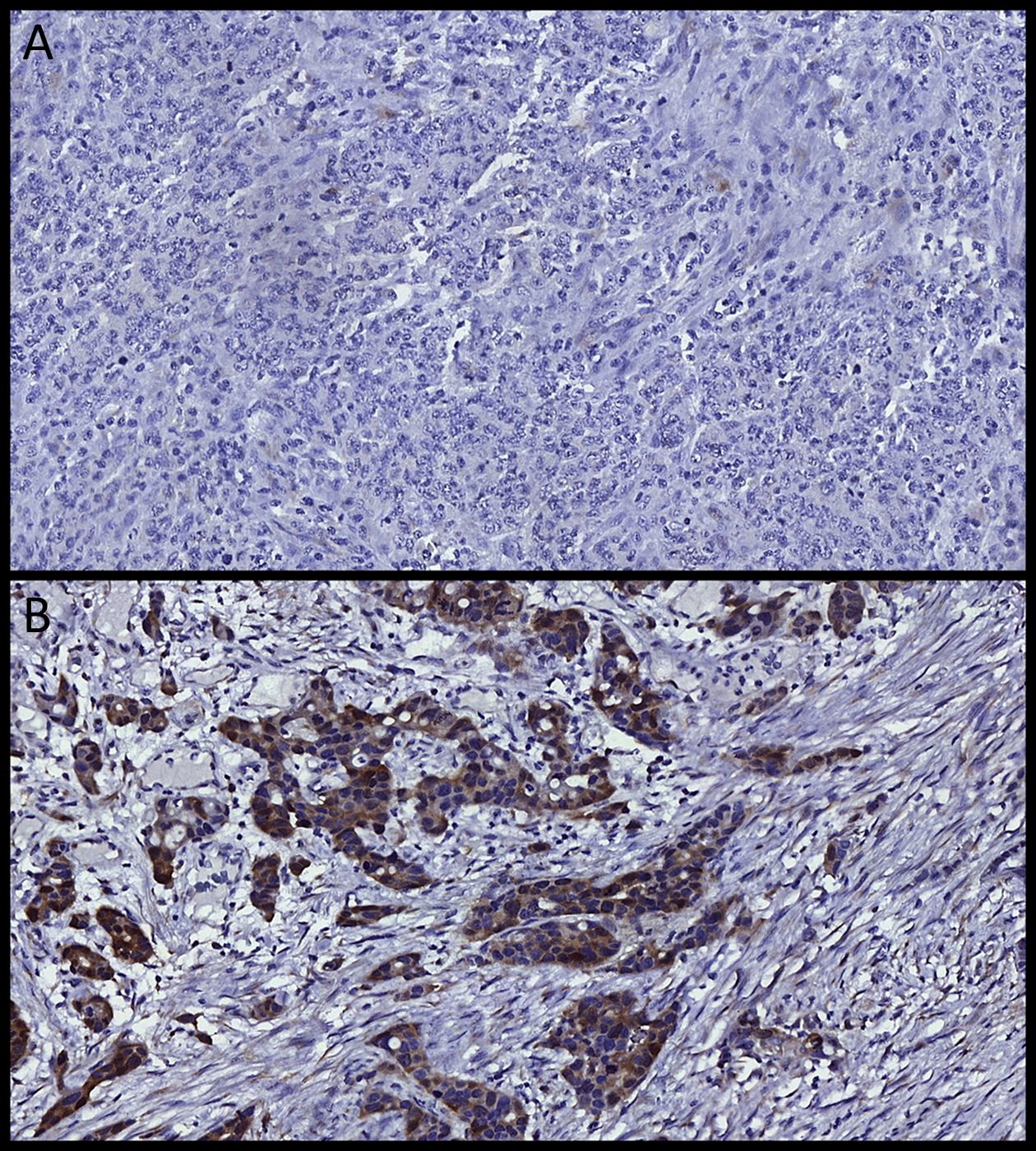
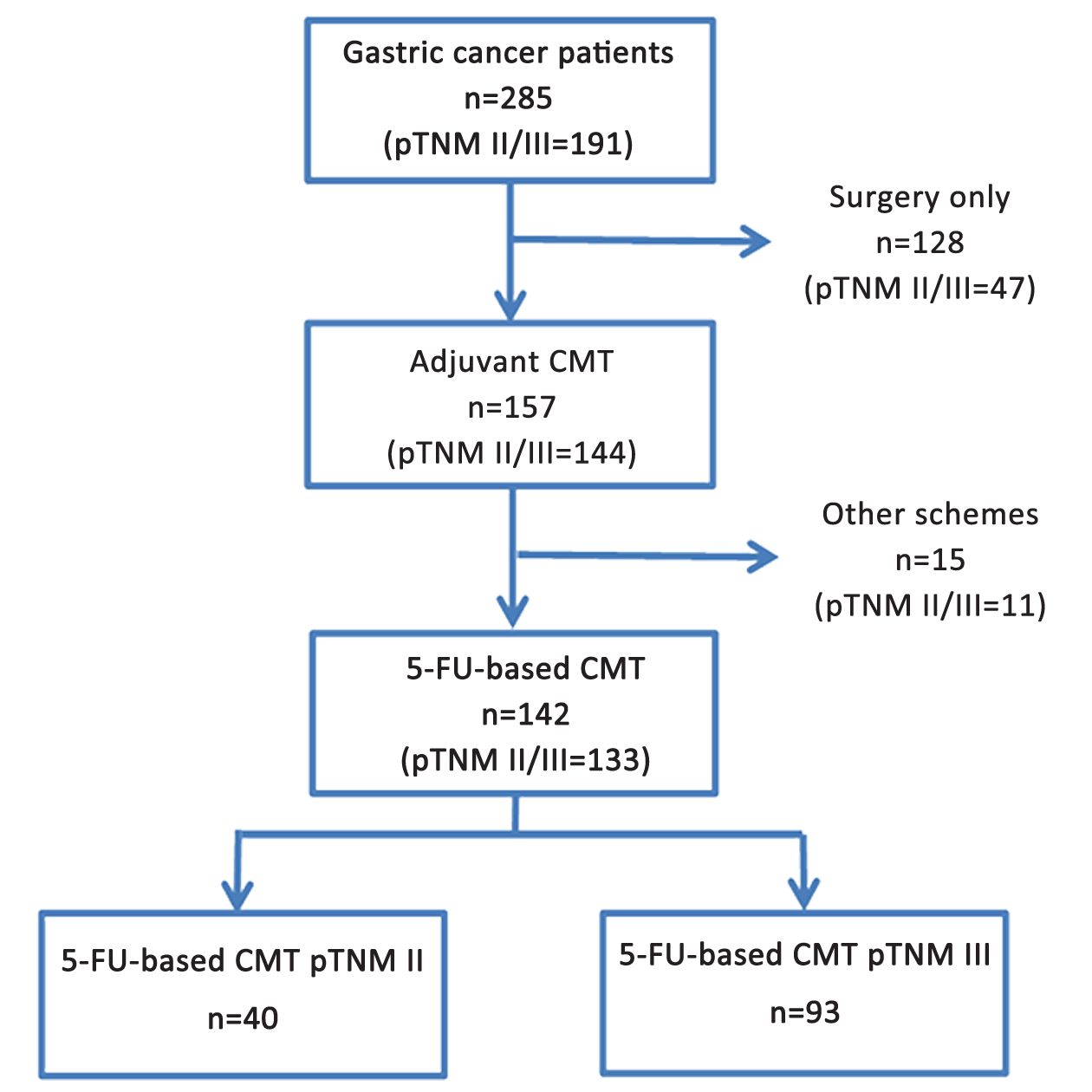
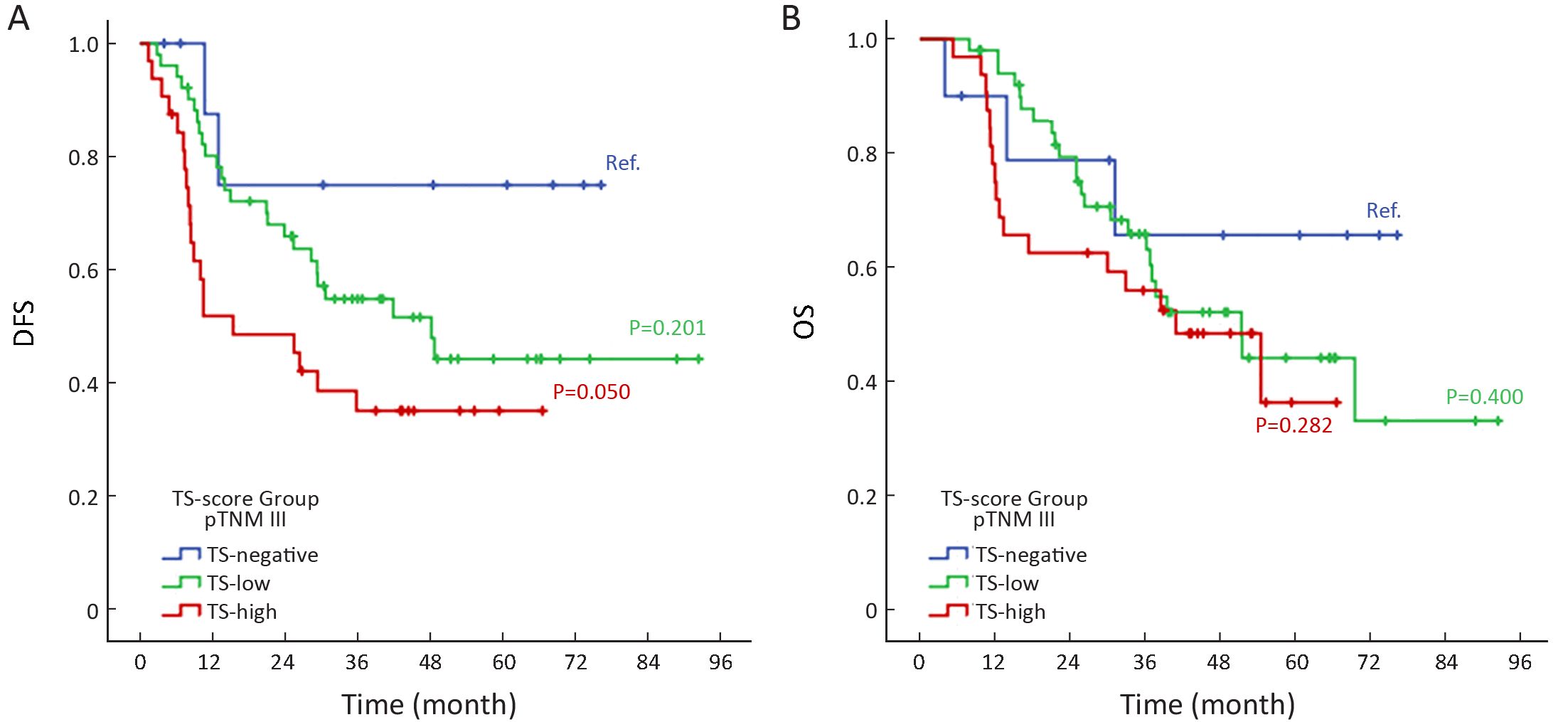
ObjectiveAdjuvant chemotherapy with 5-fluorouracil (5-FU) has been widely used in gastric cancer (GC) patients to prevent relapse after curative resection. 5-FU acts by inhibiting thymidylate synthase (TS), and high levels of TS correlate with resistance to treatment with fluoropyrimidines. The aim of this study was to evaluate the expression of TS in GC patients, and its relation with clinicopathological characteristics and prognosis in adjuvant chemotherapy with 5-FU. MethodsWe retrospectively evaluated 285 patients who underwent D2-gastrectomy with curative intent. TS expression was determined by immunohistochemistry (IHC) in tumor cells by tissue microarray (TMA). TS level was evaluated according to the intensity and percentage of cells marked by a score system. Patients were divided in three groups according to their TS-score: negative, low and high. ResultsTS expression was positive in 92.3% of GC. TS-high, TS-low and TS-negative were observed in 46.3%, 46.0% and 7.7% of patients, respectively. High-TS GC were associated with older age (P=0.007), high neutrophil/lymphocyte ratio (P=0.048), well/moderately differentiated histology (P=0.001), intestinal Lauren type (P<0.001) and absence of perineural invasion (P=0.003). Among 285 patients, 133 stage II/III patients (46.7%) received chemotherapy with 5-FU. In survival analysis, TS-high was associated with worse disease-free survival (DFS) in stage III GC patients who received 5-FU-based chemotherapy (P=0.007). Multivariate analysis revealed that total gastrectomy, poorly differentiated tumors and high TS-score were associated with worse DFS in stage III GC patients. ConclusionsHigh TS-score in stage III GC was associated with poor DFS in patients treated with fluoropyrimidine-based chemotherapy.
2018, 30(5): 537-545.
doi: 10.21147/j.issn.1000-9604.2018.05.07
Abstract:
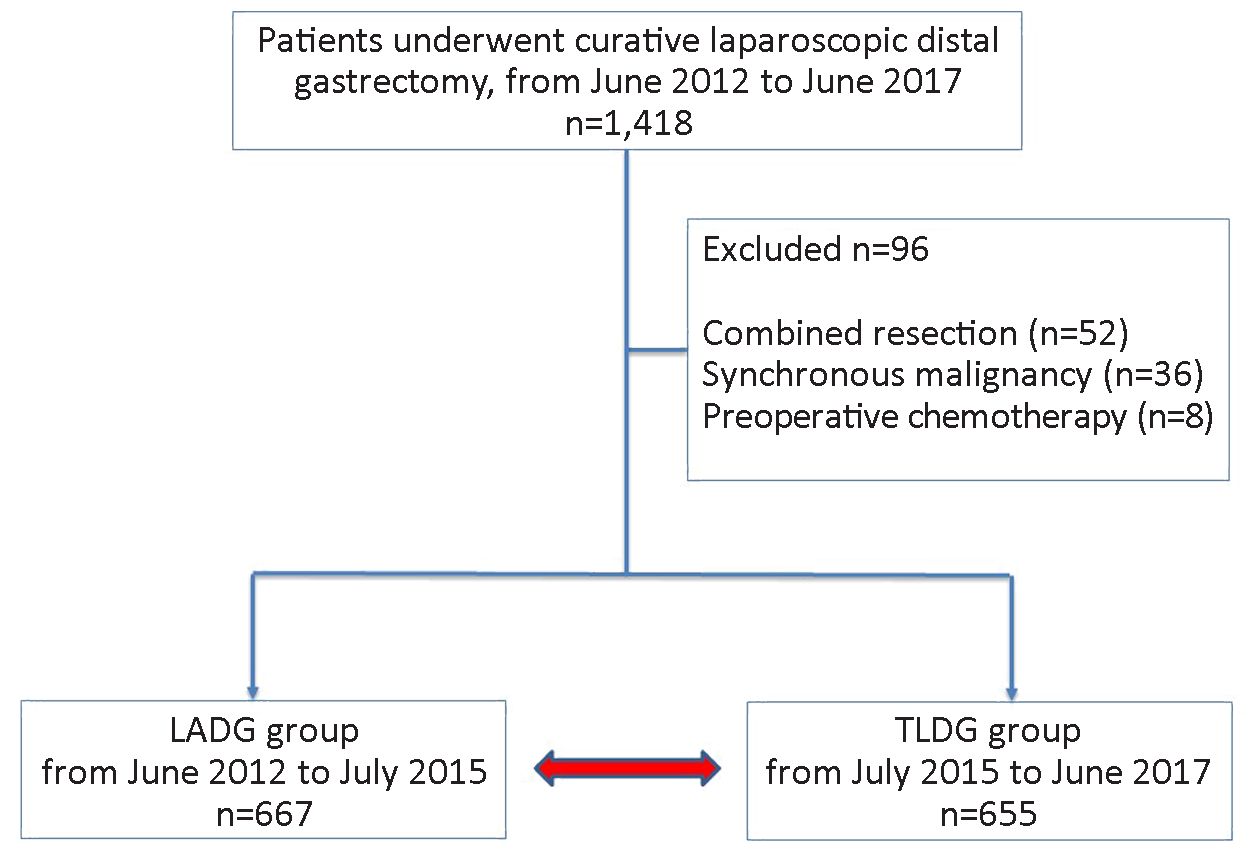
Objective Laparoscopic gastrectomy has been established as a standard treatment for early gastric cancer, and its use is increasing recently. Compared with the conventional laparoscopy-assisted distal gastrectomy (LADG), totally laparoscopic distal gastrectomy (TLDG) involves intracorporeal reconstruction, which can avoid the additional incision, resulting in pain reduction and early recovery. This study aimed to compare the short-term postoperative outcomes of TLDG vs. LADG in gastric cancer in a high-volume center. Methods A retrospective cohort study was conducted on 1,322 patients who underwent laparoscopic distal gastrectomy from June 2012 to June 2017 at the National Cancer Center, Korea. LADG was performed in the early period before July 2015, and TLDG was applied in the later period. Postoperative short-term outcomes were compared in terms of complication and clinical course between the two groups. Pain score was measured by rating the pain intensity from 0 to 10 points on postoperative day (POD) 1 and 3. Results A total of 667 patients underwent LADG and 655 patients underwent TLDG. Clinicopathologic characteristics were not different in both groups. Intraoperative estimated blood loss (EBL) was significantly lower in the TLDG group (P<0.001). Postoperative pain scores were significantly lower in the TLDG group than in the LADG group on POD 1 (5.1±1.5 vs. 4.8±1.4, P=0.015). First flatus passage after operation was significantly earlier in the TLDG group (3.4±0.8 d vs. 3.2±0.6 d, P<0.001). There were no differences in postoperative complications and hospital stay between the two groups. Conclusions Based on the reported short-term postoperative outcomes, TLDG is safe and feasible as well as LADG. Moreover, compared with LADG, TLDG can reduce intraoperative EBL and postoperative pain and enhance the bowel motility in gastric cancer surgery.
2018, 30(5): 546-552.
doi: 10.21147/j.issn.1000-9604.2018.05.08
Abstract:
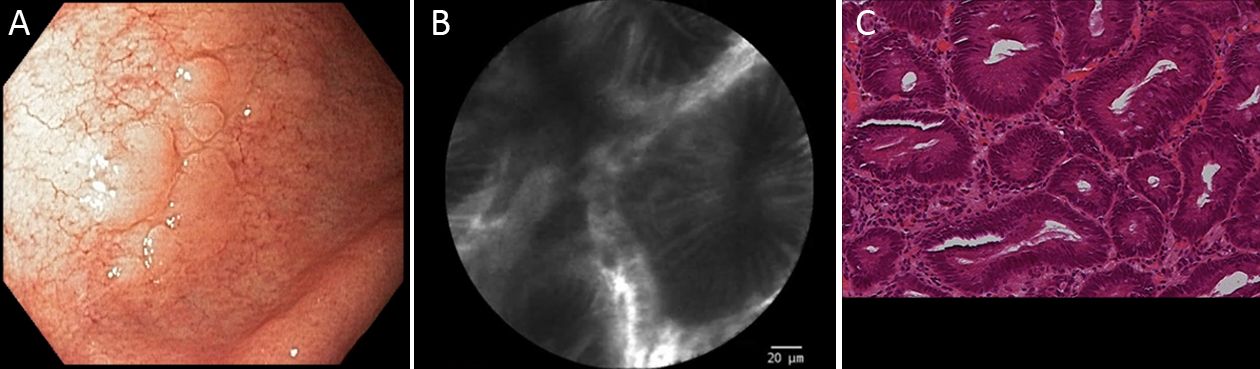
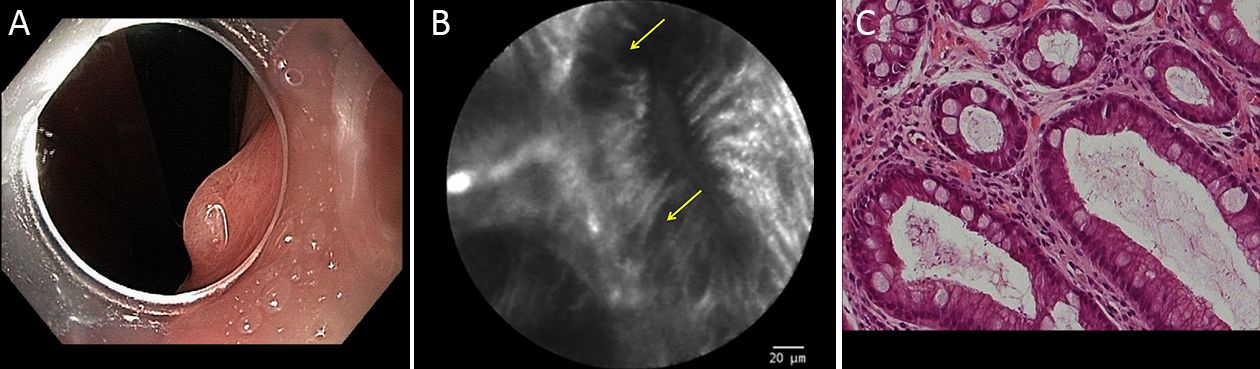
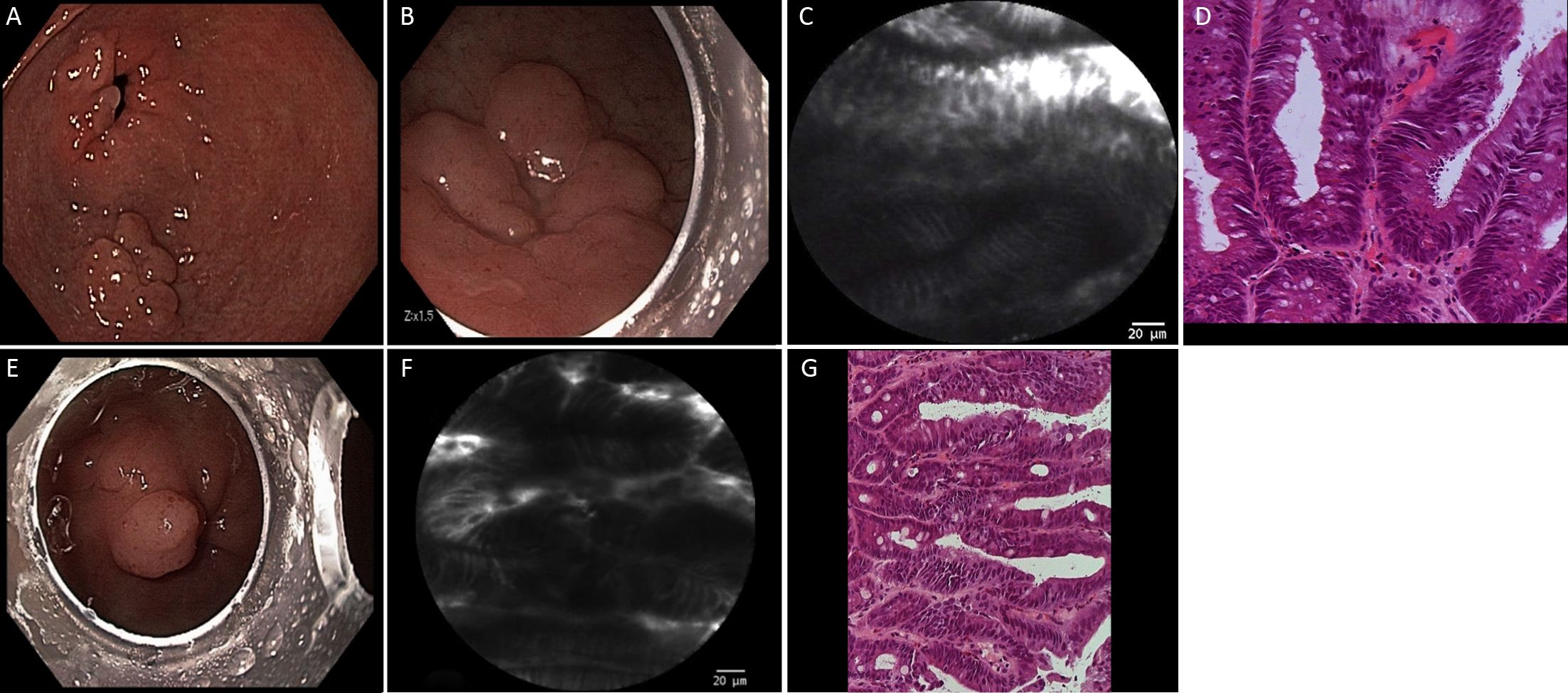
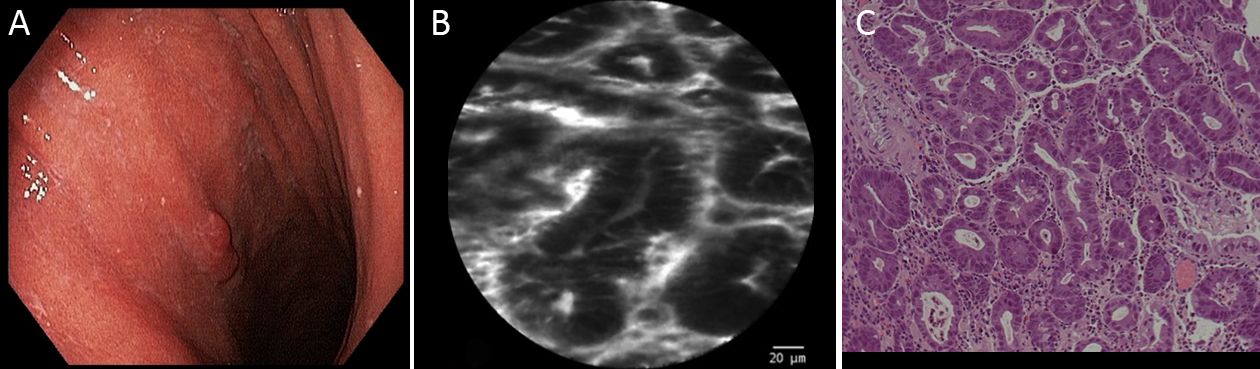
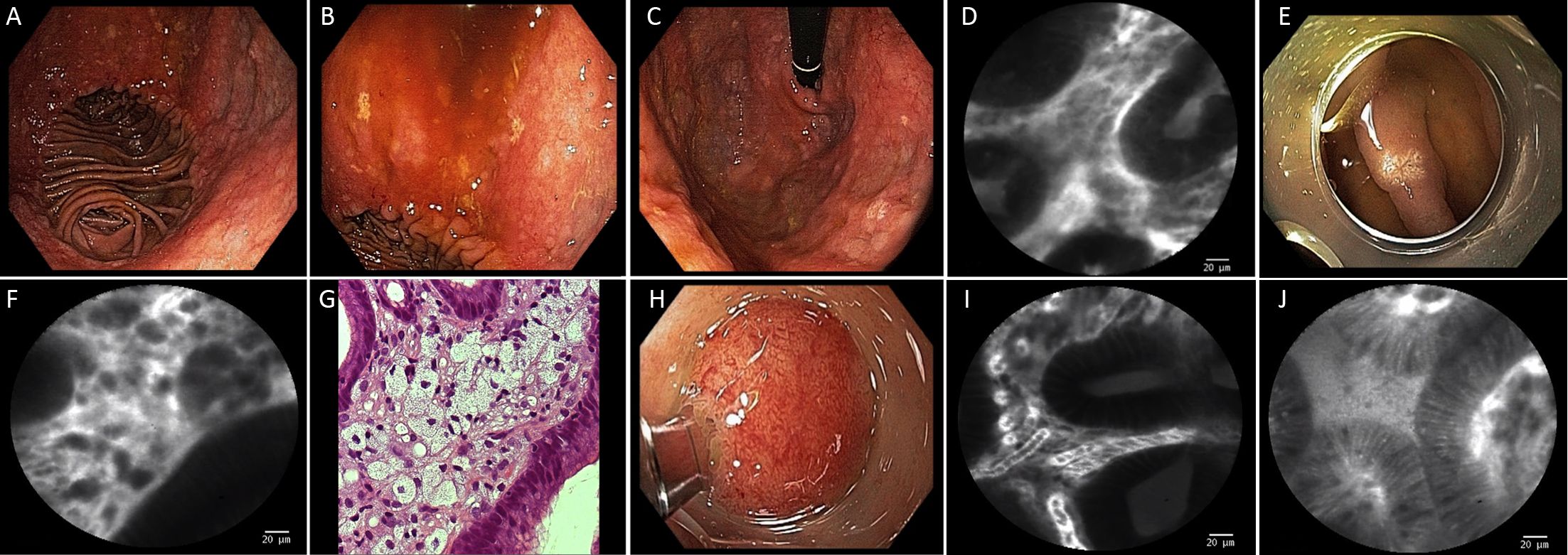
Objective Probe-based confocal laser endomicroscopy (pCLE) technique may improve the diagnosis of gastric mucosal lesions allowing acquisition of high-resolution in vivo images at the cellular and microvascular levels. This study aims to evaluate the accuracy of pCLE for the differential diagnosis of non-neoplastic and neoplastic gastric lesions. Methods Twenty gastric mucosal lesions from 10 patients were evaluated during endoscopic procedure and were examined by pCLE. Diagnostic pCLE was followed by biopsies or endoscopic resection of suspected lesions. A senior pathologist evaluated the specimens and was blinded to the pCLE results. Results Patients’ mean age was 68.3 (range, 42−83) years and six were men. Thirteen suspicious flat or elevated lesions (classified as 0−Is, 0−IIa or 0−IIa + IIc) and seven pre-malignant lesions (atrophy and intestinal metaplasia) were evaluated. One patient was studied during his long-term follow-up after partial gastrectomy and presented severe atrophy, intestinal metaplasia, and xanthomas at the stump mucosa. The location of gastric lesions was in the body (n=10 lesions), the antrum (n=9) and the incisura angularis (n=1). All neoplastic lesions and all but one benign lesion were properly diagnosed by pCLE. pCLE incorrectly diagnosed one small antrum lesion as adenoma, however the final diagnosis was intestinal metaplasia. The final histological diagnosis was neoplastic in 9 and benign lesions in 11. In this small case series, pCLE accuracy was 95% (19/20 lesions). Conclusions pCLE is accurate for real time histology of gastric lesions. pCLE may change the management of patients with gastric mucosal lesions, guiding biopsies and endoscopic resection, and avoiding further diagnostic workup or unnecessary therapy.

2018, 30(5): 553-563.
doi: 10.21147/j.issn.1000-9604.2018.05.09
Abstract:
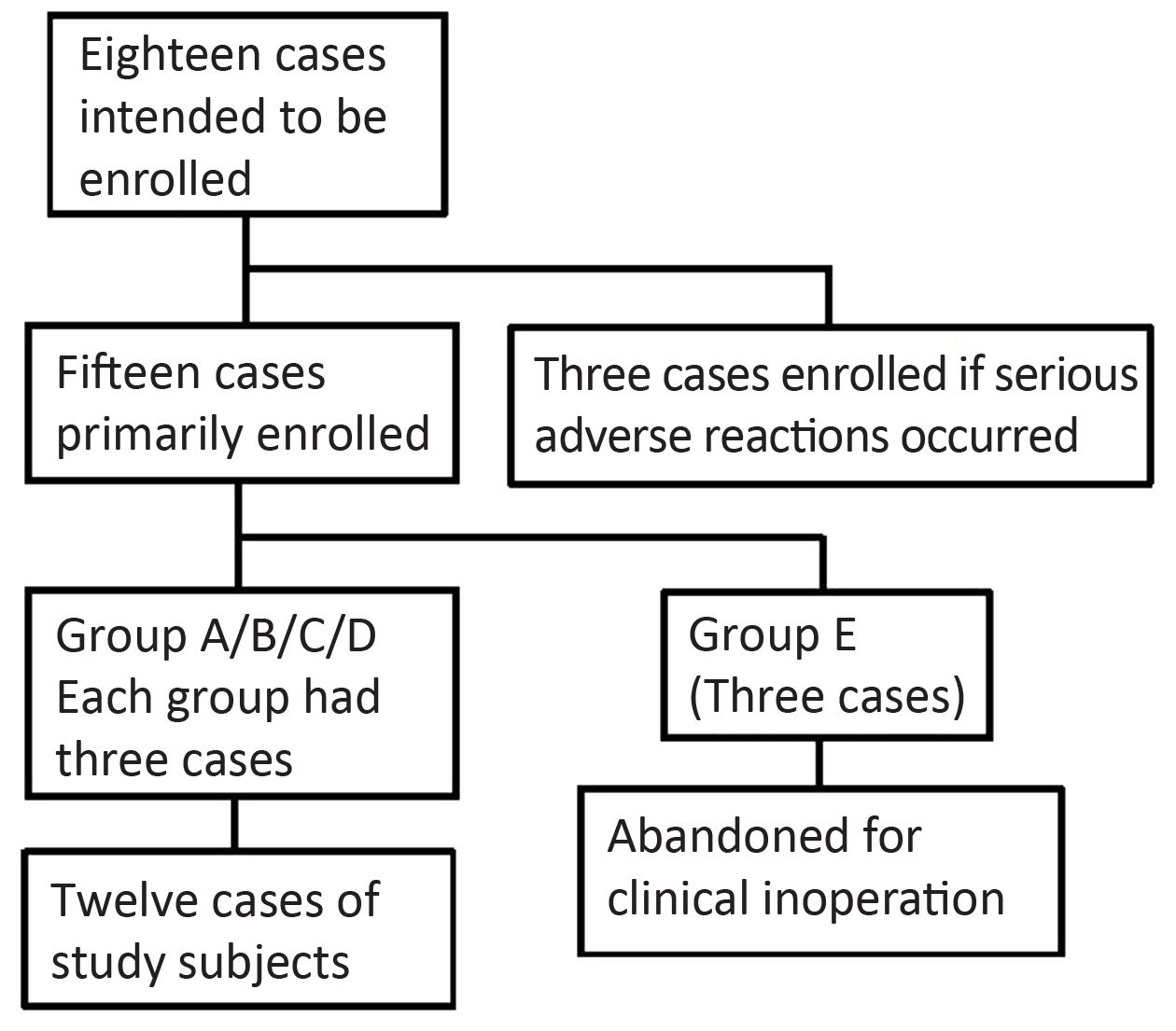
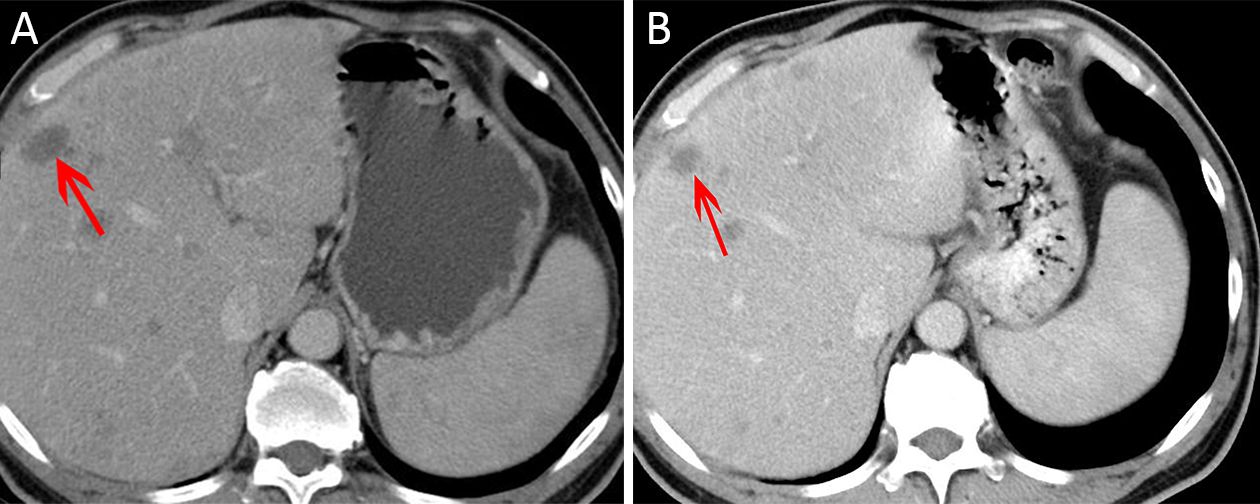
Objective To explore the safety of ultrasound and microbubbles for enhancing the chemotherapeutic sensitivity of malignant tumors in the digestive system in a clinical trial, as well as its efficacy. Methods From October 2014 to June 2016, twelve patients volunteered to participate in this study. Eleven patients had hepatic metastases from tumors of the digestive system, and one patient had pancreatic carcinoma. According to the mechanical index (MI) in the ultrasound field, patients were classified into four groups with MIs of 0.4, 0.6, 0.8 and 1.0. Within half an hour after chemotherapy, patients underwent ultrasound scanning with ultrasound microbubbles (SonoVue) to enhance the efficacy of chemotherapy. All adverse reactions were recorded and were classified in 4 grades according to the Common Terminology Criteria for Adverse Events version 4.03 (CTCAE V4.03). Tumor responses were evaluated by the Response Evaluation Criteria in Solid Tumors version 1.1 criteria. All the patients were followed up until progression. Results All the adverse reactions recorded were level 1 or level 2. No local pain occurred in any of the patients. Among all the adverse reactions, fever might be related to the treatment with ultrasound combined with microbubbles. Six patients had stable disease (SD), and one patient had a partial response (PR) after the first cycle of treatment. At the end of follow-up, tumor progression was restricted to the original sites, and no new lesions had appeared. Conclusions Our preliminary data showed the potential role of a combined treatment with ultrasound and microbubbles in enhancing the chemotherapeutic sensitivity of malignant tumors of the digestive system. This technique is safe when the MI is no greater than 1.0.
2018, 30(5): 564-567.
doi: 10.21147/j.issn.1000-9604.2018.05.10
Abstract:
The search for cancer biomarkers is frequently based on comparisons between tumors and adjacent-to-tumor samples. However, even after histological confirmation of been free of cancer cells, these adjacent-to-tumor samples might harbor molecular alterations which are not sufficient to cause them to look like cancer, but can differentiate these cells from normal cells. When comparing them, potential biomarkers are missed, and mainly the opportunity of finding initial aberrations presents in both tumors and adjacent samples, but not in true normal samples from non-cancer patients, resulting in misinterpretations about the carcinogenic process. Nevertheless, collecting adjacent-to-tumor samples brings trumps to be explored. The addition of samples from non-cancer patients opens an opportunity to increase the finds of the molecular cascade of events in the carcinogenic process. Differences between normal samples and adjacent samples might represent the first steps of the carcinogenic process. Adding samples of non-cancer patients to the analysis of molecular alterations relevant to the carcinogenic process opens a new window of opportunities to the discovery of cancer biomarkers and molecular targets.
The search for cancer biomarkers is frequently based on comparisons between tumors and adjacent-to-tumor samples. However, even after histological confirmation of been free of cancer cells, these adjacent-to-tumor samples might harbor molecular alterations which are not sufficient to cause them to look like cancer, but can differentiate these cells from normal cells. When comparing them, potential biomarkers are missed, and mainly the opportunity of finding initial aberrations presents in both tumors and adjacent samples, but not in true normal samples from non-cancer patients, resulting in misinterpretations about the carcinogenic process. Nevertheless, collecting adjacent-to-tumor samples brings trumps to be explored. The addition of samples from non-cancer patients opens an opportunity to increase the finds of the molecular cascade of events in the carcinogenic process. Differences between normal samples and adjacent samples might represent the first steps of the carcinogenic process. Adding samples of non-cancer patients to the analysis of molecular alterations relevant to the carcinogenic process opens a new window of opportunities to the discovery of cancer biomarkers and molecular targets.
2018, 30(5): 568-570.
doi: 10.21147/j.issn.1000-9604.2018.05.11
Abstract:
In recent years, some researchers have tried to find a way to improve the surgical identification of the lymphatic drainage routes and lymph node stations during radical gastrectomy, thus starting a new research frontier in this field called " navigation surgery”. Among the different reported solutions, the introduction of the indocyanine green (ICG) has drawn attention for its characteristics, a fluorescence dye that can be detected in the near infrared spectral band (NIR). A fluorescence imaging technology has been integrated in the latest version of the Da Vinci robotic system and surgeons have extensively reported their experiences in colorectal and hepato-biliary surgery for tumors, vascular and lymphatic structures visualization. However, up to date, the combined use of fluorescence imaging and robotic technology has not been adequately investigated during lymphadenectomy in gastric cancer.
In recent years, some researchers have tried to find a way to improve the surgical identification of the lymphatic drainage routes and lymph node stations during radical gastrectomy, thus starting a new research frontier in this field called " navigation surgery”. Among the different reported solutions, the introduction of the indocyanine green (ICG) has drawn attention for its characteristics, a fluorescence dye that can be detected in the near infrared spectral band (NIR). A fluorescence imaging technology has been integrated in the latest version of the Da Vinci robotic system and surgeons have extensively reported their experiences in colorectal and hepato-biliary surgery for tumors, vascular and lymphatic structures visualization. However, up to date, the combined use of fluorescence imaging and robotic technology has not been adequately investigated during lymphadenectomy in gastric cancer.


