
2019 Vol.31(5)
Display Mode: |
2019, 31(5): 707-737.
doi: 10.21147/j.issn.1000-9604.2019.05.01
 Abstract
Abstract FullText HTML
FullText HTML PDF 1139KB
PDF 1139KB
Abstract:

2019, 31(5): 738-739.
doi: 10.21147/j.issn.1000-9604.2019.05.02
Abstract:
2019, 31(5): 740-741.
doi: 10.21147/j.issn.1000-9604.2019.05.03
Abstract:
2019, 31(5): 742-748.
doi: 10.21147/j.issn.1000-9604.2019.05.04
Abstract:
ObjectiveFluid therapy is one of the key components of perioperative management. However, evidence of intraoperative fluid (IOF) administration affecting clinical outcomes following McKeown esophagogastrectomy remains limited. This study investigated the impact of IOF on clinical outcomes after McKeown esophagogastrectomy. MethodsPatients who underwent McKeown esophagogastrectomy between July 2013 and July 2016 were identified. Preoperative, intraoperative and postoperative variables for each eligible patient were retrospectively collected from our electronic medical records and anesthetic records. IOF rates were determined and their relationships to postoperative clinical outcomes were compared. ResultsA total of 546 patients were enrolled in the analysis. The median IOF rate was 8.87 mL/kg/h. We divided the patients into two groups: a low fluid volume group (LFVG <8.87 mL/kg/h, n=273) and a high fluid volume group (HFVG ≥8.87 mL/kg/h, n=273). No statistically significant differences in postoperative clinical outcomes were found between LFVG and HFVG either before or after propensity score matching. ConclusionsNo effect of IOF administration on clinical outcomes in patients undergoing McKeown esophagogastrectomy was identified. Further high-quality studies examining the influence of IOF administration on clinical outcomes following McKeown esophagogastrectomy are still needed.
2019, 31(5): 749-758.
doi: 10.21147/j.issn.1000-9604.2019.05.05
Abstract:
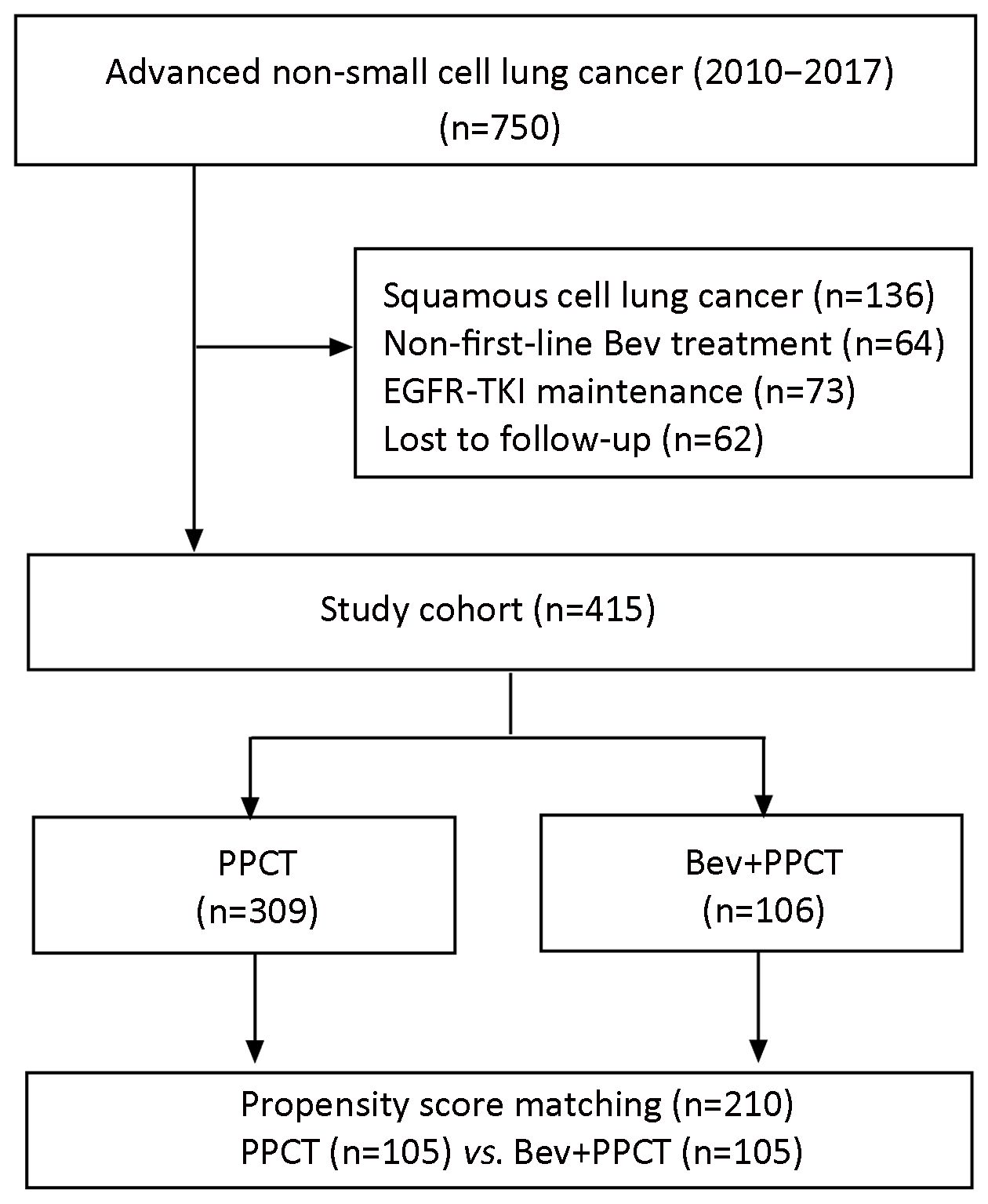
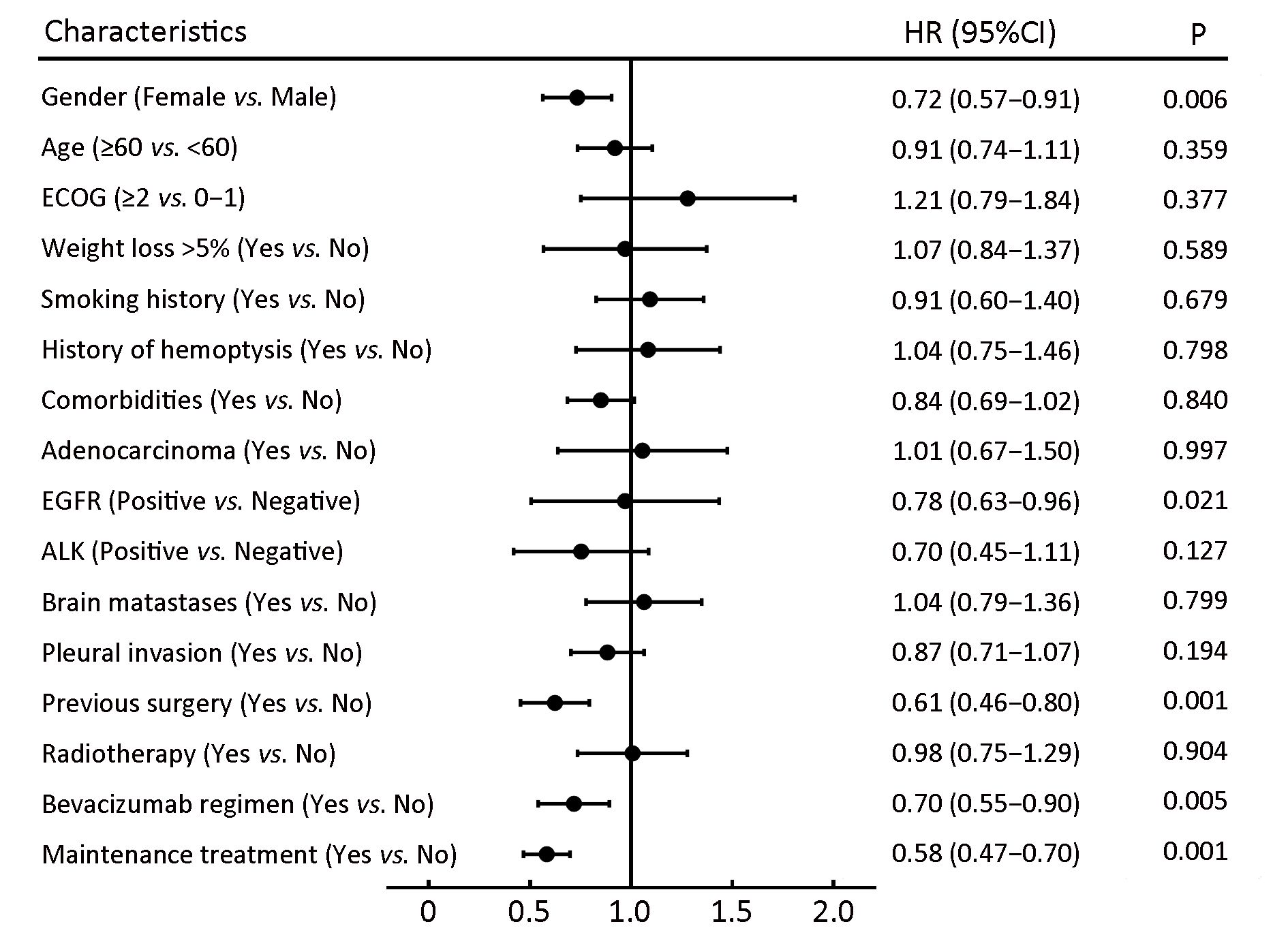
ObjectiveTo evaluate the efficacy and safety profile of first-line bevacizumab (Bev)-containing pemetrexed-platinum chemotherapy in a real-world Chinese cohort with advanced non-squamous non-small cell lung cancer (NS-NSCLC). MethodsA total of 415 eligible patients with NS-NSCLC who received first-line pemetrexed-platinum chemotherapy at National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College between February 2010 and September 2017 were reviewed retrospectively: 309 Bev(−) and 106 Bev(+) cases. Bev was administered at 7.5 mg/kg every 3 weeks in the Bev(+) group. To reduce the risk of a selection bias, a propensity score-matching (PSM) was conducted and 105 pairs of Bev(−) and Bev(+) cases were identified. ResultsThe median duration of follow-up was 15.8 months. The median progression-free survival (PFS) was prolonged significantly in the Bev(+) group than in the Bev(−) group in overall (9.8 vs. 7.8 months, P=0.006) and PSM pairs (9.8 vs. 6.6 months, P<0.001). Moreover, patients receiving maintenance therapy with pemetrexed plus Bev had longer PFS than those interrupted after induction chemotherapy, or those receiving mono-maintenance with pemetrexed (12.3 vs. 4.8 vs. 8.6 months; P<0.001). Multivariate analyses revealed Bev to be one of the favorable prognostic factors for PFS, along with the predictor of maintenance therapy. ConclusionsFirst-line induction and maintenance therapy with Bev (7.5 mg/kg every 3 weeks) combined with pemetrexed-platinum chemotherapy was efficacious and superior to non-Bev chemotherapy in Chinese patients with advanced NS-NSCLC.

2019, 31(5): 759-770.
doi: 10.21147/j.issn.1000-9604.2019.05.06
Abstract:
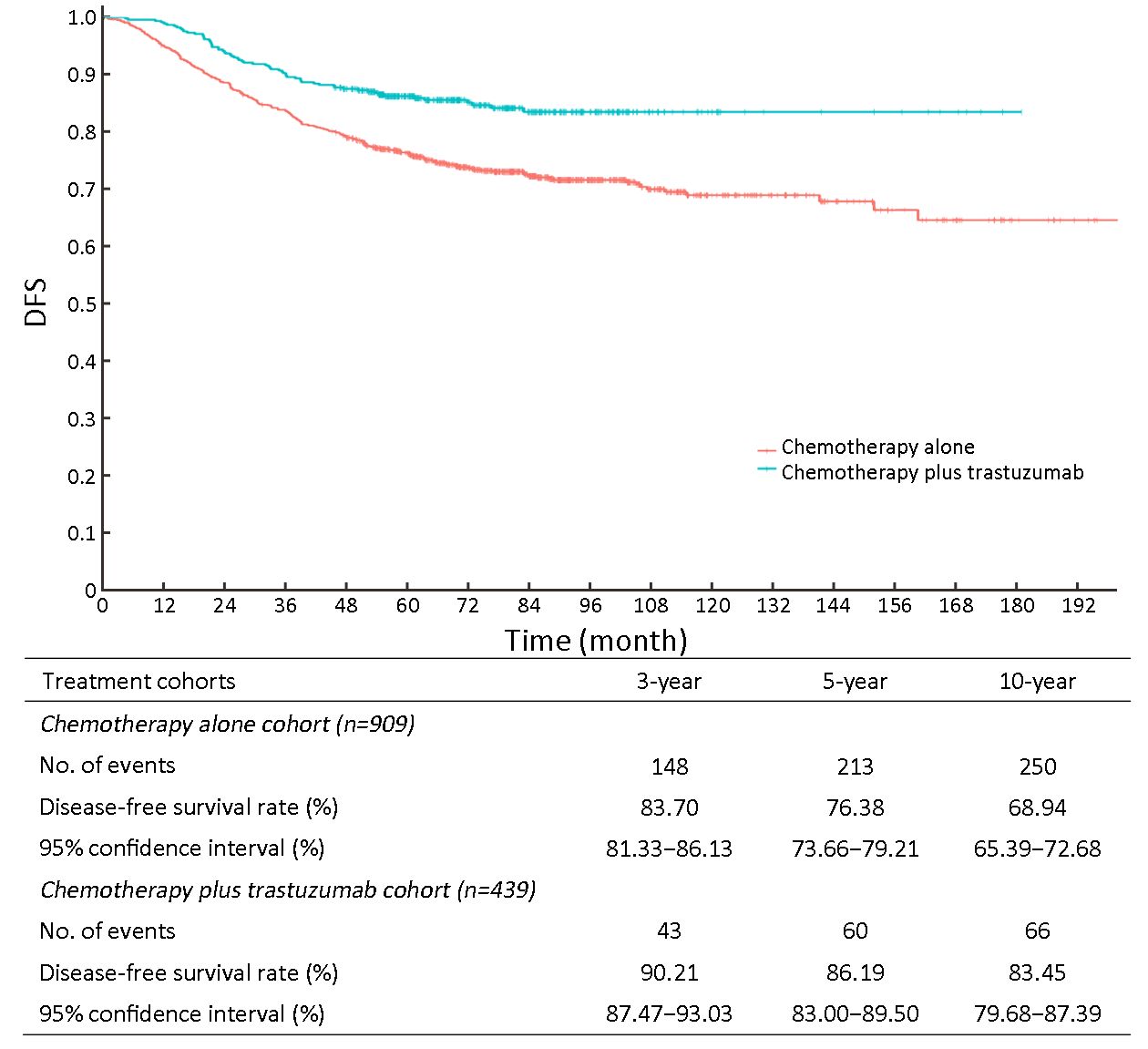
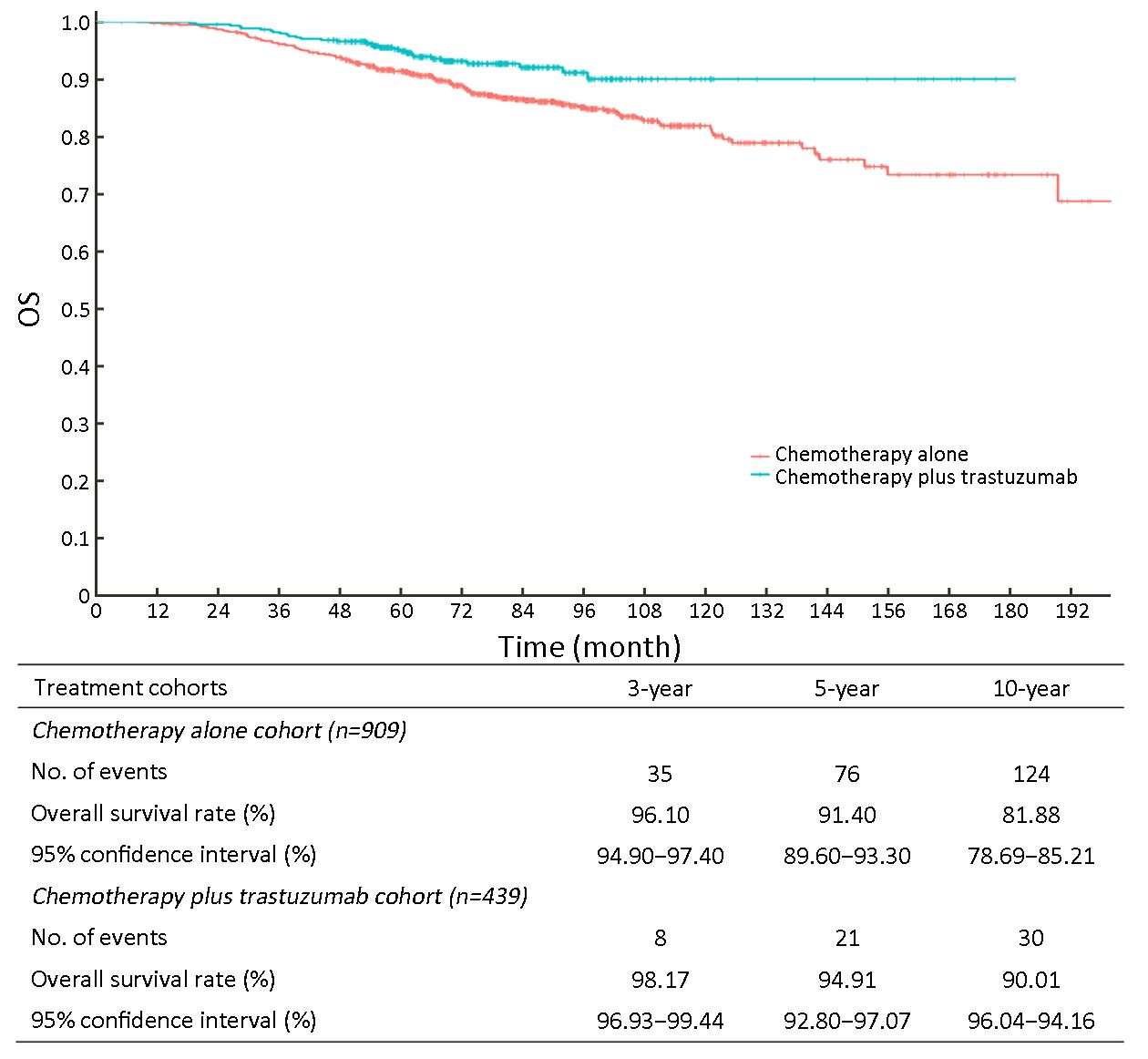
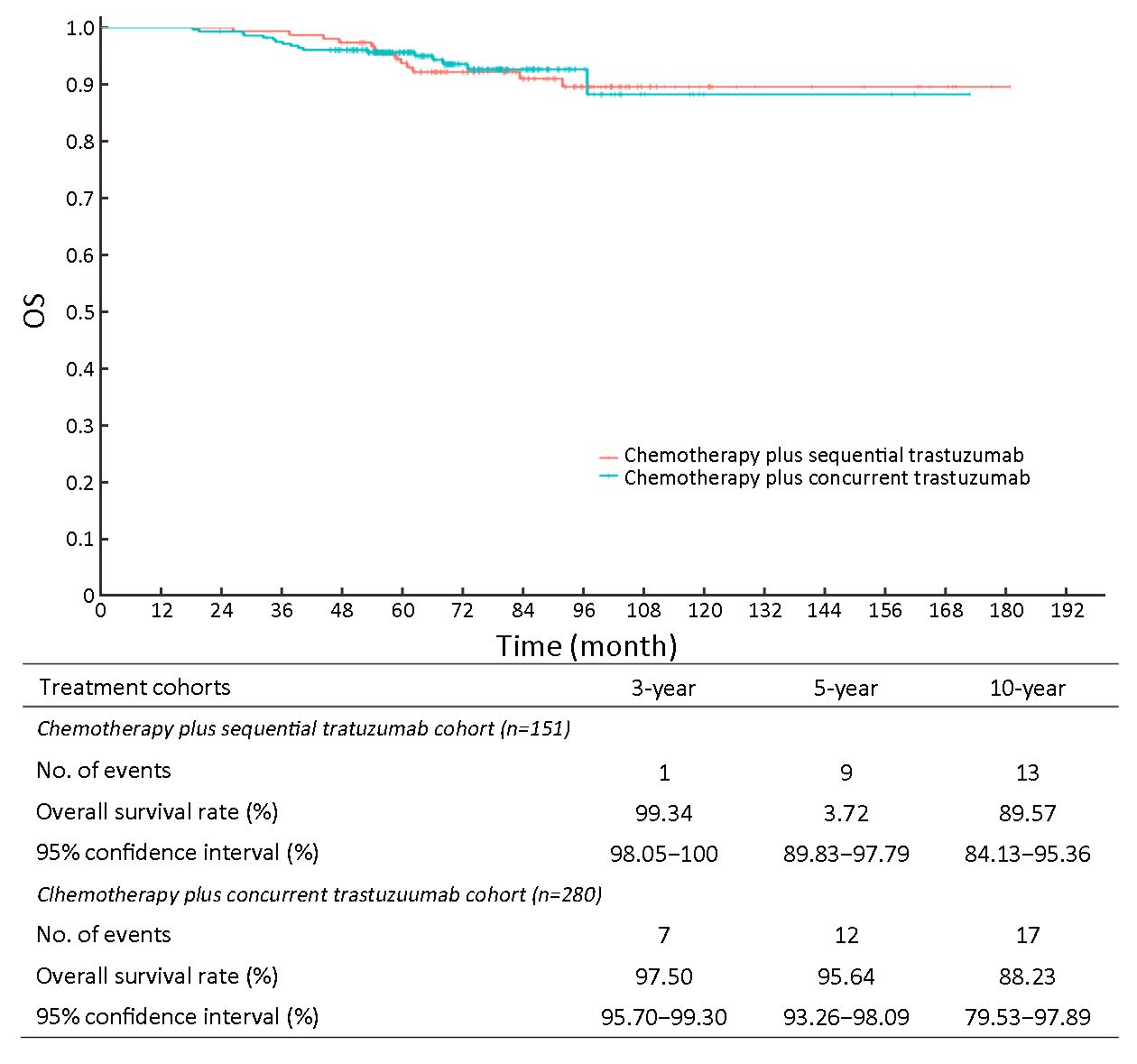
ObjectiveTo assess the long-term effectiveness and safety of trastuzumab in adjuvant therapy for Chinese patients with early-stage human epidermal growth factor 2 (HER2)-positive breast cancer in a real-world setting. MethodsThis retrospective observational study analyzed the medical records of HER2-positive breast cancer patients between 2000 and 2012 at the Chinese Academy of Medical Sciences. Patients who received adjuvant chemotherapy alone or adjuvant chemotherapy followed by/combined with trastuzumab were included. The Kaplan-Meier method was used to estimate disease-free survival (DFS) and overall survival (OS). Hazard ratios (HR) and 95% confidence intervals (95% CI) were calculated using the Cox regression model. ResultsOf the 1,348 patients analyzed, 909 received chemotherapy alone and 439 received chemotherapy plus trastuzumab. The 3-year, 5-year and 10-year DFS rates were 83.70%, 76.38% and 68.94%, respectively, in the chemotherapy-alone cohort, and 90.21%, 86.19% and 83.45% in the chemotherapy plus trastuzumab cohort. The 3-year, 5-year and 10-year OS rates were 96.10%, 91.40% and 81.88% in the chemotherapy-alone cohort, and 98.17%, 94.91% and 90.01% in the chemotherapy plus trastuzumab cohort. The chemotherapy plus trastuzumab group had a significantly lower risk of disease recurrence and death than the chemotherapy-alone group (DFS: HR=0.50, 95% CI, 0.37−0.68; P<0.001; OS: HR=0.53, 95% CI, 0.34−0.81; P=0.004) after adjusting for covariates. In the 439 patients treated with trastuzumab, multivariate analysis suggested that lymph node positivity, higher T stages, and hormone receptor-negative status were significantly associated with higher risks of disease recurrence, and lymph node positivity and hormone receptor-negative status were significantly associated with higher risks of death. Grade 3/4 adverse events (incidence ≥1%) were more common in patients receiving trastuzumab (54.44% vs. 15.73%). ConclusionsEarly-stage HER2-positive breast cancer patients treated with trastuzumab plus adjuvant chemotherapy have a significant survival benefit compared with chemotherapy-alone in real-world settings. Lymph node positivity, hormone receptor-negative status, and higher T stages may be associated with higher risks of recurrence, and effective therapy for patients with these factors is required.

2019, 31(5): 771-784.
doi: 10.21147/j.issn.1000-9604.2019.05.07
Abstract:
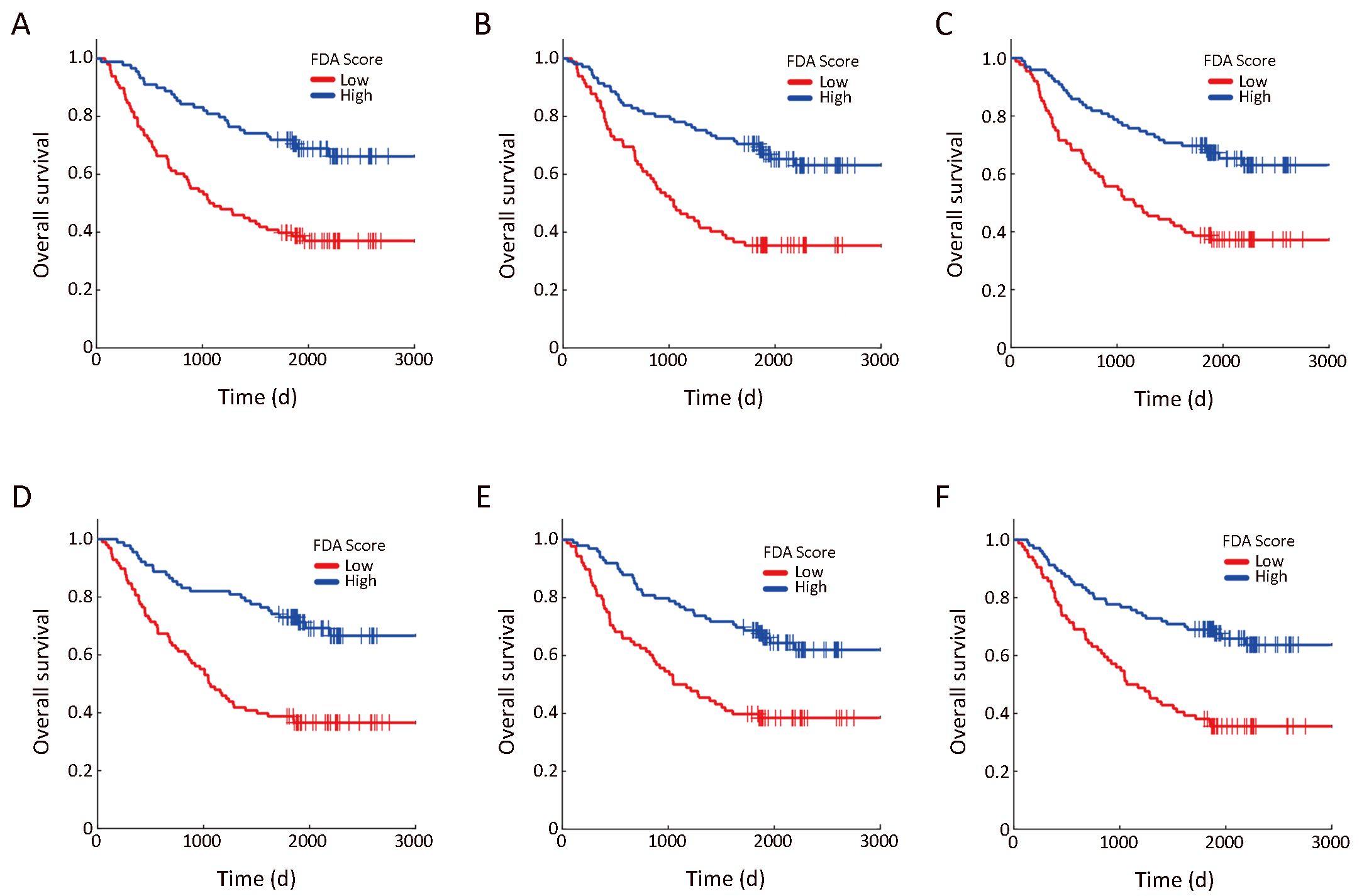
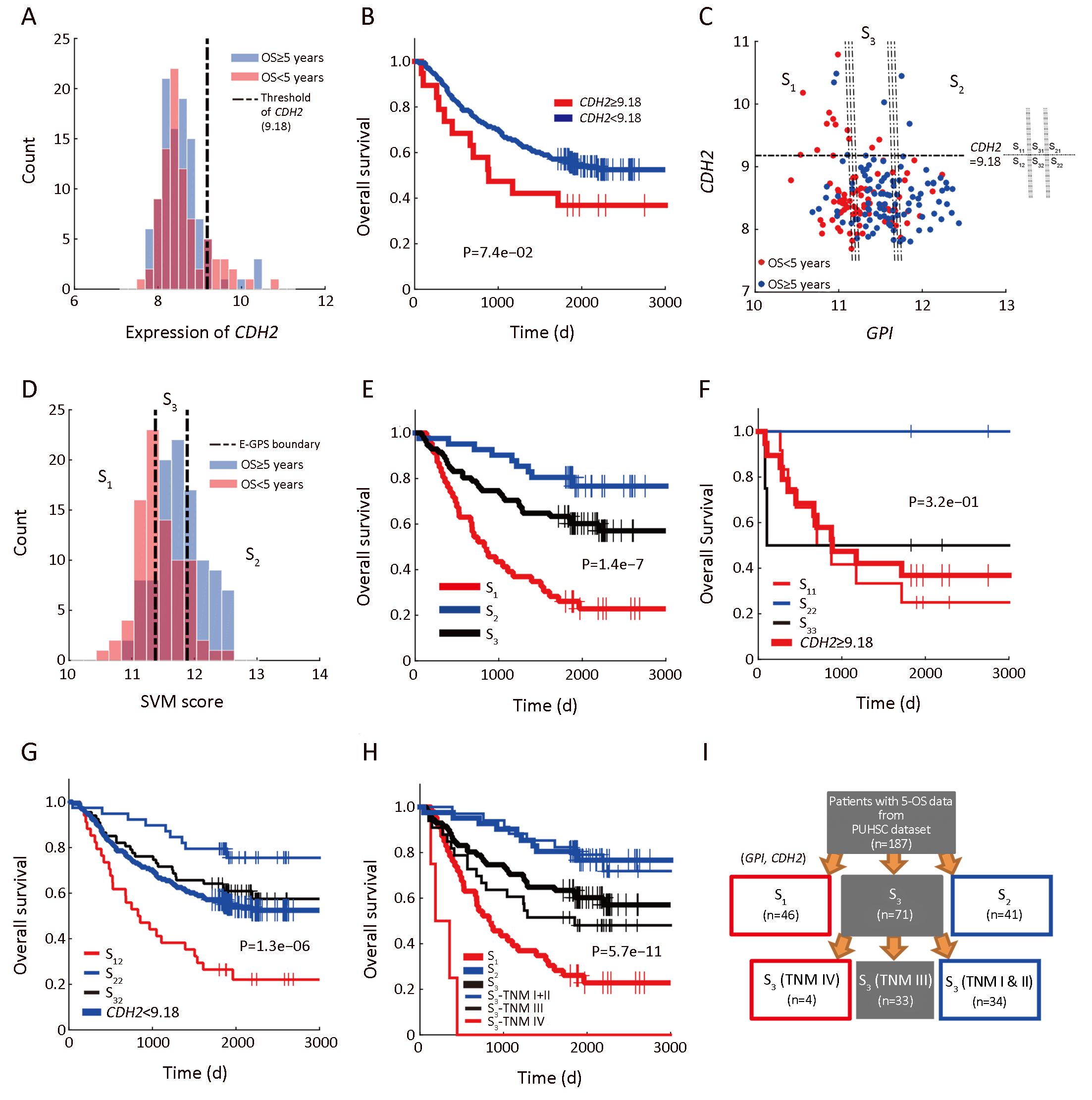
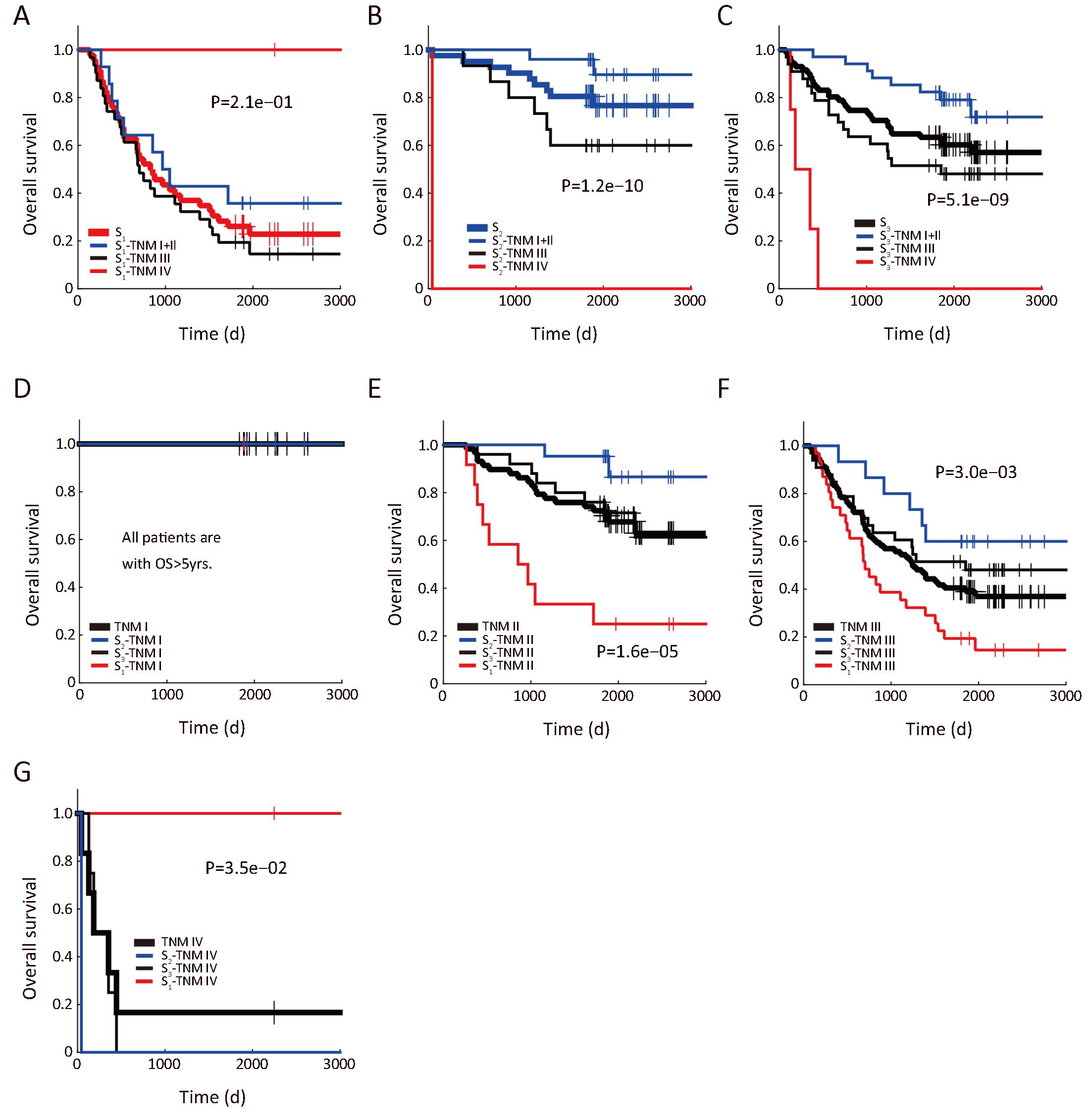
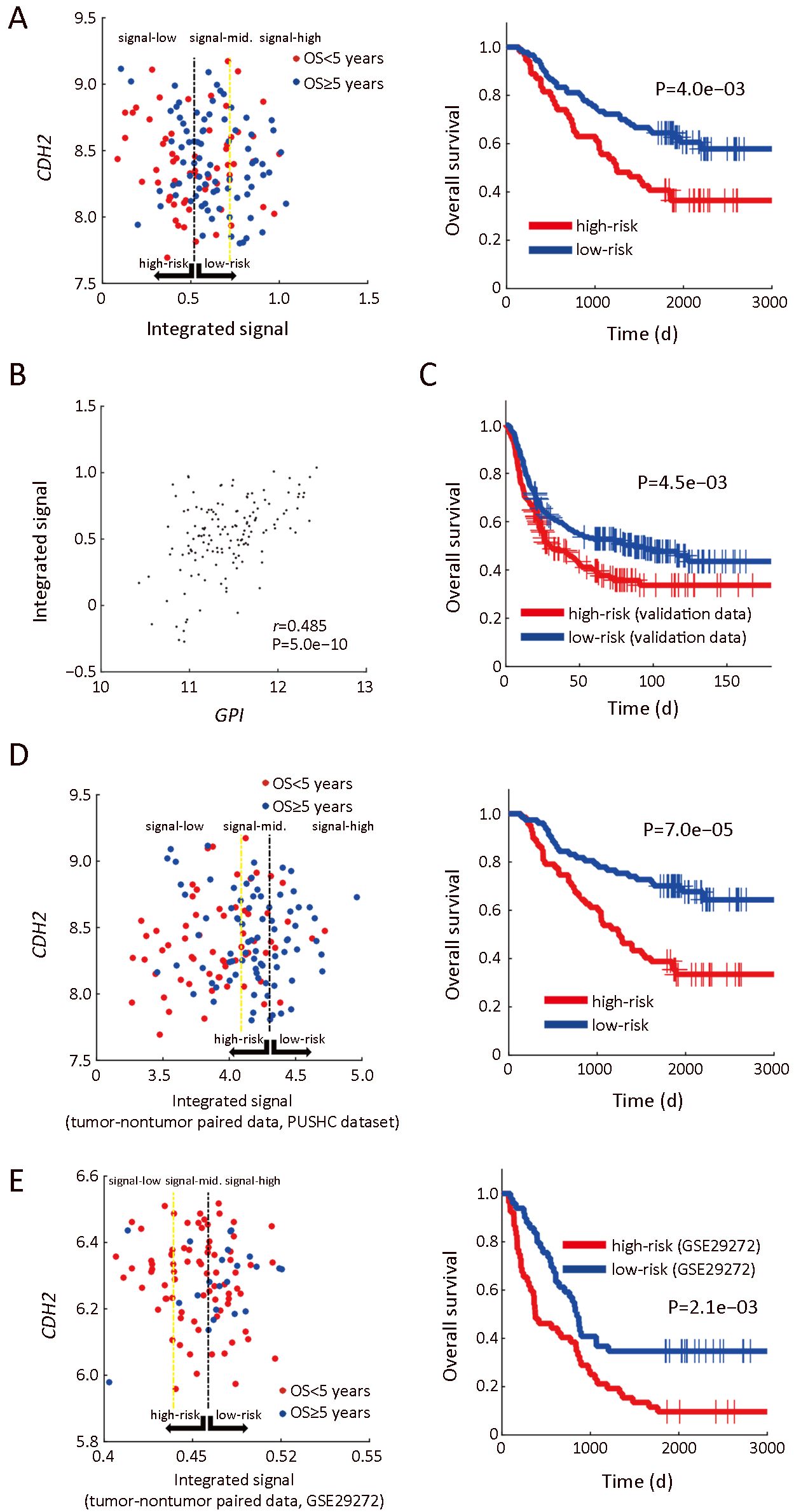
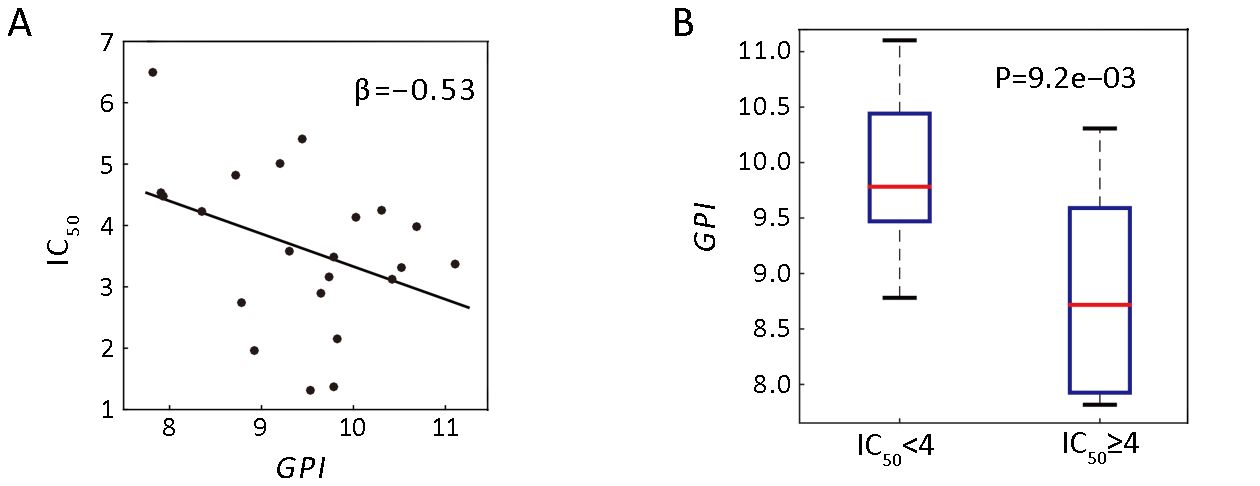
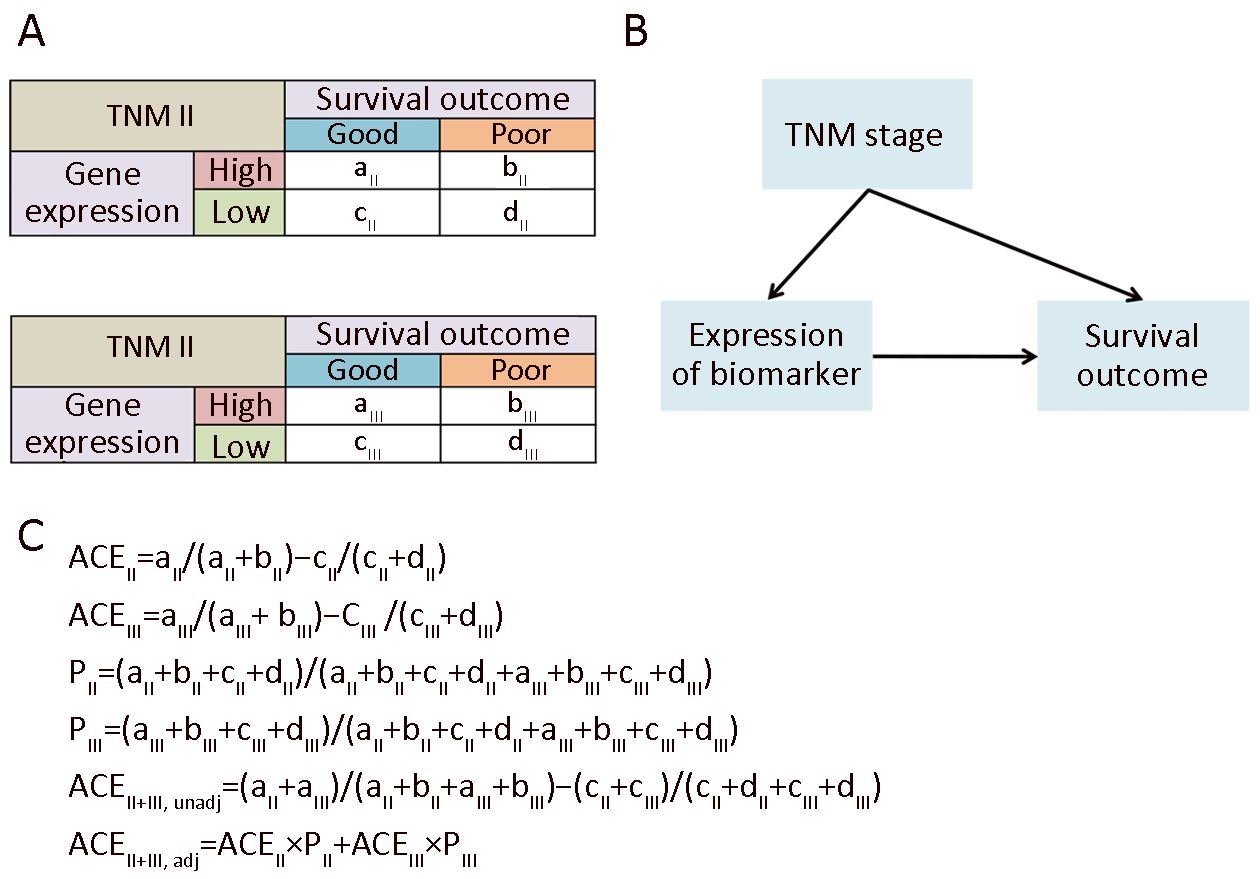
ObjectiveTumor heterogeneity renders identification of suitable biomarkers of gastric cancer (GC) challenging. Here, we aimed to identify prognostic genes of GC using computational analysis. MethodsWe first used microarray technology to profile gene expression of GC and paired nontumor tissues from 198 patients. Based on these profiles and patients’ clinical information, we next identified prognostic genes using novel computational approaches. Phosphoglucose isomerase, also known as glucose-6-phosphate isomerase (GPI), which ranked first among 27 candidate genes, was further investigated by a new analytical tool namely enviro-geno-pheno-state (E-GPS) analysis. Suitability of GPI as a prognostic marker, and its relationship with physiological processes such as metabolism, epithelial-mesenchymal transition (EMT), as well as drug sensitivity were evaluated using both our own and independent public datasets. ResultsWe found that higher expression of GPI in GC correlated with prolonged survival of patients. Particularly, a combination of CDH2 and GPI expression effectively stratified the outcomes of patients with TNM stage II/III. Down-regulation of GPI in tumor tissues correlated well with depressed glucose metabolism and fatty acid synthesis, as well as enhanced fatty acid oxidation and creatine metabolism, indicating that GPI represents a suitable marker for increased probability of EMT in GC cells. ConclusionsOur findings strongly suggest that GPI acts as a novel biomarker candidate for GC prognosis, allowing greatly enhanced clinical management of GC patients. The potential metabolic rewiring correlated with GPI also provides new insights into studying the relationship between cancer metabolism and patient survival.




2019, 31(5): 785-796.
doi: 10.21147/j.issn.1000-9604.2019.05.08
Abstract:
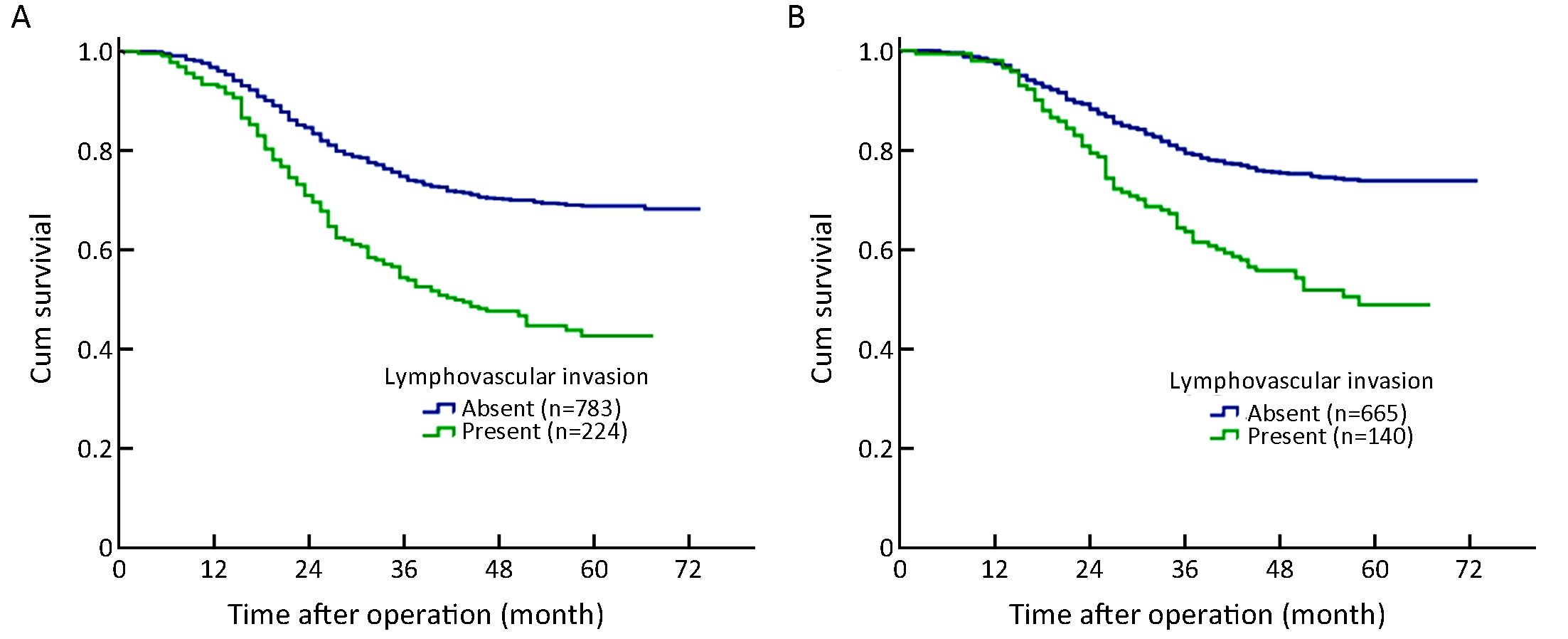
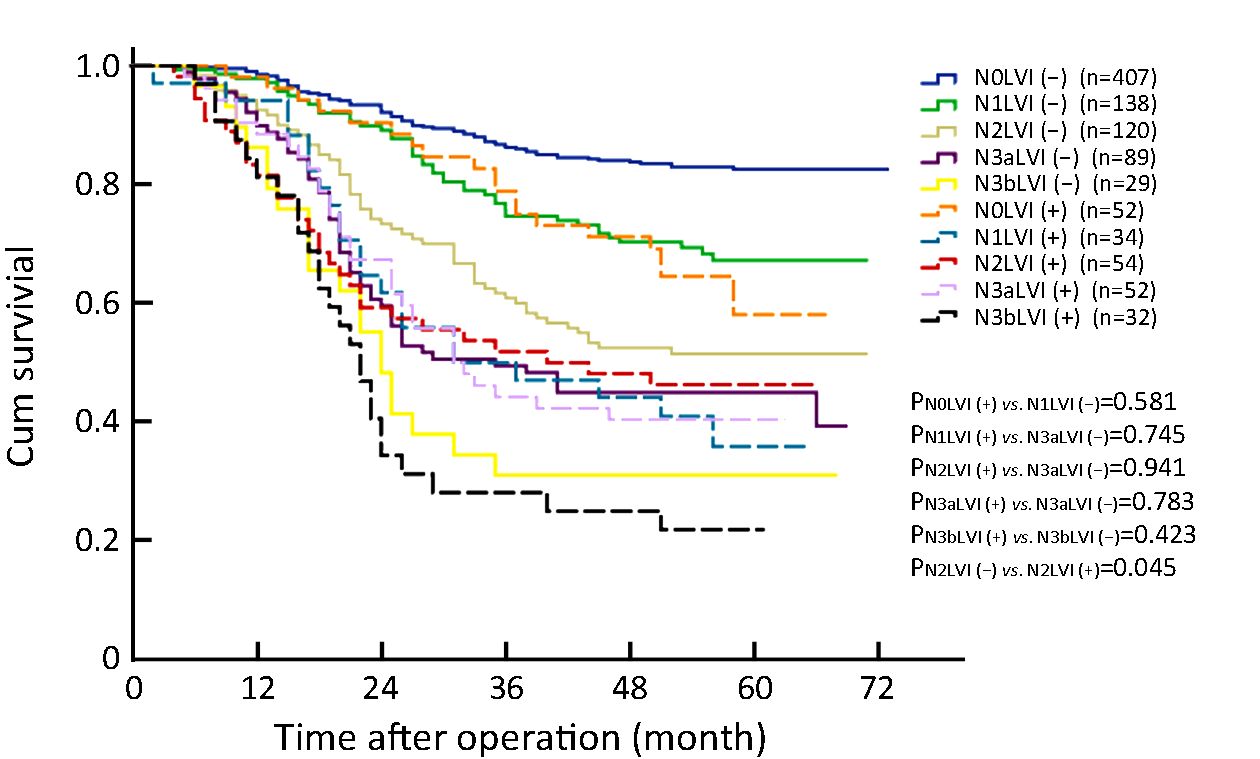
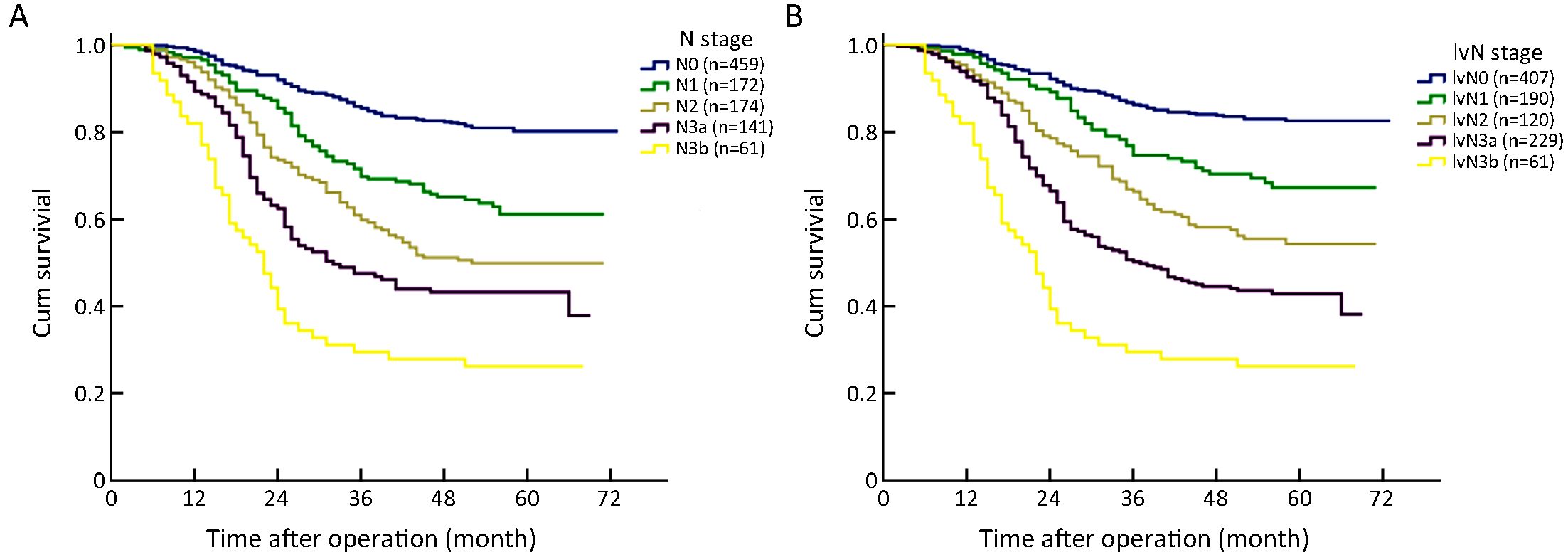
ObjectiveLymphovascular infiltration (LVI) is frequently detected in gastric cancer (GC) specimens. Studies have revealed that GC patients with LVI have a poorer prognosis than those without LVI. MethodsIn total, 1,007 patients with curatively resected GC at Department of Gastric Cancer, Tianjin Medical University Cancer Institute and Hospital were retrospectively enrolled. The patients were categorized into two groups based on the LVI status: a positive group (PG; presence of LVI) and a negative group (NG; absence of LVI). The clinicopathological factors corrected with LVI and prognostic variables were analyzed. Additionally, a pathological lymphovascular-node (lvN) classification system was proposed to evaluate the superiority of its prognostic prediction of GC patients compared with that of the eighth edition of the N staging system. ResultsTwo hundred twenty-four patients (22.2%) had LVI. The depth of invasion and lymph node metastasis were independently associated with the presence of LVI. GC patients with LVI demonstrated a significantly lower overall survival (OS) rate than those without LVI (42.8% vs. 68.9%, respectively; P<0.001). In multivariate analysis, LVI was identified as an independent prognostic factor for GC patients (hazard ratio: 1.370; 95% confidence interval: 1.094−1.717; P=0.006). Using strata analysis, significant prognostic differences between the groups were only observed in patients at stage I−IIIa or N0−2. The lvN classification was found to be more appropriate to predict the OS of GC patients after curative surgery than the pN staging system. The −2 log-likelihood of lvN classification (4,746.922) was smaller than the value of pN (4,765.196), and the difference was statistically significant (χ2=18.434, P<0.001). ConclusionsThe presence of LVI influences the OS of GC patients at stage I−IIIa or N0−2. LVI should be incorporated into the pN staging system to enhance the accuracy of the prognostic prediction of GC patients.
2019, 31(5): 797-805.
doi: 10.21147/j.issn.1000-9604.2019.05.09
Abstract:
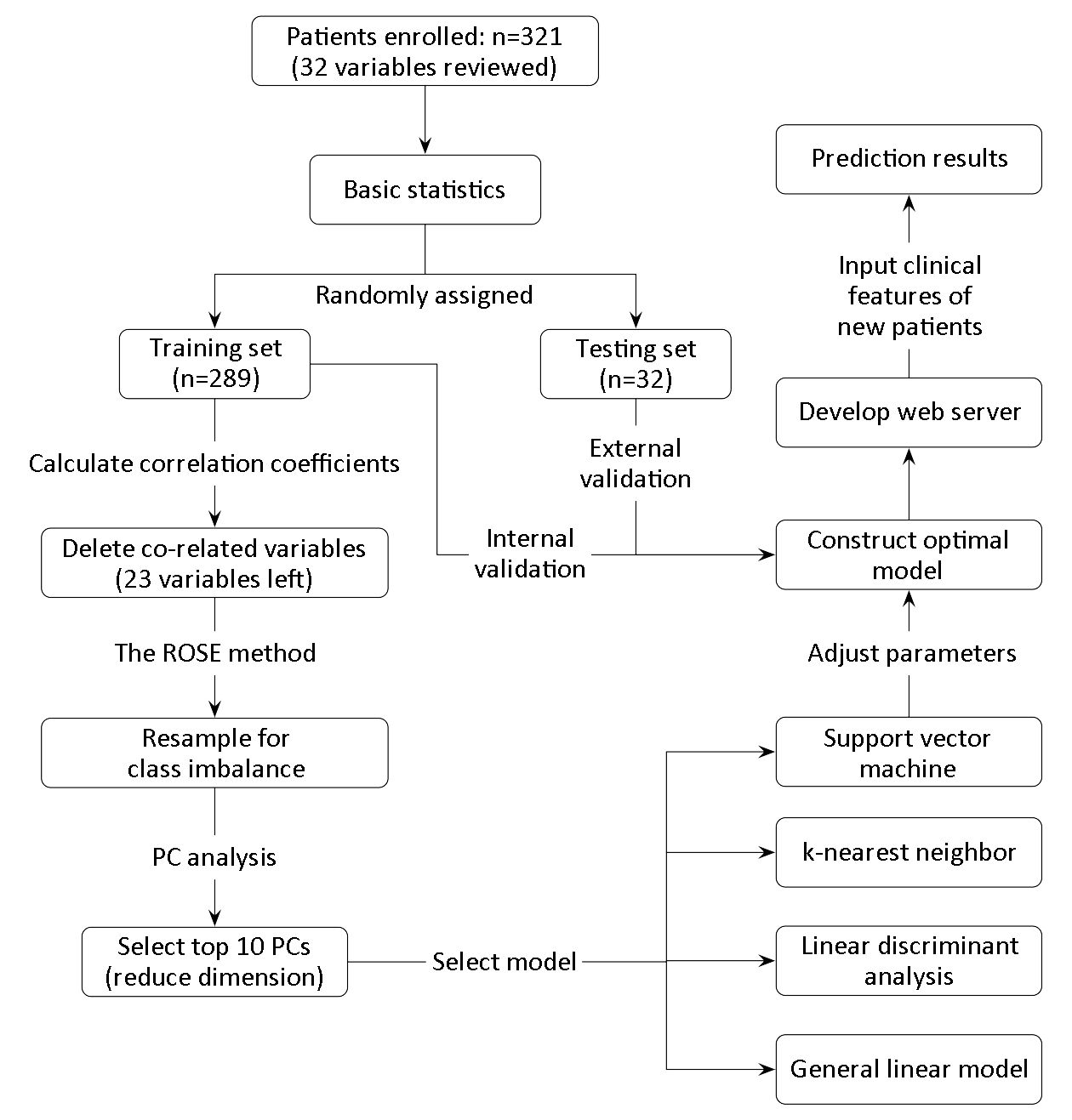
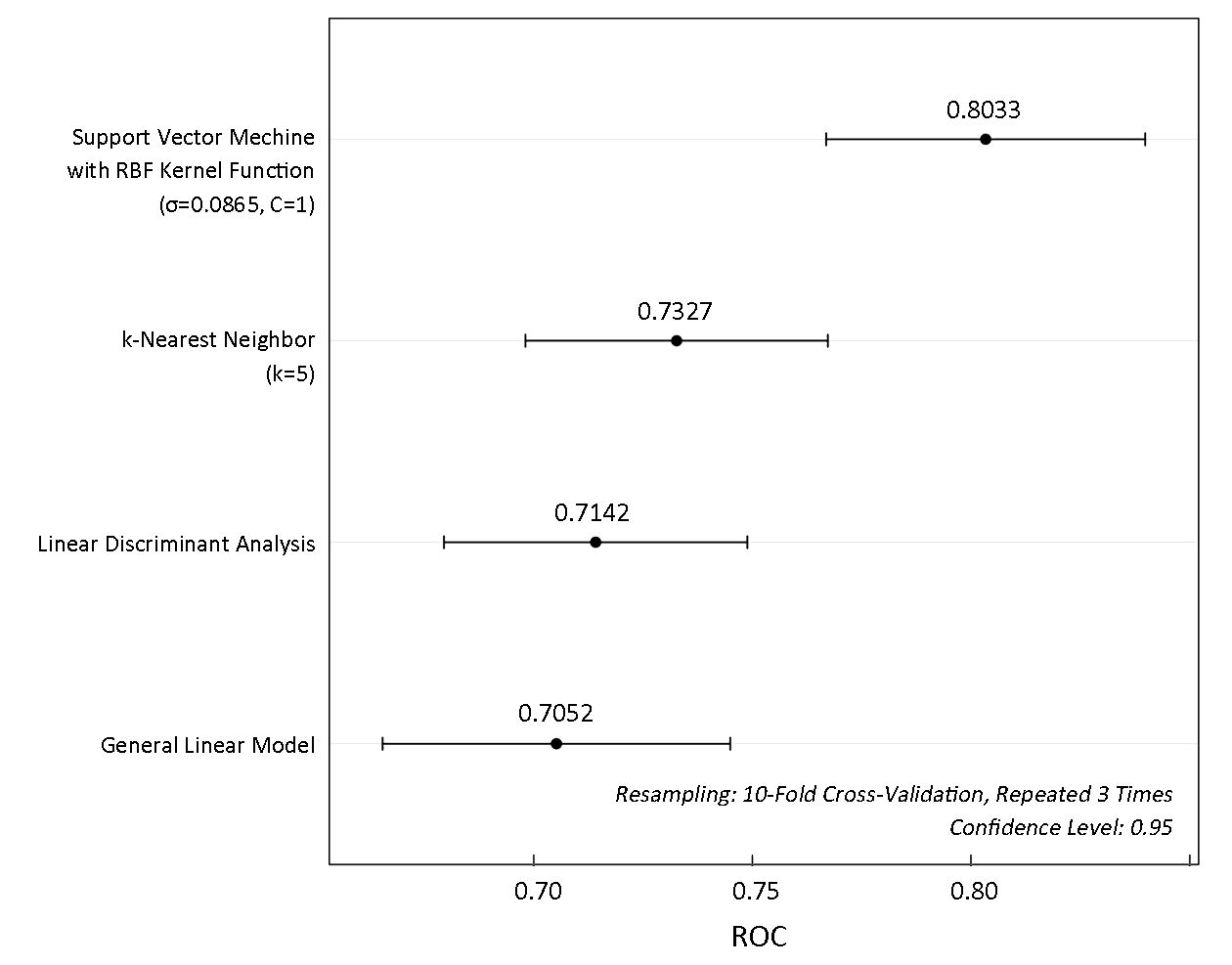
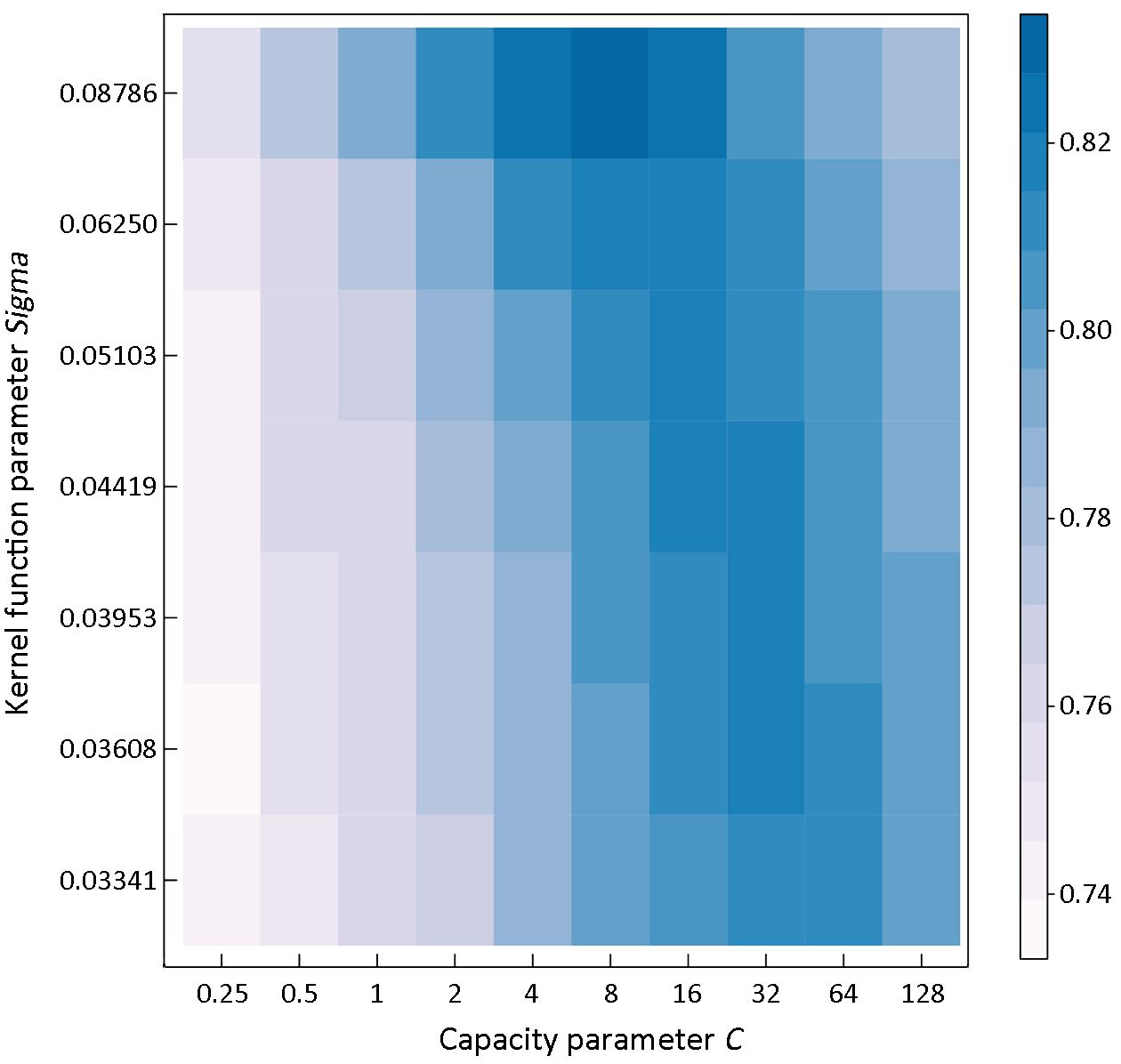
Objective Postoperative complications adversely affected the prognosis in patients with gastric cancer. This study intends to investigate the feasibility of using machine-learning model to predict surgical outcomes in patients undergoing gastrectomy. Methods In this study, cancer patients who underwent gastrectomy at Shanghai Rui Jin Hospital in 2017 were randomly assigned to a development or validation cohort in a 9:1 ratio. A support vector classification (SVC) model to predict surgical outcomes in patients undergoing gastrectomy was developed and further validated. Results A total of 321 patients with 32 features were collected. The positive and negative outcomes of postoperative complication after gastrectomy appeared in 100 (31.2%) and 221 (68.8%) patients, respectively. The SVC model was constructed to predict surgical outcomes in patients undergoing gastrectomy. The accuracy of 10-fold cross validation and external verification was 78.17% and 78.12%, respectively. Further, an online web server has been developed to share the SVC model for machine-learning-assisted prediction of surgical outcomes in patients undergoing gastrectomy in the future procedures, which is accessible at the web address: http://47.100.47.97:5005/r_model_prediction. Conclusions The SVC model was a useful predictor for measuring the risk of postoperative complications after gastrectomy, which may help stratify patients with different overall status for choice of surgical procedure or other treatments. It can be expected that machine-learning models in cancer informatics research are possibly shareable and accessible via web address all over the world.


2019, 31(5): 806-817.
doi: 10.21147/j.issn.1000-9604.2019.05.10
Abstract:
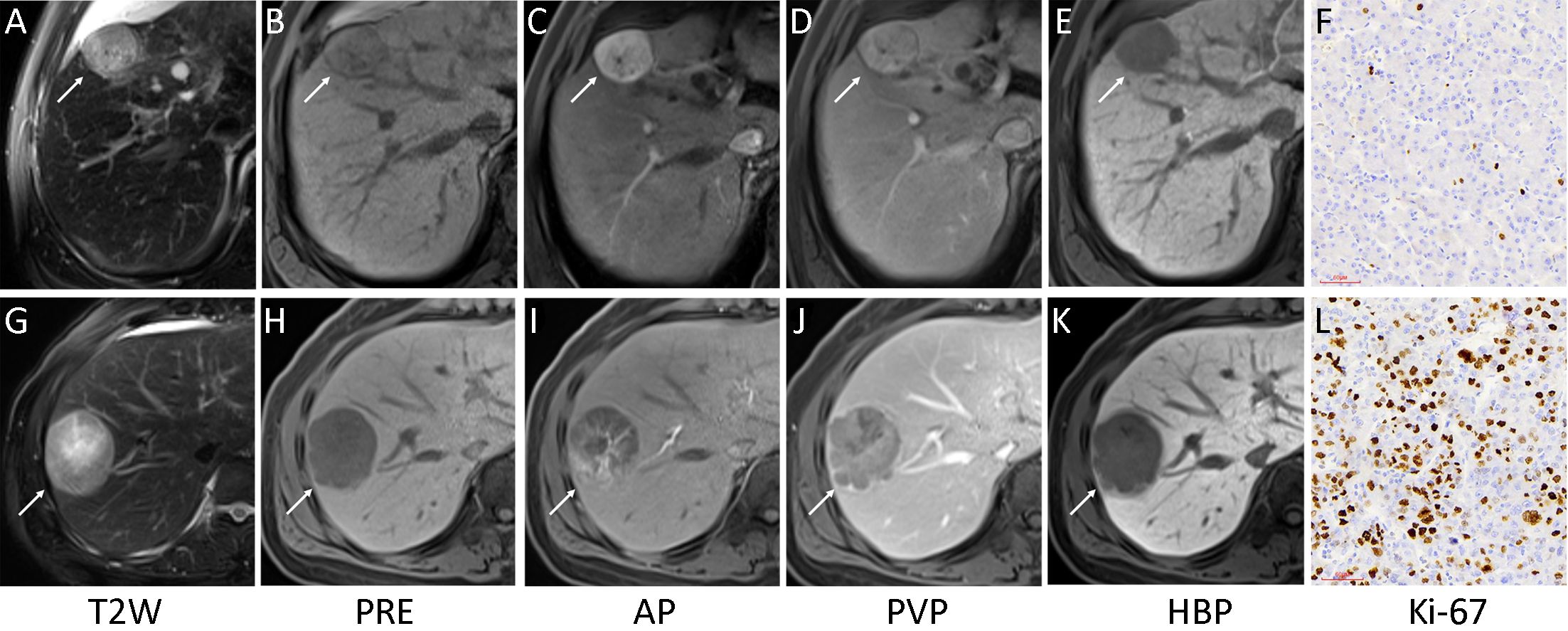
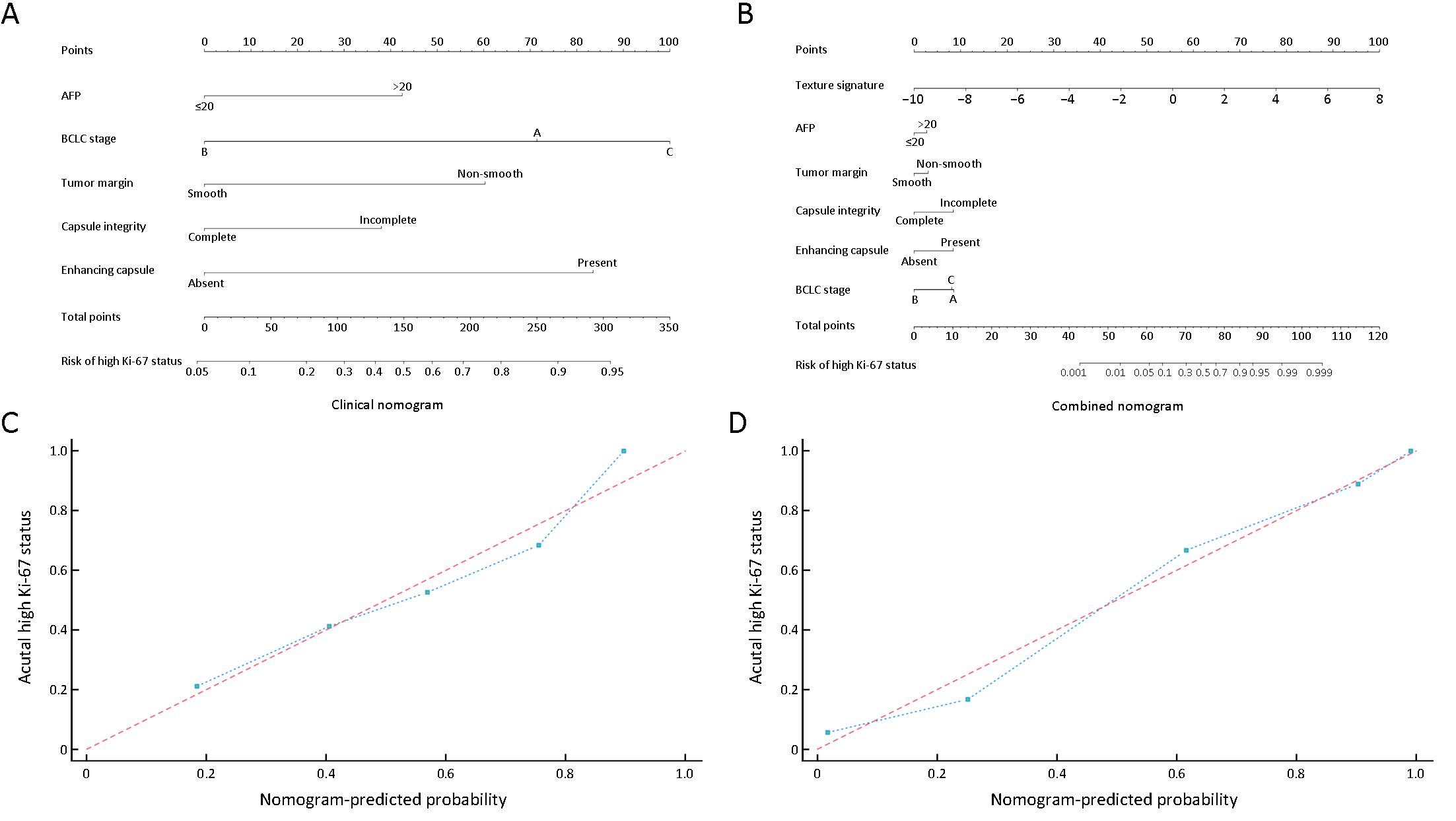
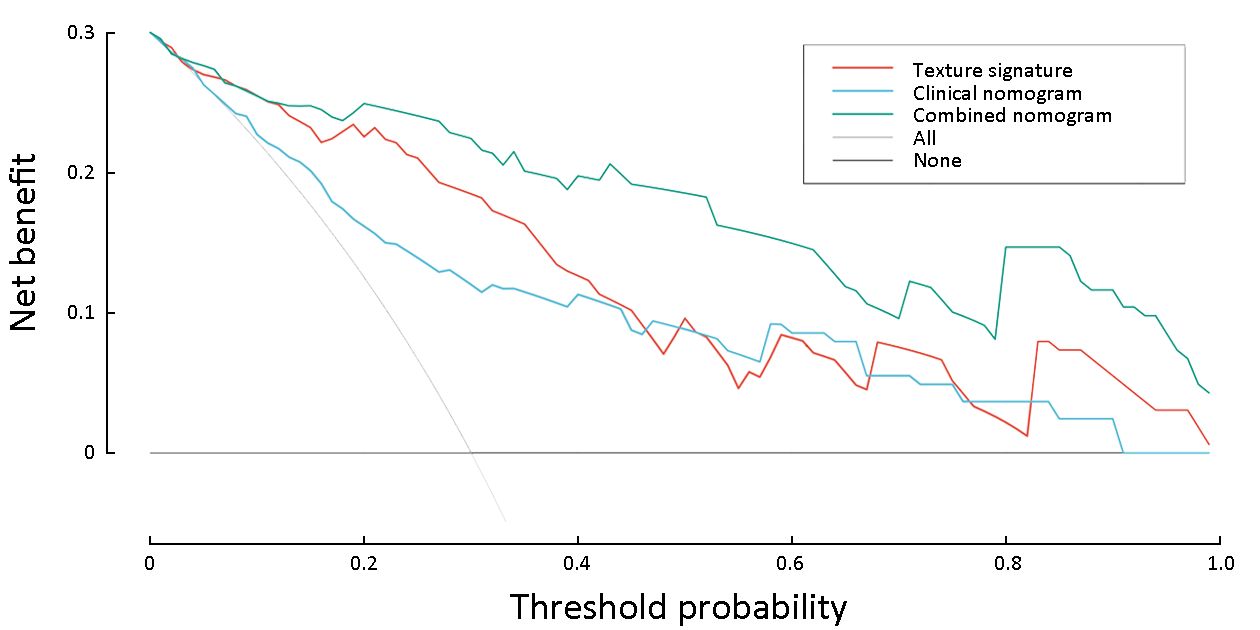
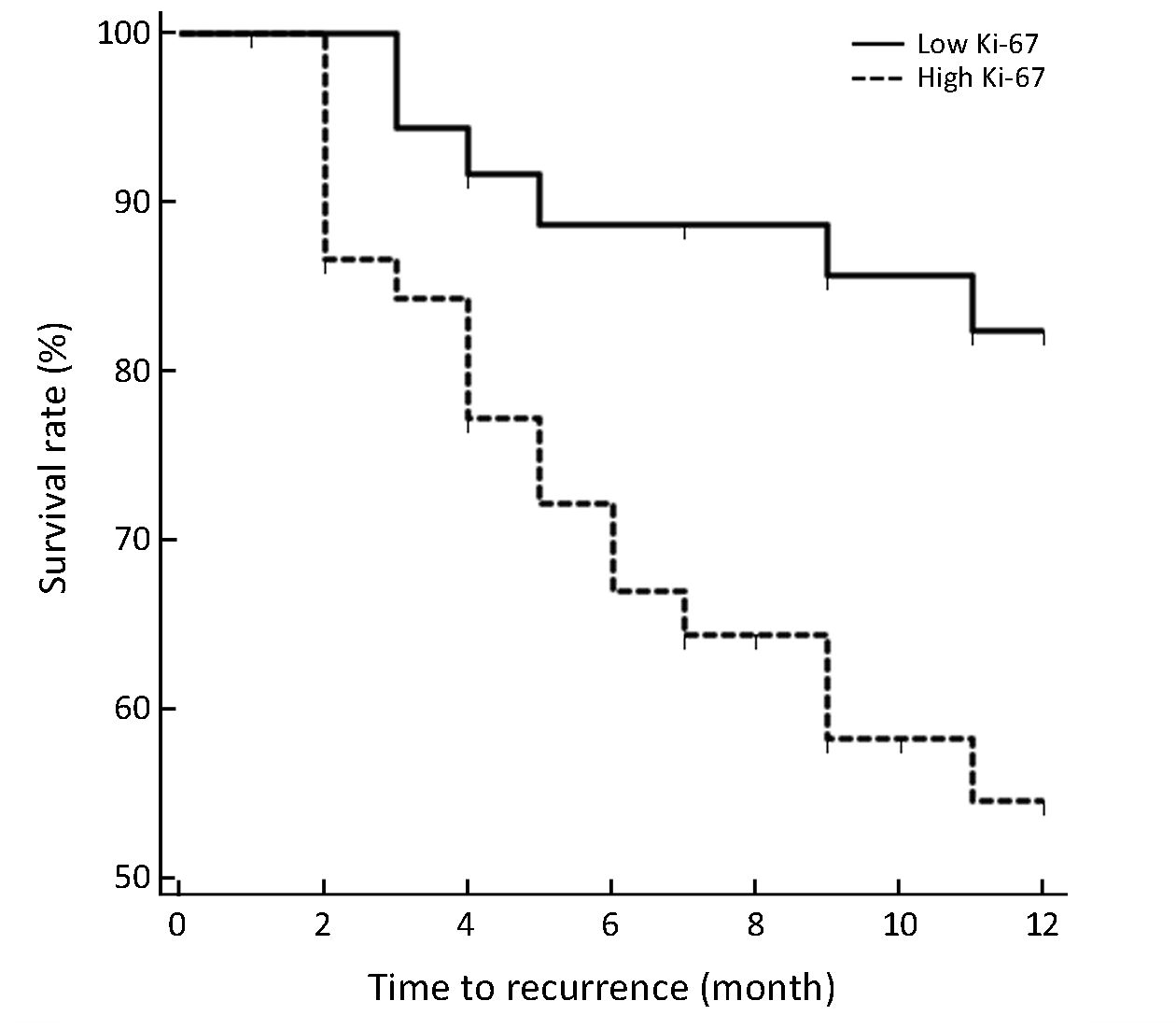
Objective To investigate the value of whole-lesion texture analysis on preoperative gadoxetic acid enhanced magnetic resonance imaging (MRI) for predicting tumor Ki-67 status after curative resection in patients with hepatocellular carcinoma (HCC). Methods This study consisted of 89 consecutive patients with surgically confirmed HCC. Texture features were extracted from multiparametric MRI based on whole-lesion regions of interest. The Ki-67 status was immunohistochemical determined and classified into low Ki-67 (labeling index ≤15%) and high Ki-67 (labeling index >15%) groups. Least absolute shrinkage and selection operator (LASSO) and multivariate logistic regression were applied for generating the texture signature, clinical nomogram and combined nomogram. The discrimination power, calibration and clinical usefulness of the three models were evaluated accordingly. Recurrence-free survival (RFS) rates after curative hepatectomy were also compared between groups. Results A total of 13 texture features were selected to construct a texture signature for predicting Ki-67 status in HCC patients (C-index: 0.878, 95% confidence interval: 0.791−0.937). After incorporating texture signature to the clinical nomogram which included significant clinical variates (AFP, BCLC-stage, capsule integrity, tumor margin, enhancing capsule), the combined nomogram showed higher discrimination ability (C-index: 0.936 vs. 0.795, P<0.001), good calibration (P>0.05 in Hosmer-Lemeshow test) and higher clinical usefulness by decision curve analysis. RFS rate was significantly lower in the high Ki-67 group compared with the low Ki-67 group after curative surgery (63.27% vs. 85.00%, P<0.05). Conclusions Texture analysis on gadoxetic acid enhanced MRI can serve as a noninvasive approach to preoperatively predict Ki-67 status of HCC after curative resection. The combination of texture signature and clinical factors demonstrated the potential to further improve the prediction performance.

2019, 31(5): 818-824.
doi: 10.21147/j.issn.1000-9604.2019.05.11
Abstract:
ObjectiveHand-assisted laparoscopic liver resection has the advantages of open and laparoscopic surgeries. There is still lack of comparison of surgical outcomes between hand-assistied laparoscopic liver resection (HALLR) and open liver resection (OLR). This study compared the surgical outcomes of the two approaches between well-matched patient cohorts. MethodsPatients who received liver resection during January 2014 and October 2017 in Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College were included in this retrospective study. Propensity score matching (PSM) was performed to reduce selection bias between the two groups. Operation and short-term surgical outcomes were compared between the well matched groups. ResultsDuring this period, 232 patients with a median age of 55.1 years old received OLR, while 49 patients with a median age of 54.7 years old received HALLR. Compared with HALLR group, OLR group has a higher proportion in male patients (190/232, 81.9% vs. 34/49, 69.4%, P=0.048) and lower albumin (43.2±4.5 vs. 44.8±3.7, P=0.020). After PSM, 49 patients from each group were included in the following analysis. Two groups were well balanced in their baseline characteristics, liver functions, preoperative treatments, abdominal surgery history, and surgical difficulty. None perioperative mortality was observed in both groups. Operation time and postoperative complications were similar in two groups (P=0.935, P=0.056). The HALLR group showed less bleeding amount (177.8±217.1 mL vs. 283.1±225.0 mL, P=0.003) and shorter postoperative stay period (6.9±2.2 d vs. 9.0±3.5 d, P=0.001). ConclusionsWe demonstrated that hand-assisted laparoscopic surgery is feasible and safe for liver resection, including some difficult cases. HALLR can provide better bleeding control and faster recovery after surgery.
2019, 31(5): 825-837.
doi: 10.21147/j.issn.1000-9604.2019.05.12
Abstract:
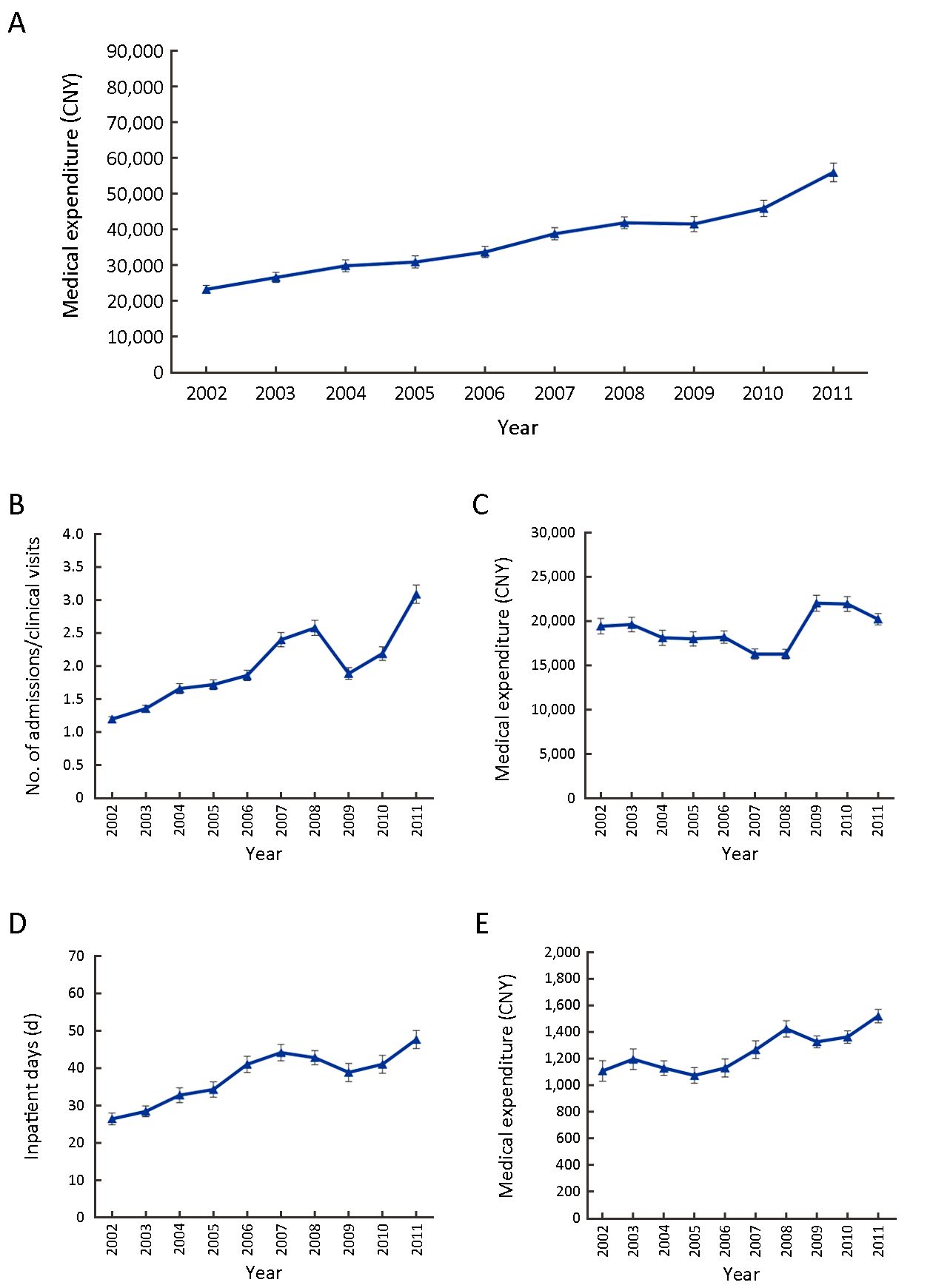
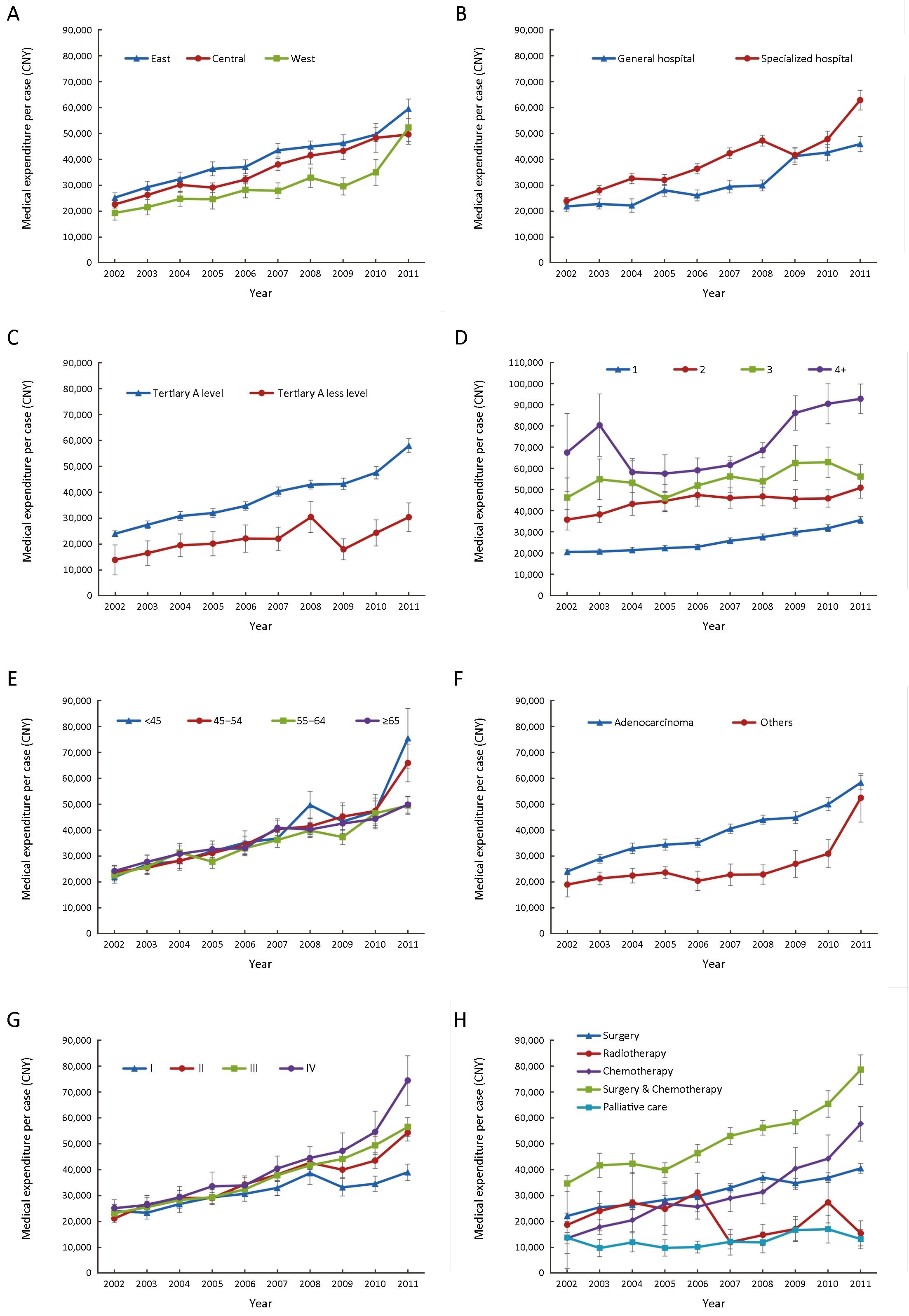
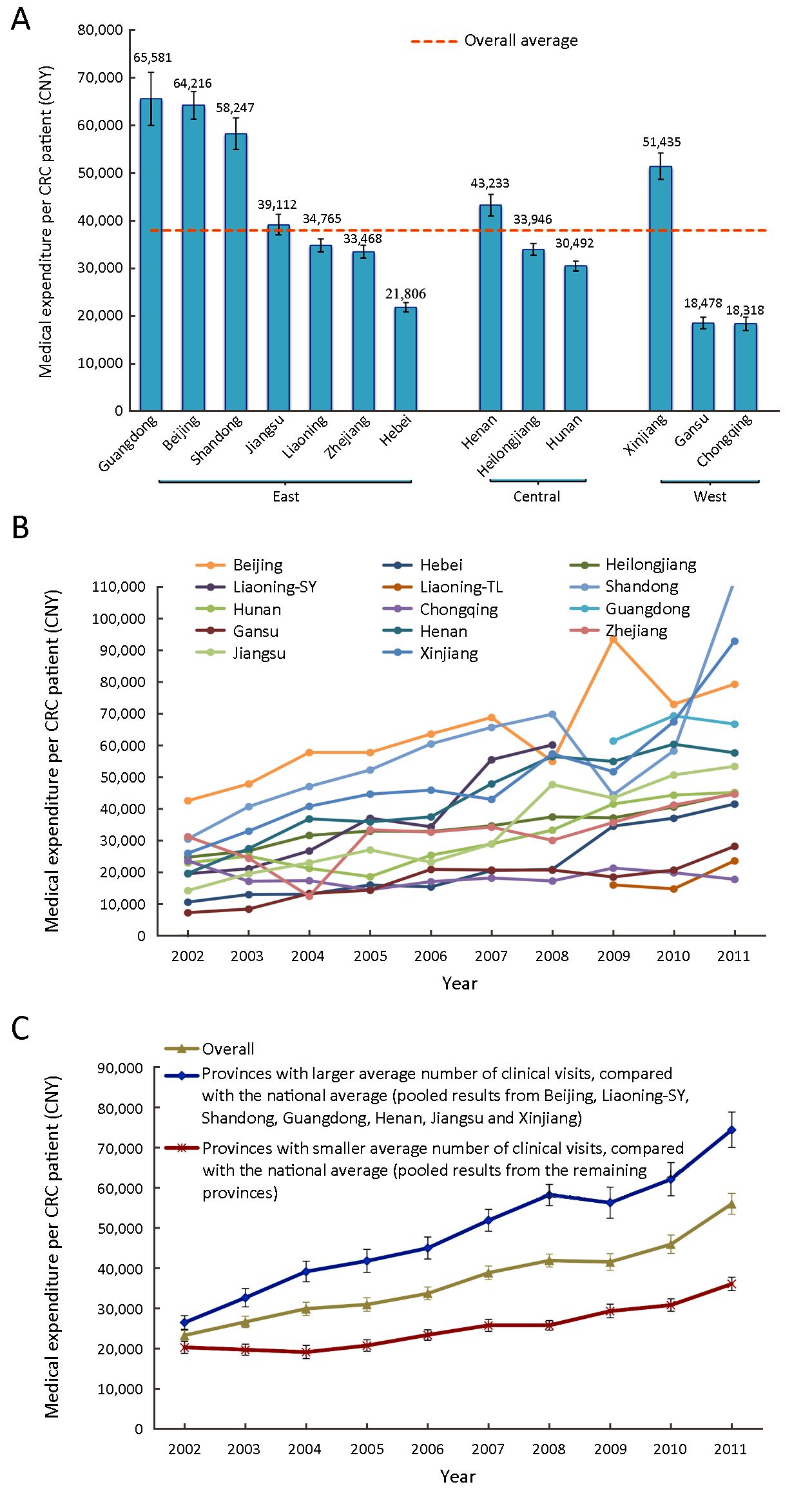
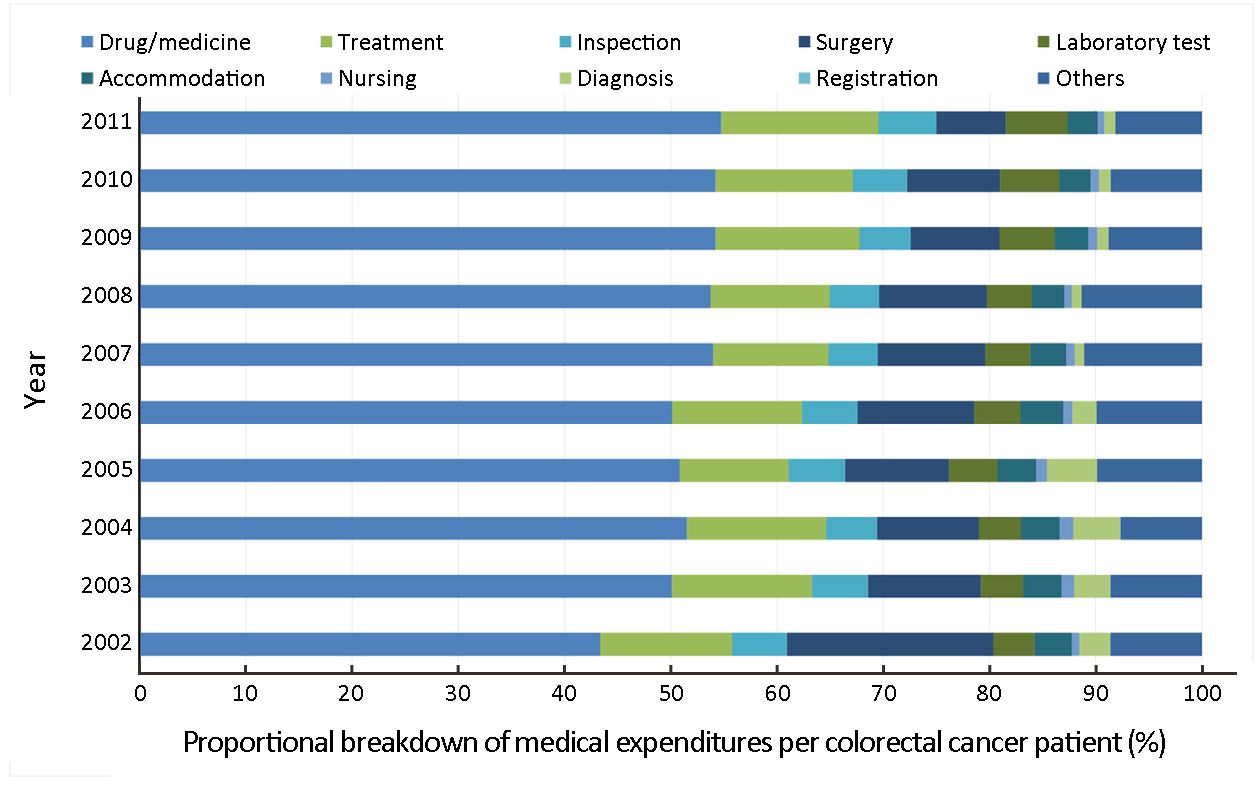
Objective Colorectal cancer (CRC) causes a substantial burden of disease in China and the evidence of economic burden triggered is fundamental for priority setting. The aim of this survey was to quantify medical expenditures and the time trends for CRC diagnosis and treatment in China. Methods From 2012 to 2014, a hospital-based multicenter retrospective survey was conducted in 13 provinces across China. For each eligible CRC patient diagnosed from 2002 to 2011, clinical information and expenditure data were extracted using a uniform questionnaire. All expenditure data were reported in Chinese Yuan (CNY) using 2011 values. Results Of the 14,536 CRC patients included, the average age at diagnosis was 58.2 years and 15.8% were stage-I cases. The average medical expenditure per patient was estimated at 37,902 CNY [95 % confidence interval (95% CI): 37,282−38,522], and the annual average increase rate was 9.2% from 2002 to 2011 (P for trend <0.001), with a cumulative increase of 2.4 times (from 23,275 CNY to 56,010 CNY). The expenditure per patient in stages I, II, III and IV were 31,698 CNY, 37,067 CNY, 38,918 CNY and 42,614 CNY, respectively (P<0.001). Expenditure significantly differed within various subgroups. Expenses for drugs contributed the largest proportion (52.6%). Conclusions These conservative estimates illustrated that medical expenditures for CRC diagnosis and treatment in tertiary hospitals in China were substantial and increased rapidly over the 10 years, with drugs continually being the main expense by 2011. Relatively, medical expenditures are lower for CRC in the earlier stages. These findings will facilitate the economic evaluation of CRC prevention and control in China.
2019, 31(5): 838-848.
doi: 10.21147/j.issn.1000-9604.2019.05.13
Abstract:
ObjectiveTo provide a decision-making basis for sustainable and effective development of cervical cancer screening. MethodsThis cross-sectional study assesses the service capacity to conduct cervical cancer screening with a sample of 310 medical staff, medical institutions and affiliated township health centers from 20 county-level/district-level areas in 14 Chinese provinces in 2016. ResultsThe county-level/district-level institutions were the main prescreening institutions for cervical cancer screening. More medical staff have become engaged in screening, with a significantly higher amounts in urban than in rural areas (P<0.05). The number of human papillomavirus (HPV) testers grew the fastest (by 225% in urban and 125% in rural areas) over the course of the project. HPV testing took less time than cytology to complete the same number of screening tasks in both urban and rural areas. The proportion of mid-level professionals was the highest among the medical staff, 40.0% in urban and 44.7% in rural areas (P=0.406), and most medical staff had a Bachelor’s degree, accounting for 76.3% in urban and 52.0% in rural areas (P<0.001). In urban areas, 75.0% were qualified medical staff, compared with 68.0% in rural areas, among which the lowest proportion was observed for rural cytology inspectors (22.7%). The medical equipment for cervical pathology diagnosis in urban areas was better (P<0.001). HPV testing equipment was relatively adequate (typing test equipment was 70% in urban areas, and non-typing testing equipment was 70% in rural areas). ConclusionsThe service capacity of cervical cancer screening is insufficient for the health needs of the Chinese population. HPV testing might be an optimal choice to fill the needs of cervical cancer screening given current Chinese medical health service capacity.


